Keywords
Mandibular tumour, Bone hyperplasia, Osteoma spongiosum
Introduction
Findings from paleoanthropological and paleopathological studies on bone materials are often a valuable source of information on the health status, biological development, health promoting behaviour, palliative measures and quality of life both of whole historical human populations and individual analysed subjects [1-3].
The preservation status of the bone material and the site of its deposition are important factors in the reconstruction of the course of disease, including its aetiology and epidemiology. Identification of health status based on the analysis of bone materials involves the correct diagnosis of disease and assessment of potential complications enabled by current clinical knowledge [3,4]. For a number of diseases only chronic conditions leave clear traces in skeletal materials. These conditions may be associated with the primary disease location in the bone tissue or be a secondary effect of other systemic diseases, e.g. of the respiratory, circulatory, or hematopoietic systems, being frequently of a neoplastic character [3,5].
Among many types of neoplastic lesions detectable in skeletal materials, bone tumours, both malignant and benign, are pathologies frequently identified within the skeleton, due to the preservation of bone tissue under conditions of fossilization [6-8].
Malignant bone tumours include: chondrosarcoma, osteosarcoma, fibrosarcoma, and their metastases. Major types of benign bone tumours include haemangioma, odontoma, chondroma and osteoma [5]. In previous studies on the health of historic populations from Wroc?aw bone materials were excavated from several medieval cemeteries located in close proximity to the city centre, and modern cemeteries. Researchers have identified benign neoplasms characteristic of osteoma and chondroma, located in the long bones of the extremities, in frontal and parietal bones, in a vertebral body, and a single case of a malignant tumour located in the vault of the skull [9-11]. However, none of the previously reported cases of neoplastic changes in bone material from the cemeteries of Wroc?aw concerned bone structures of the masticator organ. The presented mandibular tumour in a skull from a newly identified Early Modern cemetery in Wroc?aw, in Czysty Square (Plac Czysty), is the first case of this type.
The aim of our study was to carry out a paleopathological assessment, and to diagnose a case of a non-malignant bone tissue malformation in an adult female, located in the midline of the mandibular body, being a part of skeletal material excavated from the Early Modern cemetery, and to assess the impact of the diagnosed condition on the quality of life of the studied individual.
Material and Methods
In our study we analysed the skull from an adult female, excavated from grave no. 942, identified in the Early Modern Protestant cemetery near the now-gone Church of the Holy Saviour, dated at end of the 16th to early 18th century based on the town’s archived chronicles and copies of parish records, and situated outside the town walls of medieval Wroc?aw. More recently, this area was located within the limits of a construction site in Czysty Square in Wroc?aw, which was formerly the ?widnickie suburb.
In connection with a construction project carried out in 2006- 2007, 1426 sepulchral objects were identified and excavated. The objects were characterized by varying degrees of preservation of bone material, and included very well-preserved complete skeletons, very fragmented skeletons, as well as damaged and decaying bones [12]. In grave no. 942 an almost complete skeleton was found (Figure 1).
Figure 1: Skull from grave number 942 (Czysty Square in Wroc?aw) – state of preservation.
The state of skull preservation was defined as complete, i.e. cranium (Figure 1), with post- and ante-mortem loss of dentition, attrition of tooth crowns attributable to the intake of processed foods, and calculus around the preserved teeth. On preliminary macroscopic paleopathological inspection we found carious lesions in the crowns of 6 teeth, atrophic changes in the dental process, and hyperplasia in the mandibular corpus indicative of tumour (Figure 2). The research material is currently in the osteological collection of the Department of Anthropology, Polish Academy of Sciences in Wroclaw, Poland
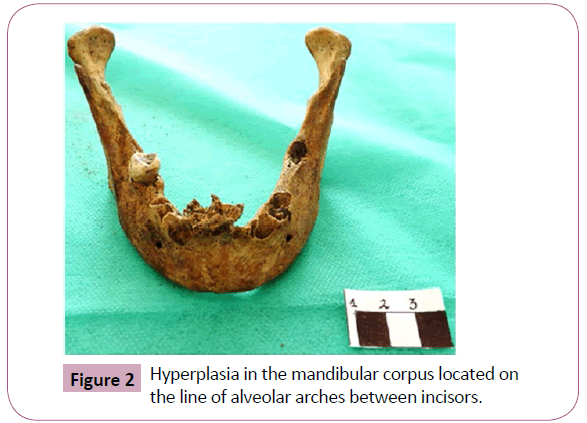
Figure 2: Hyperplasia in the mandibular corpus located on the line of alveolar arches between incisors.
The sex and age at death of the individual were estimated based on the skeletal and dental morphological features during macroscopic analysis. We analysed the expression of features in the supraorbital area, and the shape of the orbital openings, glabella and temporal, zygomatic and mastoid areas on both sides. We assessed the squama of the occipital bone for the presence of an external protuberance. In the mandible, we assessed the expression of the mental protuberance, the size of the gonial angle, and the course of the posterior margin of the mandibular ramus. In addition, we analysed the size of muscle insertions within the stomatognathic system [13-15].
The analysis of dimorphic features within the left and right pelvic bone was focused on the shape of the auricular surface, the size and shape of the greater sciatic notch, the shape of the inferior ramus of the pubic bone, and the size of the piriform muscle’s tuberosity [15-17].
The biological age was assessed based on the wear of tooth crowns, obliteration of cranial sutures, and involutive changes on the surface of the pubic symphysis [16-19]. Within the squama of the frontal bone we found only a partially obliterated frontal suture – sutura metopica.
Morphometric analysis of the skull was carried out using standard anthropometric equipment and measurement techniques established by Martin [20]. We took basic measurements (length and width) of the skull, including orbital openings and anterior nasal aperture, between standard anthropometric points according to the recommended methodology [16,20]. Because of the good condition of the long bones in the lower limbs, we additionally reconstructed the intravital body height using the methodology proposed by Piontek [15]. Within the alveolar arches we assessed carious lesions, resorption of lamina dura caused by periodontal diseases, and dental hygiene (based on the amount of calculus, according to methodology recommended in paleostomatology [21-23].
Bone tissue malformation detectable at the level of mandibular incisors, suspected to be a result of periosteal reaction, was examined using radiographic imaging techniques: a digital panoramic radiography system, Sirona Orthophos XG5DS, 60 kV/ 3mA, with exposure time 14.1 s, and spiral computed tomography on Sirona Galileos3 D; 85 kV/ 21 mAs, with exposure time 20s.
Next, the macroscopically identified tumour-like hyperplastic lesion was analysed for histopathological features. Specimens for the examination were embedded in Paraplast and sliced on a Slide 2003 microtome, to produce 20-30 μm sections, or prepared by grinding with diamond discs. Slices for examination were stained with haematoxylin and eosin (H+E) [24].
Results
Morphological features
In ancient time’s townspeople in Wroc?aw faced difficult living conditions, had low economic status, lived in considerably populated communities, had a poorly diversified diet, and had low health awareness. In some cases the only information about the incidence of disease, especially epidemics, can be found in chronicle records [10,25,26].
So far, studies of bone material from archaeological sites in Wroc?aw have led to the identification of developmental and degenerative changes, injuries, inflammatory diseases and metabolic disorders, but they have also revealed 15 cases of benign tumour. Analyzing the excavation material from a medieval Wroclaw it was observed a greater proportion of women who died reached the age of adultus (before 35 years of age), than women who died between 35 and 50 years of age (maturus). A large percentage of dying women at a young age is related to a worse nutrition and the risks associated with pregnancy and childbirth, especially with low levels of hygiene [9]. So far, studies of bone material from archaeological sites in Wroc?aw have led to the identification of developmental and degenerative changes, injuries, inflammatory diseases metabolic disorders and benign tumour [9,10]. A large number of pathological changes described above leads to the conclusion that among representatives of the townspeople part of them lived in bad conditions and at least some of them - mostly men - perform hard physical work. Food deficiency and poor hygiene further increased morbidity among adults and children [27].
The analysed morphological features of sexual dimorphism in the skull and pelvic bones from grave no. 942 explored from the newly-identified Early Modern cemetery from the area of Czysty Square in Wroc?aw were indicative of the female sex. Both the closure of the cranial sutures and the range of involutive morphological changes on the surface of the pubic symphysis corresponded with the forms characteristic of a biological age between 55 and 60 years (early senilis). However, the attrition of preserved tooth crowns indicated a younger age of the studied individual, which was about 45 to 50 years (maturus), and this may be associated with the intake of processed foods. Thus, the biological age at death could be established as not younger than late maturus.
In terms of basic anthropometric features the examined skull had greater facial length and width parameters, both in the neurocranial part (g-op length, eu-eu width, forehead width ft-ft) and in the facial part (zy-zy) when compared to the mean values from measurements taken in adult female individuals. Considering the n-pr distance (the upper facial height), we can conclude that the skull had a longer facial part than that suggested by the mean value of this parameter obtained for female skulls from Czysty Square.
The smallest differences in parameters between the skull from grave no. 942 and mean values were found for the height (n-pr) and width (eu-eu) of the neurocranium. We also found that the analysed skull had large surface areas of both orbital openings and apertura piriformis. Data collected for the relative features helped us to characterise the shape and proportions of the studied skull using 7 major quotient indices, denoting the use of absolute parameters (Table 1).
| Grave number |
942 |
Czysty Square – mean values measured for female skulls [mm] |
S.D. |
| Skull preservation |
CR |
| Sex |
female |
| Age |
≥ maturus |
| Parameter |
[mm] |
| skull length (M1*; g-op) |
178 |
169.8 |
5.6 |
| skull width (M8; eu-eu) |
148 |
145.2 |
5.8 |
| minimum forehead width (M9; ft-ft) |
102 |
95.7 |
4.4 |
| skull height (M17; ba-b) |
122 |
124 |
4.9 |
| maximum face width (M45; zy-zy) |
129 |
126.2 |
4.5 |
| upper facial height (M48; n-pr) |
72 |
65.4 |
3.7 |
| orbital width (M51; mf-ek) |
41 |
37.4 |
1.7 |
| orbital height (M52; sbk-spa) |
37 |
33.5 |
2.1 |
| aperturapiriformis width (M54; apt-apt) |
27 |
23.9 |
2.0 |
| nose length (M55; n-ns) |
46 |
47.7 |
3.1 |
* Numbering of measurements acc. to Martin and Saller [22]
Table 1: Measured values for the skull from grave no. 942 vs. mean values for female skulls from Czysty Square in Wroc?aw.
According to the classification adopted after Martin and Saller [20], and Malinowski and Bo?i?ow [28] (Table 2), the analysed skull from the female individual was found to be short in the neurocranial part (brachycranius) and low (tapeinocranius), with a medium-wide forehead (metriometopus) and a narrow face (lepten). According to the value of the Hrdli?ka-K??ka index the individual was tapeinocephalic. In the frontal part, the skull had a narrow face (lepten), medium-height eye sockets (mesoconch) and a medium-wide nose (mesorrhinus). The proportions revealed in the analysis corresponded with relative features from other female skulls from several medieval archaeological sites, e.g. Dominican Square (12-14th c.), the Churches of St. Jacob (13-15th c.), and St. Christopher (15-16th c.), and three Early Modern sites: the Church of St. Mary Magdalene (16-18th c.), the Church of SS. Peter and Paul (17th c.), and Czysty Square (16-18th c.), establishing the pattern of a short and low skull of an adult female, narrow in the facial part, with high eye sockets and a wide nasal part, which began to be more common in the late medieval period, including Wroc?aw, alongside a brachycepahlization trend spreading across Central Europe [9,29-32].
| No. |
Index name/ Index |
Skull no. 942 |
Classification |
| 1 |
Width-to-length index - eu-eu/g-op*100 |
83.1 |
Brachycranius |
| 2 |
Height-to-width index - ba-b/eu-eu *100 |
82.4 |
Tapeinocranius |
| 3 |
Frontal-parietal index - ft-ft/eu-eu*100 |
68.9 |
Metriometopus |
| 4 |
Hrdli?ka-K??ka index - ba-b/[(g-op+eu-eu)/2]*100 |
74.8 |
Tapeinocephalus |
| 5 |
Kollmann upper facial index/ n-pr/zy-zy*100 |
55.8 |
Lepten |
| 6 |
Orbital index/sbk-spa/mf-ek*100 |
90.2 |
Mesoconch |
| 7 |
Nasal index/ apt-apt/n-ns*100 |
52.9 |
Mesorrhinus |
Table 2: Values of major morphological indices for the skull from grave number 942.
The body height, established at 153.2 cm, was lower by over 3 cm than the mean body height (about 157 cm) of adult female individuals buried at the Early Modern cemetery in Czysty Square in Wroc?aw. Kozak [33] reported that changes in body height in women (in the range of 154 cm to over 156 cm), did not differ significantly between 1050 and 1650, either in rural or urban populations. This might suggest, considering the well-studied and confirmed ecosensitivity of body height, that there was a similar level of biological adaptation to continuous difficult living conditions persisting for several centuries.
The reconstructed body height, slightly different from mean values established for several skeletal series from Wroc?aw, might suggest the level of biological response, expressed in the final body height, reflecting difficult living conditions. This is, however, only one possible interpretation, as we have no detailed knowledge about the hereditary aspects of this feature.
Indicators of health and oral hygiene
In paleoanthropological research, the impact of environmental factors on the health and biological status of historical populations or their representatives is assessed based on the state of the masticatory system, which is usually one of the better preserved skeletal parts under postdeposition conditions [16,34]. In our study the wear of preserved teeth was advanced and showed signs of attrition found in adult individuals caused by the intake of processed foods by ancient populations [17,35]. In the skull from grave no. 942 we revealed carious lesions, atrophic changes in the alveolar process, and calculus. Our findings may, according to many authors, indicate poor oral hygiene, but also the intake of highly-processed foods, rich in carbohydrates, characteristic in the late medieval period and Early Modern times of various social groups from urban areas of an economic status higher than the average [11,36-39]. However, some studies, like the one carried out on a Scandinavian population, failed to demonstrate statistically significant differences in the incidence of caries in relation to social and economic status [40].
In the preserved teeth from the skull found in grave no. 942 we identified 6 carious lesions classified as medium-size based on the extent of enamel destruction. Because the incidence of carious lesions normally increases with age, the considerably extensive caries in the studied individual is not surprising [35,41]. In adults, the peak incidence of caries occurs between 35 and 65 years of age [42]. In addition, during macroscopic dental inspection, we identified signs of an apical abscess in the left part of the mandible at the level of P1. Clinical and paleostomatological studies indicated this anomaly as likely to be associated with deep caries and pulp gangrene [43,44].
Poor oral hygiene can also be concluded based on mineral deposits on the surface of tooth crowns (calculus), and consequential atrophic changes at the cervical level within the lamina dura. Dental plaque, as a starting point for the development of calculus, plays the primary role in the aetiology of caries and periodontitis [45]. In the analysed dentition of the skull from grave no. 942 we identified a small amount of calculus, but it reached the subgingival zone and was classified as the 1st degree of formation according to the Brothwell scale [21]. Calculus was present on the vestibular surfaces of incisors and canines, as well as on the buccal surface of premolars and molars. Moreover, it occurred together with irregular horizontal atrophic changes in bone tissue within the alveolar arch, as a result of intensified periodontitis (Figure 3).
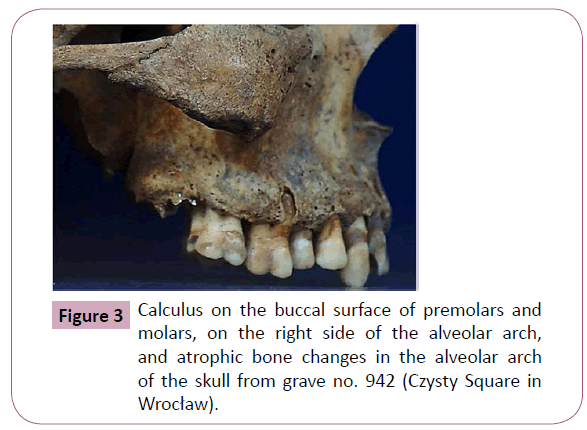
Figure 3: Calculus on the buccal surface of premolars and molars, on the right side of the alveolar arch, and atrophic bone changes in the alveolar arch of the skull from grave no. 942 (Czysty Square in Wroc?aw).
Poor oral hygiene among the people living in the Early Modern Wroc?aw is reflected by the high incidence of calculus, which was found in about 55% of adult individuals of both sexes [32]. In our study, the average loss of the alveolar process calculated as the sum of measurements taken for the atrophic lamina dura around the post mortem preserved teeth divided by the number of analysed tooth surfaces was close to 4.6 mm. This value suggests an advanced resorption of the alveolus lamina in the analysed individual in the course of periodontitis, producing symptoms such as bleeding from the gums, gingival recession, hypersensitivity of exposed parts of roots, and, even in the early stage, unstable positioning of teeth causing mastication difficulties [23,35,46,47]. In the mandible we identified alveoli obliterated following ante-mortem loss of three molars on the left side of the alveolar arch and one obliterated alveolus after the loss of the first molar. This loss of dentition might have resulted from caries or rapidly progressing periodontitis. Diseases of the alveolar process were common in the population from medieval and Early Modern Wroc?aw. In women buried near the Church of St. Elisabeth (15-16th c.) the incidence rate of periodontitis was established at over 71%, and studies on skulls from the Early Modern cemetery located near the Church of St. Mary Magdalene in Wroc?aw (16-18th c.) identified pathological atrophy of the alveolar process in over 60% of the analysed individuals [32,37]. Stomatognathic system diseases and lack of oral hygiene are among the characteristics commonly found in the Early Modern Protestant society in Wroclaw [27].
Tumour-like hyperplasia in the mandible
In the analysed material we also identified a tumour-like hyperplasia within the alveolar process and the midline of the mandibular corpus of the following dimensions: 20.5 mm - width between alveoli of the second incisors, 16.8 mm – anteroposterior midline depth, and 22.5 mm - height of bone tissue proliferation in the midline (Figure 4).
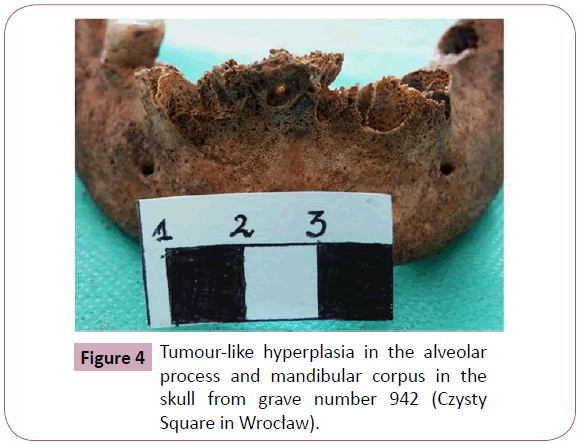
Figure 4: Tumour-like hyperplasia in the alveolar process and mandibular corpus in the skull from grave number 942 (Czysty Square in Wroc?aw).
Within the hyperplastic bone tissue of the alveolar process we found malformed and partly obliterated alveoli of incisors. This may indicate an ante-mortem loss of incisors. Further assessment of the neoplastic lesion was focused on the differential diagnosis between odontogenic tumours (odontoma), malignant tumours (osteosarcoma, myeloma), benign tumours producing bone tissue (osteoma, chondroma), neoplastic-like developmental changes or chronic osteitis. For this purpose we used radiographic imaging and histopathological techniques [48-51]. Preliminary analysis of the overall skull X-ray image did not show any pathologies in bone structures, except for the midline of the mandibular corpus. Because of the bone tissue malformation in the midline of the mandibular corpus, further analysis was based on a digital panoramic radiograph acquired with the Sirona Orthophos XG5DS system (60 kV/ 3mA) at an exposure time of 14.1 s. With this technique we identified signs of periosteal reaction and irregular growth of bone tissue which macroscopically resembled a spongy structure, a feature characteristic of benign bone tumours (Figure 5).
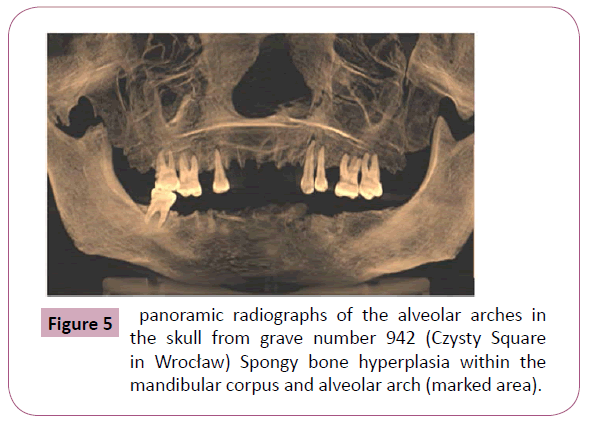
Figure 5: panoramic radiographs of the alveolar arches in the skull from grave number 942 (Czysty Square in Wroc?aw) Spongy bone hyperplasia within the mandibular corpus and alveolar arch (marked area).
Analysis of a digital image acquired using spiral computed tomography of higher voltage and longer exposure time (85 kV/ 21 mAs, 20 s) revealed the area of proliferated neoplastic tissue and changes in the structure of the compact substance of the bone and midline of the mandibular corpus. The recorded image shows an irregular hyperplasia of bone lamellae, formed on the inner side of the mandibular corpus, causing secondary changes in the normal structure of the compacted bone and partly in spongy bone. We concluded that this condition is most characteristic of a neoplastic lesion, defined as osteoma spongiosum and different from other types of osteoma, e.g. osteoma durum, formed almost entirely from compact bone, or from neoplasm-like developmental changes or chronic reactions suggesting periostitis [49,52] (Figure 6). In addition, the image of hyperplastic bone tissue resembling the substance of spongy bone, with a delicate sclerotic capsule and no clear foci of osteolytic lesions, rules out malignant tumours such as osteosarcoma, osteosarcoma iuxtacorticale or myeloma from the diagnosis [48,49,52].
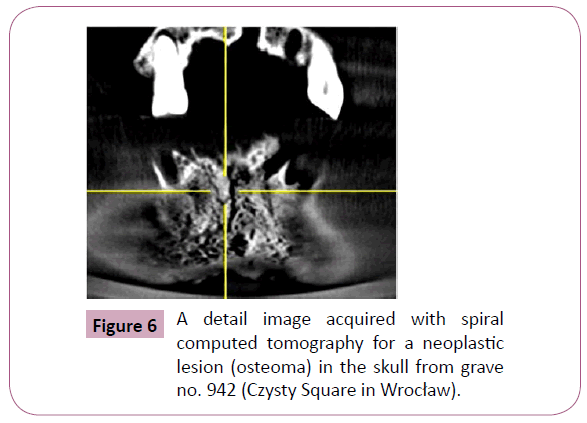
Figure 6: A detail image acquired with spiral computed tomography for a neoplastic lesion (osteoma) in the skull from grave no. 942 (Czysty Square in Wroc?aw).
Moreover, we found no compact bone hyperplasia from the periosteal side, which usually occurs during the formation of chondroma or osteochondroma [5,53]. Also, in the X-ray and CT images, we found no secondary odontogenic foci associated with the formation of hard dental tissues, usually amorphic aggregates of residual teeth, which rules out odontoma or odontoma compositum [54,55]. The radiographic assessment was followed by the histopathological examination of the specimen. In the field of vision (x100 zoom) we identified, apart from bone lamellae, additional numerous, randomly arranged osseous lacunae, which in vivo are filled with bone marrow or adipose tissue [56,57] (Figure 7).
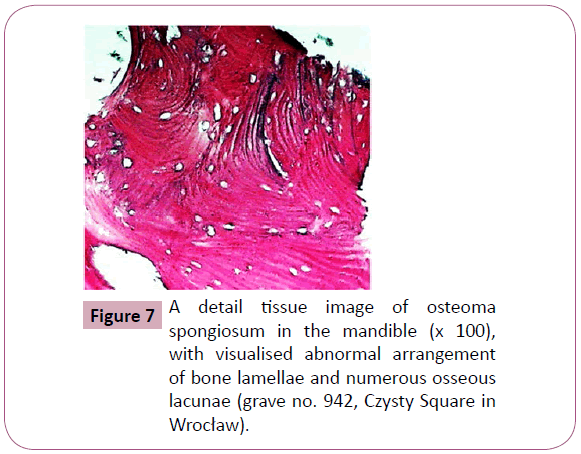
Figure 7: A detail tissue image of osteoma spongiosum in the mandible (x 100), with visualised abnormal arrangement of bone lamellae and numerous osseous lacunae (grave no. 942, Czysty Square in Wroc?aw).
The histopathological image confirms the macroscopic diagnosis previously made based on radiographic techniques, i.e. osteoma spongiosum formed in the midline of the mandibular corpus and alveolar arch. Growing osteoma spongiosum finally caused a massive deformation of the alveolar part of the mandible. The immediate consequence of such overgrowth of bone tissue was probably loosening incisors directly embedded in the tumour, resulting in their intravital loss and change of occlusion affecting periodontal health.
Osteomas classified as benign tumours, despite their abnormal bone tissue structure, are formed in a process similar to normal ossification [57,58]. Currently, osteomas are usually diagnosed accidentally based on radiographs, because they grow slowly, and are asymptomatic and painless up to a certain stage. Most osteomas are detected in long bones and girdle bones, or within cranial structures such as the skull cap, the frontal, maxillary and sphenoid sinuses, the ethmoidal labyrinth, the mastoid antrum, or bone structures of the alveolar arches, where they may cause recurrent pain or sinusitis [8,49,56,58-60]. In clinical diagnostics osteoma is also a pathology associated with Paget’s disease of bone – a genetically determined, focal metabolic disorder affecting the skeleton, and characterised by enhanced resorption of bone [61], and Gardner syndrome, also known as an autosomal dominant familial colorectal polyposis, where osteomas are formed, for example, in the paranasal sinuses [62,63].
Discussion
Many researchers point out that osteomas are more frequent in adults than in adolescents or children, and in men more than in women [49,58,64,65]. In our study, analysing the case from an Early Modern cemetery in Czysty Square in Wroc?aw, osteoma was identified in a female of maturus age. The general morphological characteristics of this individual, despite the slightly shorter stature than the mean value found for the female population, support our speculation that she was a typical representative of women living in Wroc?aw in the Early Modern period [9]. Short stature in this case, without knowledge of genetic background, does not allow for a full assessment of her health and identification of developmental conditions. In macroscopic analysis we found no pathologies other than those described within the masticatory sytem. These findings should be treated as preliminary, and require further thorough analysis with a focus, for example, on indicators of physiological stress, or disorders caused by overload or malnutrition [3,16]. Dystrophic disorders in alveolar lamellae, such as complications following periodontitis, or identified carious lesions in tooth crowns, are characteristic for the wider adult population from Wroc?aw. It should be stated, however, based on the results of clinical examinations, that complications following the formation and further growth of osteoma spongiosum may have decreased the quality of life, reduced general health, limited active life, and probably created aesthetic problems and also social difficulties with interpersonal relationships during adult life [66,67]. Hyperplasia in the anterior part of the mandibular alveolar arch undoubtedly caused difficulties in eating, but also limited the possibilities of verbal communication. The degree of tooth wear, particularly in the buccal zone, associated with the new parafunction, indicates the intake of refined foods, which might have contributed to the formation of calculus and difficulties in maintaining oral hygiene. As a result, the degree of tooth wear did not correspond with the biological age at death, established based on several skeletal criteria.
Today, osteoma spongiosum in such localization is treated by radical surgical resection of the tumour and a part of the stomatognathic system, because sparing resection may result in tumour recurrence [65,68,69]. In the case analysed by us, medical intervention, either therapeutic or palliative, was not an option available for this disease, and the described tumour was probably not a direct cause of death. The results of previous studies of bone pathology from archeological sites of medieval Wroc?aw have revealed 15 cases of benign tumor, including 14 osteomas and one chondroma [9-11], as well as one case of malignant tumor of the skull, classified as meningioma/hemangioma [9]. The most common are placed on the bones of the cranial vault, primarily the frontal bone, but can also occur in other skeletal bones [11]. Examples are 2 cases from St. Jacob's church in Wroclaw 2 cases of osteoma of long bones in 1 female and 1 male [9]. The identified mandibular osteoma spongiosum from cemetery from Czysty Square in Wroc?aw is thus the first case of this type reported for the historic area of south-western Poland. Information on neoplastic disorders of bone in archaeological skeletal materials, when properly diagnosed and described, may be an important and valuable contribution to epidemiological studies on neoplastic diseases among ancient and contemporary human populations.
The study was conducted within the framework of the research project No. 0069 / NPRH3 / H11 / 82/2014.
Acknowledgements
The authors would like to thank the head of the Department of Anthropology, Polish Academy of Sciences in Wroclaw prof. Slawomir Koziel, for the opportunity to carry out tests on the osteological material derived from Czysty Square in Wroc?aw.
7914
References
- Gladykowska-Rzeczycka J (1978) Frequency of some pathological changes discernible on bones occurence throughout millennia. PrzegladAntropologiczny 449: 187-193.
- Kozlowski T (1992) TrepanowaneczaszkizezbiorówZakladuAntropologii UMK w Toruniu. In: Biologiapopulacjiludzkichwspólczesnychipradziejowych, red. F. Roznowski, Slupsk 189-196.
- Ortner D, Putschar W (1997) Identification of Pathological Conditions in Human Skeletal Remains. Washington and London
- Jankowski J (1990) Epidemiologiahistorycznapolskiegosredniowiecza. Wroclaw.
- Waldron T (2009) Paleopathology. Cambridge Manuals in Archaeology, Cambridge University Press, Cambridge, New York, Melbourne, Madrid, Cape Town, Singapore, São Paulo.
- Kozlowski T, Drozd A (2006) Wczesnosredniowiecznecmentarzyskoszkieletowe w Kaldusie (stanowisko 1). Mons Sancti Laurentii 3. UMK Torun
- Brothwell D (2008) Tumours and tumour-like processes. In: Pinhasi R, Mays S (edn) Advances in Human Palaeopathology. John Wiley & Sons Ltd. Chichester 253-281.
- Premuzic Z, RajicSikanjic P, Masic B (2013) Frontal sinus osteoma in a 16th century skeleton from Zagreb, Croatia. International Journal of Paleopathology 3: 54-58.
- Kwiatkowska B (2005) MieszkancysredniowiecznegoWroclawia. Ocenawarunkówzyciaistanuzdrowia w ujeciuantropologicznym, Wroclaw.
- Markowska A (2007) Anthropological analysis of human skeletal remains from a Modern cemetery in Wyszynski street in Wroclaw, Poland. EAA Summer School eBook 1: 65-81.
- Kwiatkowska B, Szymczak N (2012) Analizaantropologicznakosciludzkich z badanprzykosciele sw. PiotraiPawlanaOstrowieTumskim we Wroclawiu, In: Nowozytnycmentarzprzykosciele sw. PiotraiPawlanaOstrowieTumskim we Wroclawiu (lata 1621-1670). Modern-time church of St Peter and St Paul cemetery in OstrówTumski, Wroclaw (1621-1670).Pankiewicz A. (red.), UniwersytetWroclawski, Wroclaw: pp. 69-94.
- Guszpit P, Mruczek R, Wojcieszak J, Wojcieszak M, Wojcik M (2010) PierwszywroclawskicmentarzprotestanckiprzykoscieleimieniaSalwatora-wstepnewynikibadan. In: SródmiejskaKatedra. Kosciól sw. MariiMagdaleny w dziejachikulturzeWroclawia.pod red. B. Czechowicza, Wroclaw 629-636.
- Acsadi G, Nemesceri J (1970) History of Human Life Span and Mortality. AkademiaKiado: Budapest.
- Loth SR, Henneberg M (1996) Mandibular ramus flexure: a new morphologic indicator of sexual dimorphism in the human skeleton. See comment in PubMed Commons below Am J PhysAnthropol 99: 473-485.
- Piontek J (1996) Biologiapopulacjipradziejowych. WydawnictwoNaukowe UAM, Poznan.
- Buikstra J, Ubelaker DH (1994) Standards for data collection from human skeletal remains. Arkansas Archeological Survey Research Series 44.
- White TD, Folkens PA (2005) The Human Bone Manual, Elsevier Academic Press, Oxford.
- Miles WA (1963) The Dentition in the Assessment of Individual Age in Skeletal Material. In: D.R. Brothwell (ed.), Dental Anthropology, Pergamon Press, New York, Paris 191-209.
- Lovejoy CO (1985) Dental wear in the Libben population: its functional pattern and role in the determination of adult skeletal age at death. See comment in PubMed Commons below Am J PhysAnthropol 68: 47-56.
- Martin R, Saller K (1957) Lehrbuch der Anthropologie. Gustav Fischer Verlag. Stuttgart.
- Tal H (1985) Periodontal bone loss in dry mandibles of South African blacks: a biometric study. See comment in PubMed Commons below J Dent Res 64: 925-929.
- Clarke NG, Hirsch RS (1991) Physiological, pulpal, and periodontal factors influencing alveolar bone. In: Advances in Dental Anthropology, M.A. Kelley, C.S. Larsen (edn), Wiley.
- Dlugoborski W, Gierowski J, Maleczynski K (1958) DziejeWroclawia do roku 1807. PWN, Warszawa.
- Busko C, Golinski M, Kaczmarek M, Ziatkowski I (2001) HistoriaWroclawia, t.1, Odpradziejów do koncaczasówhabsburskich. WydawnictwoDolnoslaskie. Wroclaw.
- Wachowski K (2015) Cemetery of our Saviour. The first protestant burial site in Wroclaw, Wratislavia Antiqua 21: 143-162
- Malinowski A, Bozilow W (1997) Podstawyantropometrii. Metody, techniki, normy, WydawnictwoNaukowe PWN, Warszawa-Lódz.
- Henneberg M (1976) The influence of natural selection on brachycephalisation in Poland. Studies in Physical Anthropology 2: 3-19.
- Piontek J (1979) Procesymikroewolucyjne w europejskichpopulacjachludzkich. SeriaAntropologia, 6, Wydawnictwo UAM, Poznan.
- Slociak J (1994) Zmiennosckierunkowawybranychcechkraniometrycznychodneolitu do póznegosredniowieczaiczasównowozytnych. ActaUniversitatisWratislaviensis nr 1594, StudiaAntropologiczne 1:47-74.
- Kwiatkowska B, Nowakowski D (2011) Charakterystykaantropologicznaszczatkówkostnych z cmentarzaprzykosciele sw. MariiMagdaleny we Wroclawiu (XVI-XVIII w.). Anthropological characteristics bone remains from cemetery near the church of st. Mary Magdalene in Wroclaw (XVI-XVIII c.), ZeszytyNaukoweUniwersytetuPrzyrodniczego we Wroclawiu, BiologiaiHodowlaZwierzat: 58(583):25-43.
- Kozak J (1998) Wplywstrukturyspolecznejnacechybiologicznesredniowiecznychpopulacji z terenuPolski. In: Spolecznekontrasty w staniezdrowiaPolaków, PierwszeWarsztatyAntropologiczne, Warszawa 105-118.
- Hemphill BE (2008) Dental pathology prevalence and pervasiveness at TepeHissar: statistical utility for investigating inter-relationships between wealth, gender and status. In: Technique and Application in Dental Anthropology, JD Irish, GC Nelson (edn), Cambridge University Press, Cambridge, New York, Melbourne, Madrid, Cape Town, Singapore, Sao Paulo 178-215.
- Larsen CS, Shavit R, Griffin MC (1991) Dental Caries Evidence for Dietary Change: An Archeological Context. In: Advances in Dental Anthropology, MA Kelley, CS Larsen (edn), Wiley-Liss, New York, Chichester, Brisbane, Toronto, Singapore 179-202.
- Dabrowski P, Gronkiewicz S (1997) Prochnicazebow u sredniowiecznychmieszkancówWroclawia (XV-XVI w.). ActaUniwersitatisWratislaviensis, No 1916, StudiaAntropologiczne 4:17-30.
- Lingstrom P, Borrman H (1999) Distribution of Dental Caries in an Early 17th Century Swedish Population with Special Reference to Diet. International Journal of Osteoarchaeology 9: 395-403.
- Lopez B, Pardiñas AF, Garcia-Vazquez E, Dopico E (2012) Socio-cultural factors in dental diseases in the Medieval and early Modern Age of northern Spain. See comment in PubMed Commons below Homo 63: 21-42.
- Larsen CS (1997) Bioarcheology. Interpreting Behavior from the Human Skeleton, Cambridge University Press, Cambridge.
- Einwag J, Naujokos R (1994) Epidemiologiapróchnicy In: Stomatologiazachowawcza, I, S. Potoczek (red.), Urban & Partner, Wroclaw 25-48.
- Djuria M, Rakocevia Z (2007) Pathology of the mandibles and maxillae from archaeological context: discrepancy between diagnoses obtained by external inspection and radiological analysis. CollAntropol 31: 379-385.
- Lucas S, Sevin A, Passarius O, Esclassan R, Crubezy E, et al. (2010) Study of dental caries and periapical lesions in a mediaeval population of the southwest France: Differences in visual and radiographic inspections. HOMO - Journal of Comparative Human Biology 61: 359-372.
- Hillson S (2008) Dental pathology. In: Biological Anthropology of the Human Skeleton. John Wiley & Sons, Inc., Hobben, New Jersey 301-341.
- HildeboltChF, Molnar S (1991) Measurement and description of periodontal disease in anthropological studies. In: Advances in Dental Anthropology, MA Kelley, CS Larsen (eds.), Wiley-Liss, Inc., New York, Chichester, Brisbane, Toronto, Singapore 225-240.
- StrohmTh F, Alt KW (1998) Periodontal disease -etiology, classification and diagnosis. In: Dental Anthropology. Fundamentals, Limits, and Prospectes, K. w. Alt, F. W. Rösing, M Teschler-Nicola (eds.), Springer Wien New York, 227-246.
- Dominiok GW, Knoch H (1985) Nowotworyiguzopodobnechorobykosci. Warszawa
- Greenspan A (1993) Benign bone-forming lesions: osteoma, osteoid osteoma, and osteoblastoma. Clinical, imaging, pathologic, and differential considerations. Skeletal Radiol 22: 485-500.
- An YH, Martin KL (2003) Handbook of Histology Methods for Bone and Cartilage. Humana Press.
- Greenfield GB (1990) Radiology of bone diseases. J.B. Lippincott Company, Philadelphia
- Aufderheide AC, Rodríguez-Martín C (2006) The Cambridge Encyclopedia of Human Paleopathology. Cambridge University Press
- Kaneko M, Fukuda M, Sano T, Ohnishi T, Hosokawa Y (1998) Microradiographic and microscopic investigation of a rare case of complex odontoma. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 86: 131-134.
- Preetha A, Balikai BS, Sujatha D, Pai A, Ganapathy KS (2010) Complex odontoma. Gen Dent 58: e100-102.
- Capasso L (1997) Osteoma: Paleopathology and phylogeny. International Journal of Osteoarchaeology 7: 615-620.
- Janas A, Grzesiak-Janas G (2005) EndostealOsteomas in Authors’ Own Material. Dental and Medical Problems: 42: 431-435.
- Erdogan N, Demir U, Songu M, Ozenler NK, Uluç E, et al. (2009) A prospective study of paranasal sinus osteomas in 1,889 cases: changing patterns of localization. Laryngoscope 119: 2355-2359.
- Summers LE1, Mascott CR, Tompkins JR, Richardson DE (2001) Frontal sinus osteoma associated with cerebral abscess formation: a case report. SurgNeurol 55: 235-239.
- McHugh JB, Mukherji SK, Lucas DR (2009) Sino-orbital osteoma: a clinicopathologic study of 45 surgically treated cases with emphasis on tumors with osteoblastoma-like features. Archives of Pathology & Laboratory Medicine: 133: 1587-1593.
- Whyte MP (2006) Clinical practice. Paget's disease of bone. N Engl J Med 355: 593-600.
- Lew D, DeWitt A, Hicks RJ, Cavalcanti MG (1999) Osteomas of the condyle associated with Gardner's syndrome causing limited mandibular movement. J Oral MaxillofacSurg 57: 1004-1009.
- Moretti A, Croce A, Leone O, D'Agostino L (2004) Osteoma of maxillary sinus: case report. ActaOtorhinolaryngolItal 24: 219-222.
- Noterman J, Massager N, Vloeberghs M, Brotchi J (1998) Monstrous skull osteomas in a probable Gardner's syndrome: case report. SurgNeurol 49: 302-304.
- Sayan NB, Uçok C, Karasu HA, Günhan O (2002) Peripheral osteoma of the oral and maxillofacial region: a study of 35 new cases. J Oral MaxillofacSurg 60: 1299-1301.
- Kaplan I, Calderon S, Buchner A (1994) Peripheral osteoma of the mandible: a study of 10 new cases and analysis of the literature. J Oral MaxillofacSurg 52: 467-470.
- Kondoh T, Seto K, Kobayashi K (1998) Osteoma of the mandibular condyle: report of a case with a review of the literature. J Oral MaxillofacSurg 56: 972-979.
- Yildiz Y, Bayrakci K, Altay M, Saglik Y (2001) Osteoid osteoma: the results of surgical treatment. IntOrthop 25: 119-122.
- Chiu AG, Schipor I, Cohen NA, Kennedy DW, Palmer JN (2005) Surgical decisions in the management of frontal sinus osteomas. Am J Rhinol 19: 191-197.


