Keywords
Abortion, unsafe, experiences, self-induced, students, Ghana
Introduction
Comprehensively defined, abortion is the termination of a pregnancy after, accompanied by, resulting in, or closely followed by the death of the embryo or fetus: or a spontaneous or induced expulsion of a human fetus during the first 12 weeks of gestation [1]. However, the nebulous nature of ‘abortion’ has given rise to several definitions of the term across a wide range of health-related disciplines. Still, the central point made by majority of the definitions on abortion is the fact that the pregnancy is not wanted. Unwanted pregnancies and abortion have existed since time immemorial. The influential work of Devereux2 on the history of abortion around the world points to the frequency of abortion across cultures and time. Specifically, he points out that Chinese, Greek and Roman cultures all developed systems of dealing with unwanted pregnancies and regulating population growth in their respective societies. Also the Egyptians were the first to create abortion techniques, which were discussed and reported in some of their first, and the oldest medical texts [2].
Today, abortion is one of the most common gynaecological experiences; perhaps the majority of women will undergo an abortion in their lifetimes [3]. Safe abortions (those done by trained providers in hygienic settings) and early medical abortions (using medication to end a pregnancy) carry few health risks [4]. However, every year, close to 20 million women risk their lives and health by undergoing unsafe abortions [5]. At least 25% of these women face a complication with permanent consequences and close to 66,500 women die [6]. This is especially true for women in developing countries who are faced with resource challenges as well as negative social, religious and cultural pressure. In fact, Grimes, Benson, Singh, Romero, Ganatra, Okonofua, Shah [7] report that nearly all unsafe abortions (97%) are in developing countries with millions facing permanent complications.
Importantly, a significant proportion of unsafe abortions in Ghana and other developing countries involve students [8-11]. Pachankis [12] confirms that students in developing countries remain the major vulnerable group most likely to have abortions and suffer abortion stigma. Adanu, Tweneboah [13] also recount the imperfect knowledge on the effects and causes of abortions among students in Ghana and subsequently, the need for research.
Even though some studies have been conducted on abortions in Ghana, a cursory review reveals a dearth of empirical information on the experiences Higher Education students on abortion. Importantly, while Sinha, Khan, Patel, Lakhanpal, Khanna [14] suggest that decisions and consequences of abortion may be influenced by, and affect not only the pregnant woman, but also the man responsible for the pregnancy, majority of the studies in Ghana have focused on the views of only female students. This study therefore seeks to address the paucity of empirical information the abortion discourse among male and female students in general, as well as provide evidence from their experiences to shape contemporary interventions and policies on abortion by both state and non-state actors. Particular emphasis is placed on the nature of experiences of students, the number of abortions experienced, the gestation period of aborted pregnancy as well as where the abortion procedure was done.
Methods and procedure
Data for the study was collected through 18 focus group discussions (FGDs) involving 142 students randomly sampled from the main and city campuses of University of Ghana. The discussions were done on weekends to avoid clashes with the lecture times of participants and each session lasted between 85 and 110 minutes. Appropriate permissions were sought from the relevant university authorities. The study was also reviewed and approved by the research and conferences committee of the University of Ghana Business School prior to data collection.
The procedure for selecting participants involved announcing and posting notices on the nature, content and use of the study and asking interested students to contact the research team. After 4 weeks, 158 students had volunteered to partake in the study. Students who volunteered to participate were again briefed on the purpose, the nature of information required, the available times as well as the mode of the FGD. The students were then taken through and given copies of the information sheet and consent forms for the study. After a further 2 weeks, 142 students gave informed consent and 16 students declined further participation in the study. The students were given the available dates, times and venues of the discussions and asked to choose any slot at their convenience. In line with Mack, Hilden, Watterson, Moore, Turner, Grier, Weeks, Wolfe [15] and Fossey, Harvey, McDermott, Davidson [16] the focus groups were restricted to a maximum of 9 participants. Thus, students who chose groups that had reached the 9-member limit were made to choose other groups.
A modified version of the Knoxville Center for Reproductive Health’s [17] abortion questionnaire was used for the study. The questions asked during the discussions were anonymous and focused on gathering information on the nature of abortions experienced by students, the number of abortions experienced, the gestation period of aborted pregnancies as well as who/where the abortion procedure was performed. Data on participants’ background was also collected before the discussions began. The questionnaire was pretested with a trial group of 7 students and further modified before being validated for the study.
The FGDs were recorded and transcribed and later shown to participants for signing-off before being analysed. The transcribed data was grouped under the key themes of the study and qualitatively analysed and discussed using the thematic analyses approach. Summary tables were also developed to depict some of the key issues under discussion.
Results
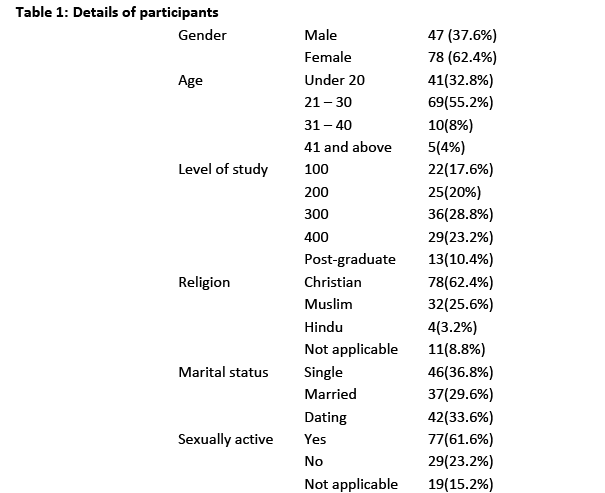
As shown in Table 1, majority (62.4%) of the participants were female with 32.8% being in their teens. A total of 86% were below 30 years, 8% were between 31 and 40 years with only 4% being above 40 years. Sufficient numbers of participants were drawn from all levels of study on both campuses with majority of respondents (62.4%) being Christians. 25.6% of the participants were Muslims, 3.2% were Hindus and 8.8% did not indicate their religion. 36.8% of participants were single, 29.6% were lawfully married and 33.6% were dating. Also, majority (61.6%) of respondents were sexually active at the time of the FGDs.
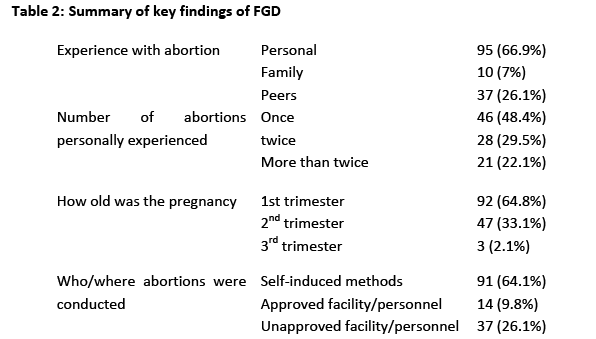
Results of the FGDs show that all students involved in the study had experienced abortions with 95 (66.9%) having personal experiences on abortions. Students in this group were females who had undergone an abortion procedure or males had consented to, influenced or supported a partner to have an abortion. Also, 37 (26.1%) had direct experience from peers - friends, course-mates, roommates. Students in this category were those who though had not personally had an abortion, closely knew or assisted a peer to undergo an abortion. The remaining 10 (7%) had experienced abortions in their family especially with their sisters.
Further discussions uncovered that only 46 (48.4%) out of the number who had been personally involved in abortions had done so once. Thus repeat abortions were common among students with more than half of the students having had multiple abortions. Specifically, 28 (29.5%) had undergone 2 abortions while 21 (22.1%) had undergone more than 2 abortions. In the words of one student
‘… the first pregnancy was a mistake so I aborted it without even telling my boyfriend. I had to abort the second pregnancy when I found out that the guy I was involved with was married. There was no point having a child with him if he was not going to marry me’
Findings also show that 92 (64.8%) of the abortions experienced were done in the first trimester of the pregnancy. 47 (33.1%) of students had also experienced abortions in the second trimester. Majority of the second trimester abortions were done in the early weeks of the second trimester and were attributed to the late detection of the pregnancy or a late decision not to keep the pregnancy. The 3 (2.1%) cases of third trimester abortions identified had been done by married students and were all done in hospitals based on medical grounds. Generally, a key consideration in the decision and timing of the abortions was the avoidance of detection of not only the pregnancy, but the importantly the abortion.
‘...getting pregnant is one thing but to be found to be engaged in abortions is even a more serious matter. Apart from the usual criminal charges, stigma, disgrace and embarrassment, your chances of even getting a husband when seen as an ‘abortion girl’ is drastically reduced’
Study findings also show that 91 (64.1%) of pregnancies experienced by students were self-induced. In such instances, they bought drugs or items meant to serve as abortifacients and performed the abortion mostly privately or with the assistance of friends in a few instances. Only a measly 14 (9.8%) of students had any experience of abortions conducted in an approved facility or by authorised personnel. This was in spite of their awareness and availability of safe abortion services. However, 37 (26.1%) of abortion experiences shared by students involved quack doctors, herbalists and ‘mallams’. Study findings suggest a new trend of door-to-door and mobile abortion services being provided by quack doctors.
‘… I called the number and we discussed everything from length of the pregnancy to the cost of abortion. He then gave me directions to a health facility on the ourskirts of Accra and told me to come alone at a designated time, with his money and without a phone. I got there, met him, confirmed my details routinely and he performed the abortion. He told me to lie down for a couple of hours for the pain to subside after which I left’
Discussion
As earlier studies [10,11,18] show, abortions are common among students in Ghana and other developing countries. Thus, it was not surprising that all students in this study had experiences on abortion. Further, the fact that a significant majority (93%) of respondents had personal or peer experiences on abortions provides justification for the classification of students as a high risk group by the GMHS [19]. While a limited level of partner and peer influence in abortions have been noted among students in Ma, Ono-Kihara, Cong, Xu, Pan, Zamani, Ravari, Kihara [9], this study suggests a relatively significant level of peer and partner support for abortions among students. Support provided varied from paying for the procedure, helping to procure or prepare the drugs and items used, helping with the administration of the drugs or concoctions, providing company and support during the process, to accommodating the pregnant girl during the procedure to avoid detection by her family or close friends.
Even more worrying is the fact that more than half of the students involved in abortions had done so more than once. Whiles confirming recent studies [20,21] that point to a trend of multiple abortions among students, evidence from the FGDs suggest that students who have had an abortion are likely to do so again when faced with subsequent unwanted pregnancies or similar situations that necessitated the first abortion. Importantly, students after the first abortion, gain confidence, begin to see abortions as a viable solution to unwanted pregnancies and as explained by Haider, Stoffel, Donenberg, Geller [22] are less likely to use contraceptives for further sexual encounters.
In line with Ahiadeke [23], there were limited experiences of early second-term abortions among students in this study. A number of students who had second term abortions were not certain about being pregnant or did not detect the pregnancy early. Evidence from Pell, Meñaca, Were, Afrah, Chatio, Manda-Taylor, Hamel, Hodgson, Tagbor, Kalilani [24] supports students account that this was common among girls with irregular menstrual cycles or who still had their menstruation despite being pregnant. Even in cases where the pregnancy was detected early, the cost of the abortion [23] resulted in the procedure being delayed till the second term. This experience were common among pregnant girls who together with their boyfriends were students and therefore unable to afford the procedure immediately. Some second term abortion also resulted from a late decision by girls who initially considered carrying the pregnancy to term. Students attributed late decisions to abort to pressure from partners or family18, as well as the subsequent reluctance to carry the pregnancy to term alone after breaking up with their partner in the course of the pregnancy.
Unsurprisingly, majority of the abortions were within the first trimester, mostly the first 8 weeks. Whiles consistent with Major, Cozzarelli, Cooper, Zubek, Richards, Wilhite, Gramzow [25] and Munk-Olsen, Laursen, Pedersen, Lidegaard, Mortensen [26], further probe suggests concealment of the pregnancy and the abortion from parents, peers and the community [8] as a key consideration in early abortions among students. Consequently, the abortions were done immediately pregnancy was suspected or confirmed; and before signs of pregnancy became evident. Interestingly, students were even more interested in concealing the abortion than they were in concealing the pregnancy. This may be explained by the fact that the laws in Ghana criminalized abortions but not pregnancy. Further that, the bad-will, stigma and negative socio-cultural attitudes and actions was far more severe on persons engaged in abortions than pregnancy in Ghana.
Almost two-thirds of abortions experienced by students in this study were self-induced. While confirming findings by similar studies18,20,27, this study also points to a widespread awareness and preference of self-induced abortions among students. Student’s preference for self-induced abortions was primarily based on the ease of accessing the materials used and the cheap associated cost. Quite apart from that, students believed that self-induced methods allowed them to do the abortions privately and in the comfort of their surroundings with little chance of detection by peers and family. This suggest that more effort must be placed by both state and non-state stakeholders on tackling the knowledge base, causes and effects of self-induced abortions among students if significant gains are to be made in reducing the incidence of unsafe abortions among students.
In Ghana, the laws on abortion [28,29] apart from defining the conditions under which abortions can be legally done also directs that abortions be done only by persons registered with and so authorised by the Ghana Health Service, Nurses and Midwife Council or the Medical and dental Council in a facility registered for that purpose by the Private Hospitals and maternity Homes Board (for private facilities) or the Ghana Health Service (for public facilities). Consequently, a good number of facilities, both private and public, as well as healthcare personnel including midwives and other community outreach workers have been trained and registered to perform abortions guided by the conditions set by the law and the Ministry of Health’s guidelines on abortion. Despite the availability of these safe abortion services, evidence from this and other studies [9,10] suggest a low level of utilization among students even though they were aware of safe abortion services. Thus, in contrast to studies [30,31] that ascribe the low levels of utilization of safe abortion services by persons under 25 to the unavailability of these services, this study suggests the existence of other barriers to utilization of safe abortion services other than availability of the service. Of relevance in this vein may be Sedgh’s [32] suggestion that the cost and perceived stigma associated with utilizing publicly provided safe abortions services may be a hindrance to the youth especially those without employment.
In relation to the above, it was disturbing to note that more than a quarter of abortions experienced by students were done by unauthorized person or facilities. While this figure is slightly higher than experienced in the sub-saharan region3,33 among persons of the same age group, it also underscores the prevalence of ‘quack’ abortion doctors and facilities even in countries like Ghana with liberal abortion laws and safe abortion services. Majority of these quack’ herbalists, ‘mallams’, doctors or nurses are unskilled, operate clandestinely in unsafe environments and often cause complications that may permanently harm the pregnant female.34-36 In spite of their awareness of the risks involved in utilizing quack abortion services, students still patronised their services owing to the clandestine nature, relatively cheap charge, and few questions asked. While the usual trend is for quack personnel to perform abortions in their homes, in their offices, in rooms rented out of town purposely for the purpose, or in privately owned health centers, student experiences shared in this study suggests that the activities of quack personnel have diversified to include mobile and door-to-door services. There were instances where quack personnel had come to the residence of students to perform the abortions. Mention was also made of a growing trend where you called them, made a deposit into their accounts and they walked you through the process on phone, including directions on what and where to find the needed abortifacients and how to use them. These activities of quack doctors raise serious public health questions that need immediate attention if the high incidence of abortion related complications and deaths are to be reduced in Ghana and other sub-saharan countries.
Limitations
Considering the personal and sensitive nature of abortion related experiences in Ghana, the study acknowledges that there may be some underreporting, misrepresentations and misinformation by students especially in a Focus Group Discussion setting.
Even though the study provides important descriptive insights into some of the key experiences of students on abortions, it may not be an entirely accurate measure for generalizing abortion experiences among all student groups in Ghana. This is recognition of the differences may exist in the determinants, experiences and decisions on abortion among basic school, High School, College and University students.
Implications
The study has broad implications for students, the youth generally and all state and non-state stakeholders involved in research, policy and practice of family and reproductive health in Ghana and other sub-saharan African countries.
While serving as a fair assessment of the knowledge and experiences of students among students, it also emphasizes the key role of peers and male partners in influencing abortion decisions and procedures. Consequently, policies and interventions aimed at educating, reducing abortion stigma and culling unsafe abortion practices among students must target peers and male partners as advocates and actors of knowledge dissemination and behaviour change among students. Generally, the study emphasises the urgent need for sensitization and education on self-induced abortions, contraception, counselling and family planning services among students.
Considering study findings that awareness and availability were not dominant barriers to utilization of safe abortion services among students, further attention and research is warranted to identify other causes of low utilization of such services and ways through which students could be encouraged to utilize safe abortion services.
Clearly, sanctions and legislations have had little impact on the activities of unsafe abortion providers. While poor implementation of sanctions may be a cause, a dearth of relevant information exists on the current practices and operations of unsafe abortion services. Urgent research is therefore necessary to identify the extent, role, methods used and operations of quack doctors and providers of unsafe abortion services. This will provide the needed information for evidence based policies and interventions to halt their activities.
Conclusion
Abortion remains a global public health issue and an important barrier to attaining the fifth Millennium Development Goal (MDG) of reducing maternal mortality ratio by three quarters and achieving a universal access to reproductive health by 2015. Nevertheless, policy and action on abortion among students and other vulnerable groups have been lethargic, less proactive and deficient in evidence base in Ghana.
While recognising that national and regional estimates on the availability of safe abortion services have increased in Ghana and other sub-saharan countries, utilization of these services still remain poor among students in favour of unsafe abortions. Quite apart from that, the continuous and unregulated operations of quack abortion service providers remain a threat to the attainment of the MDGs and other safe reproductive health targets of the government.
Evidence from this study when juxtaposed with others in similar contexts confirms that students are indeed a major risk group that need immediate attention in the abortion discourse in Ghana and other sub-saharan countries.
The risk is further exacerbated by the commonness of multiple abortions among students as well as their preference for and indulgence in self-induced abortions methods. This calls for a shift in direction of research and interventions aimed at reducing abortion stigma and unsafe abortions among students towards the student-specific factors identified above. Importantly, peers and male partners will be key to the success of these efforts. Also of essence in this direction will be multi-stakeholder approaches in sensitization and education on unsafe abortions; contraception; and counselling and family planning services among student.
Acknowledgments
Author acknowledges Christabel Nortey, Sonia Oklu and Yvette Boateng for assisting with the Focus Group Discussions and transcription.
2616
References
- Francome C. Abortion in the USA and the UK. Ashgate Publishing, Surrey, 2004.
- Devereux G. A typological study of abortion in 350 primitive, ancient, and pre-industrial societies. Abortion in America 1967; 97.
- Aahman, E., Shah I. Unsafe abortion: Global and regional estimates of unsafe abortion and associated mortality in 2000. 4th ed. WHO, Geneva, Switzerland 2004.
- WHO. Safe abortion: technical and policy guidance for health systems. WHO, Geneva, Switzerland 2004.
- Sedgh G, Henshaw S, Singh S, Åhman E, Shah IH. Induced abortion: estimated rates and trends worldwide. The Lancet 2007; 370(9595):1338-1345.
- Kumar A, Hessini L, Mitchell EM. Conceptualising abortion stigma. Culture, Health & Sexuality 2009;11(6):625-639.
- Grimes DA, Benson J, Singh S, et al. Unsafe abortion: the preventable pandemic. The Lancet 2006; 368(9550):1908-1919.
- Appiah-Sekyere P. The Perception of Students on Abortion: A Survey of Senior High Schools in the Sunyani Municipality of Ghana. ABIBISEM: Journal of African Culture and Civilization 2013;4.
- Ma Q, Ono-Kihara M, Cong L, Xu G, Pan X, Zamani S et al. Unintended pregnancy and its risk factors among university students in eastern China. Contraception 2008;77(2):108-113.
- El-Adas A. The Resolution of Unintended Pregnancy among Female Students at the University of Ghana, Legon. A study funded by the National Population Council under Award No. I06.82G, Regional Institute for Population Studies- University of Ghana, Legon, 2007.
- Appiah-Agyekum NN, Kayi EA. Students' Perceptions of Contraceptives in University of Ghana. Journal of Family and Reproductive Health 2013;7(1):39-44.
- Pachankis JE. The psychological implications of concealing a stigma: a cognitive-affective-behavioral model. Psychological bulletin 2007;133(2):328.
- Adanu RM, Tweneboah E. Reasons, fears, and emotions behind induced abortions in Accra, Ghana. Research Review of the Institute of African Studies 2005;20(2):1-9.
- Sinha R, Khan M, Patel BC, Lakhanpal S, Khanna P. Decision-making in acceptance and seeking abortion of unwanted pregnancies. Abortion facilities and post abortion in context of RCH programme Centre for Operations Research and Training, New Delhi 1998.
- Mack JW, Hilden JM, Watterson J, Moore C, Turner B, Grier H et al. Parent and physician perspectives on quality of care at the end of life in children with cancer. Journal of Clinical Oncology 2005;23(36):9155-9161.
- Fossey E, Harvey C, McDermott F, Davidson L. Understanding and evaluating qualitative research. Australian and New Zealand journal of psychiatry 2002;36(6):717-732.
- KCRH. Abortion Questionnaire. Knoxville: Knoxville Center for Reproductive Health 2010. Available at www.kcrh.com/PDFs/Abortion%20Questionnaire.pdf accessed in November 2012
- Coleman PK, Nelson ES. Abortion attitudes as determinants of perceptions regarding male involvement in abortion decisions. Journal of American college health Jan 1999;47(4):164-171.
- Ghana Statistical Services(GSS); Ghana Health Service(GHS); Macro International. Ghana Maternal Health Survey 2007. Calverton, Maryland USA: GSS, GHS, and Macro International 2009. Available www.usaid.gov/pdf_docs/PNADO492.pdf accessed in January 2013
- Paluku JL, Kalisoke S, Wandabwa J, Kiondo P. Knowledge and attitudes about induced abortions among female youths attending Naguru Teenage Information and Health Centre, Kampala, Uganda. Journal of Public Health 2013;5(4):178-185.
- Oshiname FO, Ogunwale AO, Ajuwon AJ. Knowledge and perceptions of date rape among female undergraduates of a Nigerian university. African journal of reproductive health 2013;17(3):137-148.
- Haider S, Stoffel C, Donenberg G, Geller S. Reproductive Health Disparities: A Focus on Family Planning and Prevention Among Minority Women and Adolescents. Global Advances in Health and Medicine 2013.
- Ahiadeke C. Incidence of induced abortion in southern Ghana. International Family Planning Perspectives 2001:96-108.
- Pell C, Meñaca A, Were F, Afrah, NA, Chatio S, Manda-Taylor L et al. Factors Affecting Antenatal Care Attendance: Results from Qualitative Studies in Ghana, Kenya and Malawi. PloS one 2013;8(1):e53747.
- Major B, Cozzarelli C, Cooper ML, Zubek J, Richards C, Wilhite M et al. Psychological responses of women after first-trimester abortion. Archives of General Psychiatry 2000;57(8):777.
- Munk-Olsen T, Laursen TM, Pedersen CB, Lidegaard Ø, Mortensen PB. Induced first-trimester abortion and risk of mental disorder. New England Journal of Medicine 2011;364(4):332-339.
- Elul B. Determinants of induced abortion: an analysis of individual, household and contextual factors in Rajasthan, India. Journal of Biosocial Science 2011;43(01):1-17.
- Republic Of Ghana. Criminal Code, Act 29, §58 - 67 (1960), Government Printer, Accra 1967.
- Republic Of Ghana. Criminal code (Ammendment Law), PNDC Law 102(1985), Information Services Department, Accra, 1986
- Shah IH, Åhman E. Unsafe abortion differentials in 2008 by age and developing country region: high burden among young women. Reproductive Health Matters 6/2012;20(39):169-173.
- Singh S, Sedgh G, Hussain R. Unintended pregnancy: worldwide levels, trends, and outcomes. Studies in family planning 2010;41(4):241-250.
- Sedgh G. Abortion in Ghana. Issues in brief (Alan Guttmacher Institute) 2010(2):1.
- Åhman E, Shah IH. Unsafe Abortion: Global and Regional Estimates of the Incidence of Unsafe Abortion and Associated Mortality in 2008. World Health Organization 2011.
- Tunde AI. Socio-Economical and Sociological Factors as Predictors of Illegal Abortion among Adolescent in Akoko West Local Government Area of Ondo State, Nigeria. Public Health Research 2013;3(3):33-36.
- Payne CM, Debbink MP, Steele EA, Buck CT, Martin LA, Hassinger JA et al. Why Women Are Dying from Unsafe Abortion: Narratives of Ghanaian Abortion Providers. African Journal of Reproductive Health Vol. 17, No. 2, June 2013. 2013;3:118.
- Tagoe-Darko E. “Fear, Shame and Embarrassment”: The Stigma Factor in Post Abortion Care at Komfo Anokye Teaching Hospital, Kumasi, Ghana.

