Keywords
Bladder; Urethrovesical; Foreign body; Electric wire; Children
Introduction
Urethrovesical foreign body, though uncommon, can be seen in adolescents [1]. The major route for its implementation is via the urethral meatus and usually, it is self-insertion of different objects. Late presentation and hesitancy to report to a doctor are possible due to a feeling of embarrassment. It may also be due to iatrogenic causes or migration from medically installed materials i.e., catheters. The main site where the foreign bodies are found in the urethra and/or urinary bladder. Urethrovesical foreign bodies are encountered in both male and female patient [2]. There are few series that discuss this problem in the pediatric population. The most common motives associated with foreign bodies of the genitourinary tract are sexual or erotic in nature.
The late presentation may lead to calculus formation, diverticulum, urethral stricture and may be misdiagnosed. Iatrogenic intravesical foreign bodies may result from previous procedures such as urinary catheterization, suture, and migration from adjacent organs such as intrauterine devices or from the digestive tract. Patients may present with variable symptoms such as recurrent UTI, urinary incontinence, pelvic pain, or gross hematuria. A complete evaluation of the patients suspected to have intravesical foreign bodies must be performed to rule out other pelvic organs damage or bladder perforation [3]. In our case, radiographs and ultrasound scan provided sufficient evaluation of mature and extent of morbidity. Two cases are presented herein.
First being a 15-year-old male who inserted a flex electrical wire into his own urethra and subsequently into the bladder for self-erotic stimulation. The second case is a 16-year-old male with an over 6-month history of recurrent urinary infection post insertion into the bladder the coated electrical wire.
Case Presentation
Case 1
A 15-year -old male presented to us with obstructive urinary tract symptoms and a fragment of electrical wire protruding from the urethra.
He gave a history of having inserted an over-20 cm long coated metal wire into his urethra on the day of admission. Local perineum and genitalia examination revealed a visible part of the foreign body protruding per urethral meatus (Figure 1).
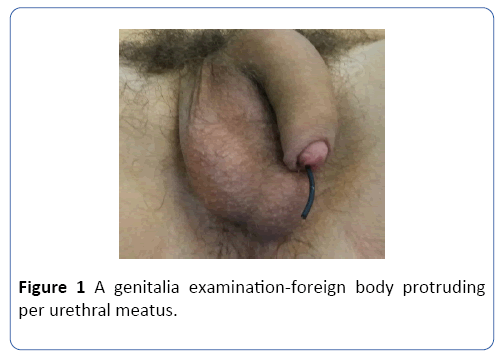
Figure 1: A genitalia examination-foreign body protruding per urethral meatus.
Per abdominal examination was essentially normal without bladder distension or discharge form urethra. After initial evaluations, the abdominopelvic radiograph anterior-posterior view which revealed coiled radio-opaque shadow extending along the urethra to the urinary bladder (Figure 2).
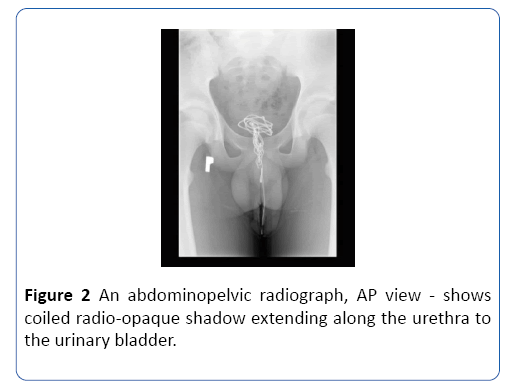
Figure 2: An abdominopelvic radiograph, AP view - shows coiled radio-opaque shadow extending along the urethra to the urinary bladder.
This confirmed the presence of a foreign body in the suprapubic area. An ultrasound scan showed normal upper urinary tract with a foreign body found in the bladder. An urethrocystoscopic removal failed due to knotting of electric wire. A suprapubic Pfannenstiel approach was then developed and cystotomy was performed during which the foreign body was completely removed (Figure 3). The patient was catheterized with a 22-Foley catheter. In the postoperative care, the patient was given trimethoprim course and on the 8th day, the bladder catheter was removed. The postoperative wound healed correctly without the signs of inflammation. He was followed-up 1 month after initial operation presented with no complaints or symptoms. A repeated abdominal ultrasound scan revealed no pelvic or bladder abnormality.
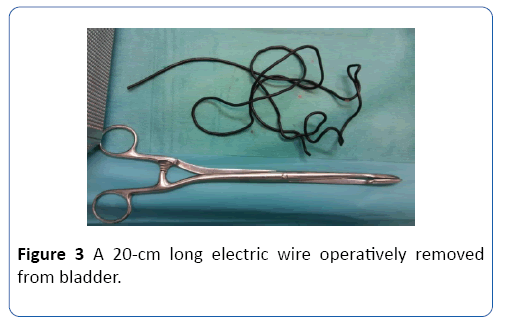
Figure 3: A 20-cm long electric wire operatively removed from bladder.
Case 2
A 16-year -old male presented to us with complaints of difficulty of voiding, dysuria, and a recurrent urinary tract infection. He gave a history of having inserted an electrical wire from the mobile phone charger into the urethra 6 months before the admission. After initial evaluations, an abdominopelvic X-ray revealed a long radio-opaque shadow in the suprapubic area corresponding with wire knotted within the bladder. An ultrasound scan showed a normal upper urinary tract with a calcified foreign body in the bladder (Figure 4).
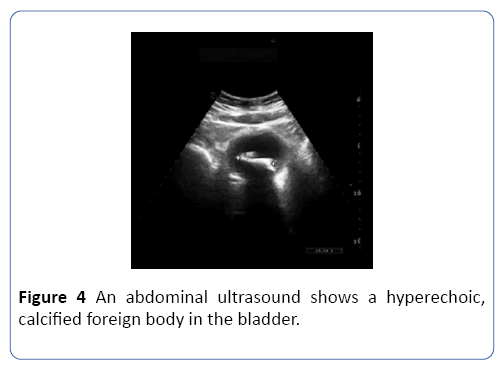
Figure 4: An abdominal ultrasound shows a hyperechoic, calcified foreign body in the bladder.
Local perineum and genitalia examination revealed no visible foreign body. On examination urinary bladder was not distended slight tenderness in the suprapubic region was noted but the rest of the abdominal and systemic examination was unremarkable. Initial he underwent an Urethrocystocopy during which the presence of calcified foreign body was verified but the attempt of removal via urethra was unsuccessful. Patient and his parents did not consent for open cystotomy so the procedure was discontinued and he was discharged.
14 days after first admission he was presented to our Ward with a gross lower abdominal pain and dysuria. Urine analysis showed macroscopic hematuria and bacteriuria with pus cells. His biochemical profile was otherwise unremarkable. At this time the consent for operative treatment was obtained. A suprapubic Pfannenstiel approach was then developed and cystotomy was performed during which the foreign body was completely removed (Figure 5). The patient was catheterized with a 22-Foley catheter. In the postoperative care, the patient was given an Amoxicillin course and on the 4th day, the bladder catheter was removed. The patient was discharged on the 5th day of hospitalization. The postoperative wound healed correctly without the signs of inflammation. He was followed-up 3 weeks after initial operation presented with no complaints or symptoms. A repeated abdominal ultrasound scan revealed no pelvic or bladder abnormality.

Figure 5: A calcified foreign body removed from the bladder.
Discussion
Urethrovesical foreign bodies are not a rare condition and can be a challenging problem in pediatric surgery and pediatric urology and it is usually a urologic emergency. The pediatric patient usually adolescents may complain of lower urinary tract symptoms and recurrent urinary tract infection [1,3].
Most of the cases foreign bodies are introduced deliberately for sexual stimulation but they can be also iatrogenically introduced during therapeutic manoeuvers. Other reasons being psychiatric disorders, narcotic drug intoxication or curiosity especially in children [4,5].
The different types of an object were seen in literature: including ballpoint pens, pins, battery, drinking straws, electrical wire, telephone cables, rubber tubes, toothbrushes, vegetables, wax or powders [6-8].
Initial management of the patients with intravesical foreign bodies should consist of clinical history and imaging study namely ultrasound scan which visualizes the radiolucent foreign bodies and plain radiographic film which delineate radio-opaque objects [9]. In uncomplicated cases, these modalities are enough to plan proper treatment options and rule out complications. Although cystography and computed tomography can be used for diagnosis [10].
Patient with urethrovesical foreign bodies presents with acute or chronic cystitis or/and urethritis. Some patients present with obstructive urinary tract symptoms and urine retention. In long-lasting cases additionally, the calcium encrustation and complication as fistulas, abscesses, sepsis may develop. Diagnosis is frequently made by a detailed history and physical examination of genitalia and abdomen. Broad-spectrum antibiotics may be required for the control of urinary tract infection and prevention of sepsis in infected patients.
The main goal of the treatment is the removal of a foreign body with no or minimal trauma to the urethra or the bladder. The best treatment depends on a different factor. The most important are; patient ’ s age, the general condition, comorbidities, the foreign body ’ s shape, size location and presence of complications. Small object recently inserted may be expelled spontaneously. Larger than the urethral lumen should be operatively removed.
Endoscopic removal of foreign bodies has been successful in most case reports. Cystoscopy is both a diagnostic and treatment tool for addressing the insertion of foreign bodies in the urethra and bladder usually utilizing endoscopic forceps, stone-retrieving baskets or balloon-wire baskets Small foreign bodies can be removed directly from urethra but in some case, it is necessary to push it back into balder and removed piecemeal [11,12].
In Kachakarn and Pummanagura report, 78 cases of foreign bodies in both male and female were assessed. They removed cystoscopically 74 out of 78 foreign bodies [7].
In our case, we tried to remove the intravascular object with foreign-body forceps, but this was not possible due to dimension and calcium deposits covering the objects.
Urethrocystocopy can be challenging especially in children due to the small diameter of the urethra. We then performed cystotomy and removed the object.
Enstrud and Poulsen introduced intravesical laparoscopy to untie the knots and retrieve wire [13]. The same was performed in children by Reddy and Danile who reported carbon dioxide insufflation and intravesical laparoscopy to remove the vesicle foreign body [14].
Hamouda et al. reported endoscopic treatment of mesh erosion in four patients that were successful in two of them [15]. Wyatt et al. have also been successfully using Holmium: YAG laser to remove intravesical foreign bodies to cut a wirelike object in the bladder [16].
If minimally invasive procedures fail to remove foreign bodies, suprapubic cystotomy by Pfannenstiel approach or other open surgery may be performed [17].
In our cases, foreign bodies were too big due to calcium deposits to be endoscopically removed so in both cases authors perform an open cystostomy during which foreign bodies successfully removed. This procured was safe and uneventful.
Conclusion
The intravesical foreign body is not seldom in the adolescent population. Their diagnosis can be made base on radiographs or ultrasound scan but the management can be challenging. Pediatric surgeons or urologist should consider the foreign body as a differential diagnosis when evaluating adolescents with acute or chronic lower urinary tract symptoms.
Urethrocystocopy is considered ideal for the removal of foreign objects.
Conflict of Interest
No competing financial interests exist.
Acknowledgments
Authors wish to thank the staff of the Department of Pediatric Surgery at S. Zeromski Hospital, especially Maria Wieczorek-Grohman, MD, PhD.
26383
References
- Ceran C, Uguralp S (2012) A Case Report. Self-Inficted urethrovesical foreign bodies in chidren. Case Reports in Urology. 2012: 3.
- Rahman NU, Elliott SP, McAninch J (2004) Self-inflicted male urethral foreign body insertion, endoscopic management and complications. BJU Int 94: 1051–1053.
- Rafique M (2008) Intravesical foreign bodies. Review and current management strategies. Urol J 5: 223–231.
- Jayadeep MR, Raviraj R, Shirol SS (2015) Electric wire as foreign body in the bladder and urethra-A case report and review of literature. Indian J Surg. 77( Suppl 3): 1323-1325.
- Pal DK, Bag AK (2005) Intravesical wire as foreign body in urinary bladder. Int Braz J Urol 31: 472-4.
- Vezhaventhan G, Jeyaraman R (2007) Unusual foreign body in urinary bladder: a case report. The Internet Journal of Urology 4: 2.
- KochakarnW, PummanaguraW (2008) Foreign bodies in the female urinary bladder: A 20-year experience in Ramathibodi hospital. Asian J Surg; 31: 130–133.
- Bakshi GK, Agarwal S, Shetty SV (2000) An unusual foreign body in the bladder. J Postgrad Med 46: 41-2.
- Younesi M, Ahmedani H, Asl Zare M (2004) An unusual foreign body in the bladder and percutaneous removal. Urol J 1: 126–127.
- Barzilai M, Cohen I, Stein A (2000) Sonographic detection of a foreign body in the urethra and urinary bladder. Urol Int 64: 178–180.
- Trehan RK, Haroon A, Memon S, Turner D (2007) Successful removal of a telephone cable, a foreign body through the urethra into the bladder: a case report. J Med Case Rep 1: 153.
- Kurz DA, Mucksavage P (2016) The endoscopic removal of eroded foreign bodies in the ureter. J Endourol Case Rep. 2: 30-32.
- Ejstrud P, Poulsen J (1997) Laparoscopic removal of an electric wire from the bladder. Br J Urol 80: 336.
- Reddy BS, Daniel RD (2004) A novel technique for removal of foreign bodies from urinary bladder using carbon dioxide insufflations. Surg Laparosc Endosc Percutan Tech 14: 238–239.
- Hamouda A, Kennedy J, Grant N, Nigam A, Karanjia N (2010) Mesh erosion into the urinary bladder following laparoscopic inguinal hernia repair: Is this the tip of the iceberg? Hernia 14: 317–319.
- Wyatt J, Hammontree LN (2006) Use of Holmium: YAG laser to facilitate removal of intravesical foreign bodies. J Endourol 20: 672–674.
- Park KS, Sim YJ, Jung H (2013) Migration of a Hem-o-Lok clip to the ureter following laparoscopic partial nephrectomy presenting with lower urinary tract symptoms. Int Neurourol J 17: 90–92.


