Jamali S MD1, Paydary K MD1, SeyedAlinaghi SA MD1*, Rasoulinejad M MD1
Iranian Research Center for HIV/AIDS (IRCHA), Tehran University of Medical Sciences, Tehran, Iran
*Corresponding Author:
SeyedAhmad SeyedAlinaghi, MD
Mailing address: Iranian Research Center for HIV/AIDS (IRCHA)
Tehran University of Medical Sciences, Tehran, Iran
Phone: +98(21)66947984
Fax: +98(21)66947984
Email: s_a_alinaghi@yahoo.com
Key words
Varicella pneumonia, immunosuppressed
Introduction
Although varicella pneumonia is rare, but it is the most seriously evoked complication of varicella infection in adults. The incidence rate of respiratory complications of varicella infection in adults are almost 25-fold more prevalent than in children. Although varicella in adults accounts for only 2% of all chickenpox cases, it may eventually lead to death [1-3]. To date, only a few case series and other retrospective analysis have been conducted to describe the very complicating features of this condition. We present a case of varicella pneumonia in an immunocompromised woman presented with dry cough, hemoptysis and positive radiological findings.
Case Presentation
A 29-year-old, non-pregnant, non-smoker female who is a known case of Crohn’s disease was referred to the Department of Imam Khomeini hospital in February 2010. She complained of progressive dyspnea, severe cough and fever in the last two weeks. She had no history of a prior chickenpox; however, she mentioned a history of contact with a patient with active varicella zoster infection. Within the last 6 months, she received combination therapy for Crohn’s disease composed of azathioprin (100 mg daily), mesalamine (Asacol; 2400 mg daily) and prednisolone (10 mg daily). Subsequently and concurrent with fever, the diffuse upper body rashes began to appear accompanying nausea, dyspnea, cough and hemoptysis in the last two weeks before attendance. She had also noted epigastric tenderness with intermittent diarrhea in the last week. At the same time, she suffered from severe fatigue, weakness and pruritis. On examination, she looked unwell with diffuse purpuric maculopapular and somewhat crusted rashes over her face, neck and torso. She was agitated and feverish. Abdomen was quite tender in the epigastric region. Organomegally was not detected on examination. Lower limb forces were decreased and reported as 3/5 on examination, while upper limb forces were normal (5/5) in both sides.
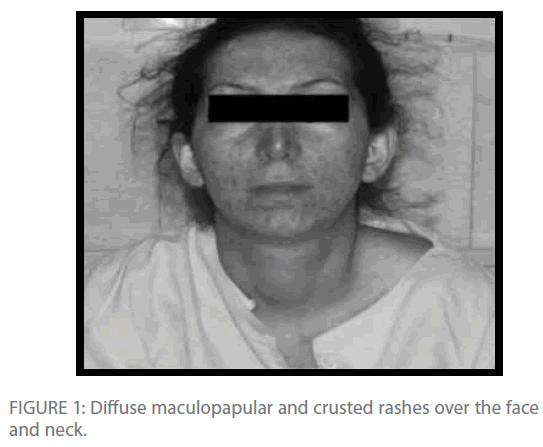
Figure 1: Diffuse maculopapular and crusted rashes over the face and neck.
The chest radiograph revealed predominant noduloreticular pattern of the posterior and inferior zones. The diagnosis of Varicella zoster infection has been established via skin biopsy from the abdominal wall. Since the patient suffered of anemia and thrombocytopenia, bone marrow aspiration and biopsy has been performed and reported as normal. Viral markers including HIV (Enzyme immunoassay), HBS Ag and Anti HCV were not reactive. Her lab data is shown in the following table.
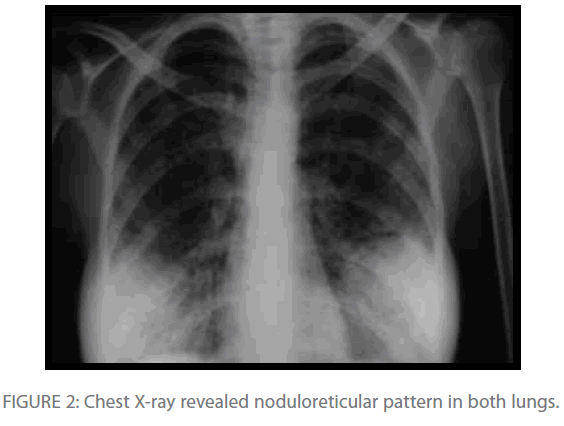
Figure 2: Chest X-ray revealed noduloreticular pattern in both lungs.
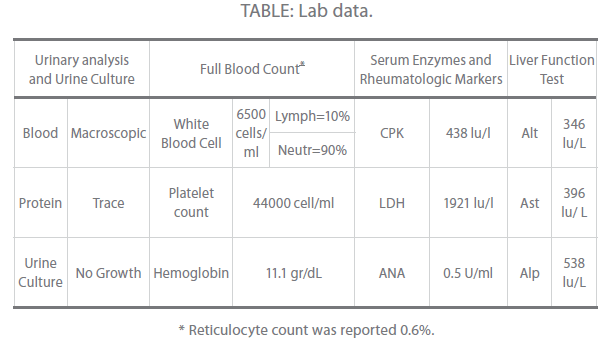
Table Lab data.
Soon after the diagnosis of chickenpox has been confirmed, intravenous acyclovir 10mg/kg was started 8 hourly and she started to improve over the next few days. Intravenous acyclovir has been administered for one week. Her chest radiographic findings and hematological markers returned to normal within a week, the fever resolved and skin lesions began to fully crust and disappear. The patient was discharged on day 14 and subsequently remained symptom free.
Discussion
Varicella pneumonia has been estimated to occur as one in 400 cases of chickenpox infection [4]. There is no sex predilection and immunosuppressive conditions may predispose patients to get varicella pneumonia. In fact, the course of varicella seems to be more aggressive in immunosuppressed hosts such as HIV infected and patients with organ transplant, than normal persons [5-7].
Our patient had taken high doses of anti-inflammatory drugs for the last 6 months, and this may account for high severity of both her skin rashes and respiratory condition. Respiratory complications seem to occur through the bloodstream rather than the local extension; therefore, suppression of cell-mediated immunity could have provoked development of varicella pneumonia in susceptible individuals [5,8]. Radiologic findings often include patchy or diffuse consolidation and nodular shadowing, while pleural effusion and hilar lymphadenopathy are of less prevalence [9]. Bronchial vesicular lesions have also been reported in bronchofiberscopy of patients with varicella pneumonia. It has been shown that chickenpox may be associated with a restrictive pattern of lung disease in acute and recovery phases. In addition to pneumonia, arthritis, encephalitis and secondary bacterial infections of the skin include other varicella complications [10-12].
In the present patient, liver dysfunction, anemia, thrombocytopenia and glomerulopathy were documented. It is not obvious whether chronic inflammatory diseases such as Crohn’s disease could have facilitated the development of above mentioned conditions. For example, one possible explanation for observed glomerulopathy is that prolonged inflammatory condition due to inflammatory bowel disease might have resulted in the formation of immune complexes and their subsequent precipitation in glomerular membranes. Moreover, reduced force of the lower limbs could have been related to the transient electrolyte dysregulation such as hypokalemia; however, this explanation has never been documented. These conditions might have evolved as a result of respiratory dysfunction and acute inflammatory state.
Although no randomized control trials have been conducted to provide evidence for the use of acyclovir in varicella pneumonia, it has become standard therapy for patients with or at risk of developing complications. The necessity of its use via IV route is also appreciable in complications such as pneumonia, particularly in immunocompromised patients. Moreover, to prevent potentially refractory respiratory failure in such patients, maximum ventilatory support is recommended. To avoid development of such severe complications in immunosuppressed patients, varicella zoster immunoglobulin is offered for those with a history of contact with a varicella infection resource [1,5,8].
To avoid development of varicella zoster infection complications such as life-threatening pneumonia especially in adults, a high degree of suspicion is needed. Clinical presentations of these patients in combination with accurate paraclinical assessments, particularly simple radiographies, may aid the clinicians to timely diagnose varicella pneumonia and limit the involvement via initiation of appropriate antiviral regimens, in this case acyclovir.
277
References
- Lee S, Ito N, Inagaki T (2004) Fulminant varicella infection complicated with acute respiratory distress syndrome and disseminated intravascular coagulation in an immunocompetent young adult. Int Med 43:1205-1209.
- Gucuyener K, Citak EC, Elli M (2002) Complications of varicella zoster. Indian J of Pediat 69(2):195-196.
- Kaneko T, Ishigatsubo Y (2004) Varicella pneumonia in adults. Int Med 43(12):1105-1106.
- Mandell GL, Douglas GR, Bennett JE (2000) Principal and Practice of Infectious Diseases. 5th Ed. Philadelphia, Churchill Livingston. 1582 p.
- Mohsen AH, McKendrick M (2003) Varicella pneumonia in adults. EurRespir J 21:886- 891.
- Popara M, Pendle S, Sacks L, Smego RA, Mer M (2002) Varicella pneumonia in patients with HIV/AIDS. Int J Infect Dis 6:6–8.
- Fehr T, Bossart W, Wahl C, Binswanger U (2002) Disseminated varicella infection in adult renal allograft recipients: four cases and review of the literature. Transplantation 73:608–611.
- Ho BCH, Tai DYH (2002) Severe adult chickenpox infection requiring intensive care. Ann Acad Med Singapore. 33:84-8.
- Nee PA, EdrichPJ. Chickenpox pneumonia: case report and literature review (1999) J AccidEmerg Med 147-150.
- El-Daher N, Magnussen R, Betts RF (1998). Varicella pneumonitis: clinical presentation and experience with acyclovir treatment in immunocompetent adults. Int J infect dis 2:147-151.
- Frangides CY, Pneumatikos I (2004). Varicella-zoster virus pneumonia in adults: report of 14 cases and review of the literature.Eur J Internal Med 15:364-370. Jaeggi A, Zurbruegg RP, Aebi C (1998) Complications of varicella in a defined central european population. Arch dis child 79: 472-477.

