Keywords
Community-based health insurance; Satisfaction score; Arsinegele; Ethiopia
Introduction
Moving towards the goal of universal health coverage require escalation of service delivery and overcoming significant financial barriers. Nevertheless, globally, every year around 150 million people suffer from financial catastrophe and about 100 million are pushed into poverty because of high out of pocket payments for health care services. Out of pocket expenditure for healthcare is a major problem in low and middle income countries (LMIC), as healthcare financing and access to affordable and effective healthcare is untangle [1].
To achieve the UHC goal and to resolve financial hardship as a result of receiving the health care ,governments set public financing mechanisms from two main sources of funds which are general tax financing and social health insurance contributions.
Both of these mechanisms involve pre-payments into a pooled fund for equitable distribution and most importantly compulsory contributions. This ensures that the healthy and wealthy cross-subsidize the costs of health services for the sick and the poor [1].
From diverse types of health insurances CBHI is one of them. It is an emerging and growing tool for providing financial protection to deprived individuals against health-related events. CBHIs have the following characteristics: voluntary membership, a non-profit objective, they are linked to a healthcare provider, they pool risk, and there is an underlying ethic of mutual aid trust, enrollment, and solidarity [1-12].
CHI has emerged as a valuable alternative to user fees in in rural Sub- Sahara Africa too, by pooling risks and resources at the community level, it promises to ensure better access to health services and greater financial protection against the costs of illness for traditionally excluded and disadvantaged populations which mean for urban and rural self-employed and informal sector workers [3].
Strong evidence shows that CBHI improve service utilization and protect members financially by reducing their out-of-pocket expenditure, and that CBHI improves resource mobilization too [4].
In Ethiopia overall level of catastrophic health expenditure was high among noninsured households when compared to insured one. Hence has significant financial protection from catastrophic health expenditure. The empirical studies which focus on the impact of the insurance, show that CBHI is one of the mechanism that helped to improve health care utilization on top of other variables [13-15].
Ethiopia household out of pocket payments constituted about 37% of the total health expenditure. Such financing is regressive and hold up access to health services. Thus CBHI was launched in June 2011 for rural population and the informal sector in urban areas to reduce household vulnerability to out-of-pocket health care expenditure an increasing quality of services to balance high demand of health care and low supply of medical services basically for rural households and people in urban informal sector, intended to cover 83.6% of the population in 13 districts in the four main regions (Tigray, Amhara, Oromia, and SNNPR) of the country. Then planned to be implemented in two stages, after piloting, it planned to scaled up throughout the country drawing on lessons from the pilot phase [16-20].
The pilot program of CBHI in Ethiopia, households are expected to pay 180 Birr (8.57 US$) annually as a premium. The benefits packages were include all curative and preventive care that is part of the essential health package in Ethiopia [21,22].
Due to the introduced scheme the utilization level of the client were increased, which is 72.3 percent of CBHI members visited health facilities and the likelihood of CBHI members visiting a health facility when feeling sick was 26.3 percentage points higher than that of non-members [23-25].
Alongside assessing utilization level, satisfaction level of the client on the service can have contribution for improvement of the program, improving healthcare services, shaping health policies and providing feedback on the quality, availability, and responsiveness of healthcare services. That is why this particular study focus on clients’ satisfaction to ensure the quality of healthcare services provided by the health insurance scheme which are currently not much available in this context [26].
Methods
Negele Arsi bordered on the south by Shashamene Zuria, on the southwest by Lake Shala which separates it from Shala, on the west from the Southern Nations, Nationalities and Peoples Region, The 2007 national census reported a total population for this woreda of 260,129, of whom 128,885 will men and 131,244 will women; 51,535 or 19.81% of its population will urban dwellers. The study was conducted in Arsi Negele health centers, which is located at north East of West Arsi zone, Oromia region. Arsi Negele is found at southern part, 232 km away from the capital Addis Ababa. The District has eight health centers and there is no hospital in the District. Arsi Negele enrolled community Based health insurance staring from 2008 E.C and until the end of 2010 E.C CBHI district office report they reached 4,460 members and insured households are access health services according to their catchment. According to West Oromia CBHI office report at the end of (2010 E.C) the average enrollment rate of Negele Arsi District reduced from 18.35% to 11.60% (end of 2009 E.C) which is low enrollment and high dropout when compared from other areas which coordinate by the mentioned sector. Institution-based cross-sectional survey study was conducted in Arsi Negele District health centers, west Arsi zone, Oromia, Ethiopia, 2019 [27-30].
Source population
The source population includes all insured clients enrolled during data collection period for quantitative and all concerned sectorial and individuals.
Study population
For quantitative:
The study populations were sampled and randomly selected insured client enrolled during data collection period from the source population.
For qualitative:
Purposively selected individuals from key informants were incorporated such as district health officers (head of health centers, Health care providers, CBHI agency focal persons etc.)
Study unit:
Insured house of head who had taken health service in health centers during data collection period were taken for quantitative and focal person who had concerned regarding to CBHI service were selected for qualitative.
Sampling techniques
Among the health centers found in Woreda two of them are selected based on number of client flow. Accordingly, Kello Dure and Dello health centers selected to increase the representativeness of the targeted population. Systematic random sampling was used to obtain the final study participants and the first client to be included in the study was selected by lottery method and every two client who completed their treatment particularly after they visit drug store of the center were interviewed.
Sample size determination for quantitative:
To determine the required sample size at a confidence level of 95%, and a 0.05 margin of error as given by [23] was considered. The sample size was determined by using single population proportion formula based on taking the Assuming 50% of households enrolled in the CBHI scheme were satisfied with the assumption of 50% of householdssatisfaction with a community-based health insurance scheme in Ethiopia 2016 [6].
Data measurement
For quantitative data
Insured Client who was health center for utilization of Outpatient department (OPD) were interviewed. Pre-test structured questioners were used. The questionnaires were direct primarily who were household heads. A structured questionnaire is adopted from Ethiopian Health Insurance Agency that used for evaluation of community-based health insurance pilot schemes in Ethiopia [15]. It will be translate in to local language (Oromifa) to ease the interview processes. In the questionnaire one major scale determinate to measure; CBHI client satisfaction (satisfaction with health care service they receive from the health center, Health care service provider politeness, waiting time etc.., the collection process of insurance cards, the time to make use of the CBHI program after payment of registration fee, schedule for paying of premium, the information provided, CBHI packages, want to stay enrolled in the CBHI scheme, recommending CBHI scale up to other settings). Then, households was leveled as satisfied if their response lay median score of satisfaction questions otherwise it will leveled as not satisfied.
This were measured by Likert Scale usually five degrees. The respondent may respond in any one of the following ways: (i) strongly agree, (ii) agree, (iii) (neutral)undecided, (iv) disagree, (v) strongly disagree. I found that these five points constitute the scale. At one extreme of the scale there were strong agreement with the given statement and at the other, strong disagreement, and between them lie intermediate points [23]. The overall level of satisfaction with CBHI scheme Six items related to satisfaction on a five point Likert scale (from 1: very satisfied 1 to 5: very dissatisfied) were used to assess CBHI client satisfaction with public health service . Together, all six items produced a maximum score of 30 and a minimum score of 6.
Health service?related factors which were satisfied with laboratory services, waiting, respect from service providers and services providers are friendly. The reliability coefficient (Cronbach’s alpha) of the health services-related factors scale was 0.73 indicating internal consistency.
CBHI process?related factors Household heads were asked four questions on different aspects of CBHI process management on an ordinal scale from ‘strongly disagree’ to ‘strongly agree’ to yield a maximum score of 20 and a minimum score of 4. These four items were based on the following questions: I am satisfied with the opening hours of the CBHI office; I am satisfied with the collection process of insurance cards; I am satisfied with the time to make use of the CBHI program after payment of registration fee; and I am satisfied with the schedule for paying the premium. The reliability coefficient (Cronbach’s alpha) of the CBHI process management factors scale was 0.73 indicating internal consistency [31].
Qualitative data
Qualitative research were an approach conducted for exploring and understanding the meaning individuals or groups attribute to a social phenomenon in which they are experiencing [10]. Then used to investigate the contextualization of community based health insurances design and implementation, quality of health care services and perceptions of health services providers about CBHI scheme on CBHI packages and the factors that affects the satisfaction of the client. Interviews by semi structured questioners were conducted for key informants and also after getting consent the recording of the voice were also taken from some of them and transcript properly and narrated by English [32].
Research Approach
Quantitative and qualitative
These studies were employed combination of mixed research approach which incorporates both qualitative and quantitative approaches. Mixed approach encompasses both quantitative and qualitative data help to comprehensively understand a research problem by addressing multiple interests by triangulate [10]. Triangulation method makes possible to obtain statistical, quantitative data from a representative sample survey, and individuals with CBHI scheme members and health care providers to probe or explore more deep information from qualitative data. Mixed approach resolve between the limitations of both approaches [33].
Sources of data
Primary source of data
Accordingly, the researcher collected primary data through survey and key informant interviews. Since, employing both primary and secondary data on a single research increases the validity, reliability and comprehensiveness of the research secondary data will be incorporated if it is related with pre-sated objectives of this study [23].
Secondary data sources
Official government documents, office reports, service provision manuals, and guidelines concerning community based health insurances, reports of evaluations client satisfaction, and quality of services was reviewed. Ethiopian healthcare financing police through CBHI scheme, mainly, the design and implementation of main parameters in Kebele level health care provision for insured households will critically examine.
Operational definitions
Level of satisfaction: Each question was scored on an ordinal scale from ‘‘strongly satisfaction to strongly dissatisfaction" to yield a maximum score of 20 and a minimum score of
Adverse selection: This is the enrolment of those who are ill or more prone to illness in an insurance scheme compared to the healthier ones.
Capitation: This is a prospective means of paying health care staff based on the number of people they provide care for.
Catastrophic expenditure: This occurs when health care payments force households to borrow heavily, incur debts or to reduce their other basic expenditures on items like food, housing and clothing. A household is considered to be facing catastrophic financial health expenditure when it‘s out-of-pocket health payments is equal or more than 40% of its non-subsistence expenditure or health expenditures in excess of 10 percent of total household consumption.
Community-based health insurance: This is a form of health financing which is usually organized at community level and has outstanding features of being run as a not for profit schemes. It targets the informal sectors and applies the basic principles of risk sharing and members participation in the management of the schemes.
Health insurance policy: This is a contract between an insurance provider (e.g. a private health insurance company and an individual or his/her sponsor e.g. an employer or a community organization). The contract can be renewable (e.g. annually, monthly) or lifelong.
Health insurance scheme: This is an insurance operated by a public agency where the premium takes the form of compulsory contribution which is deducted from the payroll as part of earning. Its membership is compulsory, it is run by public bodies either single or multiple organisations, and has redistribution policies.
Out-of-pocket: This is payment made by a patient directly to the provider at the point of service.
Premium: This is the amount of money the policy-holder or his sponsor (e.g. an employer) pays to the health care pre-payment plan to purchase health care coverage of specified benefits.
Private health insurance: This is a health care pre-payment plan that is taken up and paid for the discretion of individuals or employers on behalf of individuals [34].
Result
Socio-demographic and economic characteristics
A total of 399 respondents were participated in the study and the response rate was 95%. The mean age of the patients were 48.19 (13.87) years. Almost half, 206 (51.6%) of the respondents were Females. Nearly one third, 126(31.6%) of the study participants were Secondary education (Grade 7-12) and more than half, 261 (65.4%) of the participants were married. The majority of the ethnic groups were Oromo and Amahara with 337 (84.5%) and 21(5.3%) respectively. Among the study subjects 307(76.9%) were Muslims followed by Orthodox 65(16.3%) and Protestant 23 (5.8%).Among the respondents 69.2% were Farmer followed by Students 21.3%. More than half, 229 (57.4%) of the study subjects had more than three family size. Nearly half of the participants, 198(49.6%) had an average monthly income of 1001-5000 Ethiopian Birr [35] (Table 1).
| Variables (n=399) |
Frequency |
Percent |
| Age of the patients (Years) |
|
|
| 15-24 |
32 |
8.0 |
| 25-34 |
45 |
11.3 |
| 35-44 |
47 |
11.8 |
| 45+ |
275 |
68.9 |
| Sex of the patients |
|
|
| Male |
193 |
48.4 |
| Female |
206 |
51.6 |
| Name of Health Ceneter |
|
|
| KelloDuro |
202 |
50.6 |
| Dolle |
197 |
49.4 |
| Educational status of the patients |
|
|
| Illiterate |
103 |
25.8 |
| Reading and writing |
76 |
19.0 |
| Primary education (Grade 1-6) |
86 |
21.6 |
| Secondary education (Grade 7-12) |
126 |
31.6 |
| Vocational training |
5 |
1.3 |
| Tertiary education |
3 |
.8 |
| Marital status |
|
|
| Married |
261 |
65.4 |
| Divorce/Separated |
31 |
7.8 |
| Single |
85 |
21.3 |
| Widowed |
22 |
5.5 |
| Ethnic group |
|
|
| Oromo |
337 |
84.5 |
| Amhara |
21 |
5.3 |
| Wolayeta |
11 |
2.8 |
| Kembata |
14 |
3.5 |
| Guragey |
10 |
2.5 |
| Other |
6 |
1.5 |
| Religion |
|
|
| Muslim |
307 |
76.9 |
| Orthodox |
65 |
16.3 |
| Protestant |
23 |
5.8 |
| Catholic |
4 |
1 |
| Occupation of the patients |
|
|
| Employed/Farmer |
276 |
69.2 |
| Non-employed |
16 |
4 |
| Student |
85 |
21.3 |
| Other |
22 |
5.5 |
| Family size |
|
|
| 1-3 peson |
148 |
37.1 |
| >3 |
251 |
62.9 |
| Income (ETB) |
|
|
| <1000 |
78 |
19.5 |
| 1001-5000 |
198 |
49.6 |
| 5001-10000 |
94 |
23.6 |
| >10001 |
29 |
7.3 |
Table 1 Socio-demographic and economic characteristics of CBHI members in Arsi Negele District health facilities from March 25 – May 31, 2019.
The reason for client visit the health facilities
Majority of the respondents 379 (95%) of the CBHI members visit health facilities due to non-infectious disease while 20(5%) where due to infectious diseases and among the prescribed drug majority 304(76.2) of the client got some of them.
Overall Level of satisfaction of CBHI members towards health service in health facilities
To determine the overall level of satisfaction of CBHI members with health service at health facilities, internal consistency (Cronbach’s alpha) was first calculated for the scale items measuring satisfaction: the items had a Cronbach’s alpha of 0.79. The findings of the study showed that the overall client satisfaction level of CBHI with the health services rendered at the health center was 63.4% (95% CI= 26.1-35.2).
Level of satisfaction of respondents with different components of health care services:
Among the Outpatient clients, the way the health care provider examined the clients was the aspect where satisfaction was rated highest 330 (82.7%) and satisfaction was rated lowest (21.8%) which is availability of drugs. Nearly two fifth of the respondents (39%) responded they were not satisfied with the information provision about the health facilities services and the flow.
More than one third (52.4%) of the respondents reported dissatisfaction with the overall waiting time to get the health facility services, while (21.8%) of the clients were dissatisfied with the lack of drugs and supplies in the health facility (Table 2).
| |
Frequency |
Percent |
Cumulative Percent |
| fully (all prescribed) |
92 |
23.1 |
23.1 |
| Partially or some of them |
304 |
76.2 |
99.2 |
| None |
3 |
.8 |
100.0 |
| Total |
399 |
100.0 |
|
Table 2 Getting the prescribed drug/supplies in Arsi Negele District health centers from March 25 – May 31, 2019.
Waiting time of the respondents at different service delivery point
The clients respond that waiting time less than 15 minutes were 342(85.7%), 121(30.3%), 322(80.7%) and 5(1.2%) at card room, consulting room, pharmacy and laboratory respectively. Two hundred and fifty six (62.9%) of the respondents revealed that waiting time at consulting room is greater than 30 minutes whereas waiting time at laboratory were 274(68.8%) (Table 3).
| Characteristics |
V. sat
(%) |
Sat.
(%) |
Neut.
(%) |
Dissat
(%) |
V.dissat
(%) |
| Information provision by health workers |
24.3 |
56.4 |
10 |
8 |
1.3 |
| Time spent to see a health provider |
14.5 |
67.2 |
5.3 |
12.3 |
0.8 |
| Courtesy and respect |
20.3 |
71.7 |
4 |
3.3 |
0.8 |
| Privacy |
24.8 |
51.6 |
6 |
14 |
3.5 |
| Access to latrines |
23.3 |
64.7 |
0 |
11 |
4 |
| Cleanliness of latrines |
17.3 |
21.1 |
2.5 |
57.4 |
1.8 |
| Cleanness of wards |
15 |
42.4 |
5 |
37.6 |
0 |
| Queue process to see health provider |
16.8 |
48.6 |
1.8 |
32.1 |
0.8 |
| The way the health provider examined |
28.1 |
54.6 |
5.3 |
11.3 |
0.8 |
| Confidentiality |
18 |
74.7 |
0 |
4.8 |
3.3 |
| Availability of drugs |
5.8 |
16 |
13.5 |
44.4 |
20.3 |
| Overall waiting time |
8 |
44.4 |
10.5 |
36.6 |
0.5 |
| Visiting hours |
4.5 |
42.6 |
0 |
35.6 |
17.3 |
| Way questions &queries dealt by staff |
24.8 |
37.5 |
10 |
27.5 |
0 |
v.sat = very satisfied; sat = satisfied; neut = neutral; dissat =dissatisfied; v.dissat = very dissatisfied
Table 3 Level of satisfaction of clients with the different components of health care services of CBHI members in Arsi Negele District health facilities from March 25 – May 31, 2019.
| |
Waiting time |
Frequency |
Percentage |
| Card room |
Less than 15minutes |
342 |
85.70% |
| |
Between 15 to 30 minutes |
37 |
9.30% |
| |
More than 30 minutes |
20 |
5.00% |
| |
Total |
399 |
100.00% |
| Consulting room |
Less than 15minutes |
121 |
30.30% |
| |
Between 15 to 30 minutes |
27 |
6.70% |
| |
More than 30 minutes |
251 |
62.90% |
| |
Total |
399 |
100.00% |
| Pharmacy |
Less than 15minutes |
322 |
80.70% |
| |
Between 15 to 30 minutes |
50 |
12.50% |
| |
More than 30 minutes |
27 |
6.80% |
| |
Total |
399 |
100.00% |
| Laboratory |
Less than 15minutes |
5 |
1.3% |
| |
Between 15 to 30 minutes |
120 |
30.10% |
| |
More than 30 minutes |
274 |
68.70% |
| |
Total |
399 |
100.00% |
Table 4 Waiting time at different service delivery point of CBHI members in Arsi Negele District health facilities from March 25 – May 31, 2019.
| Characteristics |
V. sat
(%) |
Sat.
(%) |
Neut.
(%) |
Dissat
(%) |
V.dissat
(%) |
| Voluntarily enrollment |
16.0 |
21.8 |
16.8 |
40.9 |
4.5 |
| CBHI office opening time |
6.0 |
59.4 |
12.3 |
20.1 |
2.3 |
| Satisfaction with paying premium |
9.0 |
74.9 |
11.6 |
2.8 |
1.8 |
| Satisfied with time interval to use benefit package |
17.8 |
71.4 |
6.8 |
2.3 |
1.8 |
Table 5 Level of satisfaction of clients with the CBHI related factors of health care services of CBHI members in Arsi Negele District health facilities from March 25 – May 31, 2019.
Level of satisfaction of clients with the CBHI related factors
Majority of the respondents were satisfied by voluntarily enrollment and CBHI opening time.
Factors associated with poor community based health insurance client satisfaction level towards health service provision
The bi-variant logistic regression analysis revealed thatfactors associated with poor community based health insurance client satisfaction level had association with age of the patients, educational status, waiting time at consulting room, CBHI members who have information about service, waiting time at laboratory, availability of laboratory service and availability of the drug at health facility.
Multivariate logistic regression analysis was carried out in order to identify the independent determinant of poor community based health insurance client satisfaction level. Those variables which had P value of less than 0.25 in bivariate analysis were entered in multivariate analysis. Step wise back ward logistic regression method was employed. In multivariable analysis age of the patients, educational status, waiting time at consulting room, CBHI members who have information about service and availability of the drugs significantly associated with level of satisfaction of CBHI members toward health care service at health facilities [36].
Patients who aged from 15-24 years were 34% less likely to satisfied with service compared to those above 45 years [AOR=0.34 (95%CI= 1.34-8.00)]. The formal educational status [AOR=0.45 (95% CI: 1.56-4.40)], waiting time at consulting room [AOR=1.98 (95% CI: 1.01-3.87)] and availability of the drug at health facility [AOR=4.71 (95% CI: 2.15-10.30)] were significantly associated with level of satisfaction of CBHI members toward health care service at health facilities. CBHI members who have information about service delivered in health facilities were 2 times at risk of satisfied compared to their counterparts [AOR=2.11(95% CI: 1.29-3.47)] (Table 6).
| Variables (n=399) |
Patient Satisfaction |
COR
(95% CI) |
|
satisfied
n |
Not satisfied
n |
AOR (95% CI) |
| Age in years |
|
|
|
|
| 15-24 |
16 |
17 |
0.34(1.13-4.87) |
0.30(1.34-8.00)* |
| 25-34 |
15 |
32 |
1.00(0.52-1.94) |
0.82(0.38-1.76) |
| 35-44 |
19 |
41 |
1.15(0.63-2.12) |
1.05(0.52-2.10) |
| 45+ |
78 |
181 |
1 |
|
| Educational status |
|
|
|
|
| Illiterate |
21 |
39 |
0.47(1.05-5.07) |
0.45(1.95-6.86)* |
| Read and write |
36 |
93 |
1.66(0.83-3.33) |
2.19(0.92-5.27) |
| primary |
27 |
40 |
2.89(1.35-6.18) |
3.05(1.23-7.60) |
| Secondary |
30 |
52 |
2.26(1.09-4.68) |
2.05(0.87-4.84) |
| College and above |
14 |
60 |
1 |
1 |
| Waiting time |
|
|
|
|
| <15minutes |
27 |
120 |
1 |
1 |
| 15 - 30 minutes |
63 |
102 |
2.62(1.56-4.40) |
3.00(1.61-5.37)* |
| >30 minutes |
20 |
45 |
1.98(1.01-3.87) |
2.39(1.12-5.12)* |
| Availability of the drug |
|
|
|
|
| Available( full/partially) |
57 |
183 |
0.43(0.28-0.66) |
0.40(0.24-0.66)** |
| Not available |
71 |
101 |
1 |
|
| Information provision |
|
|
|
|
| Yes |
71 |
108 |
1.94(1.23-2.96) |
2.11(1.29-3.47)* |
| No |
57 |
176 |
1 |
|
NB: 1- Reference group; *= P<0.05; **= P<0.0
Table 6 Results in multivariable logistic regression showing determinants of level of satisfaction among CBHI members visiting health facilities in Arsi Negele District, Oromia region, March 25 – May 31, 2019.
Results of Key informants
The Fifty (15) key informants involved in the study included: Arsi Negele District health Officer (THO), HF (CBHI) manager, 2 PHCU head, 2 Health care provider (HCP), 1 community member representative(CMR) and Woreda Health Officer (DHO). The results of the interviews were consolidated and their responses quantified. Figure 1 given in brackets indicate the number of quotes that were collected pertaining to the specific issue. For example, the index (CP 1) indicates that one quote with the specific issue of concern was collected from a chair person and (CP 2) denotes two quotations from two chair persons. The same applies to interviews from key informants. Plain numbers between brackets, for example (10), indicate that the issue was directly mentioned ten times in the interviews. Similarly, (1) is used to indicate one quote regarding an issue of concern collected from key informant with a scheme [37].
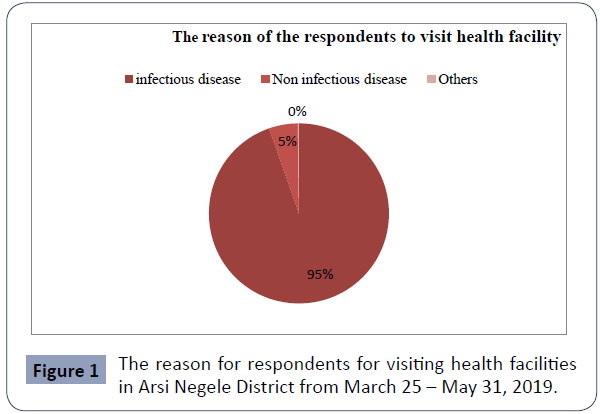
Figure 1 The reason for respondents for visiting health facilities in Arsi Negele District from March 25 – May 31, 2019.
All (15) key informants said the majority of the CHIS enrollees’ education qualification level was below secondary school certificate.
‘’This scheme is for people who didn’t go to school and have low income. If they don’t afford three meals per a day, what about quality of medical care?” (CBHI manager).
“One of the objectives of the CBHI is to improve incomes of poor and informal families in the target communities to meet their health financing need” (one of the officials of Dolle health center said).
The essential medicines reported to be available at all times and were rarely out of stock (MS1, THO1, HCP2, CP1, and CBHI manager 1). On the other hand, the key informants felt the following were lacking/deficient in the facility: The ambulance services is not fully utilized by patients (CBHI manager, VCBHI).
The DHO suggested that the government employed health officers should also give more attention to CBHI members visiting health facilities.
Majority of the key informants were satisfied with the services provided under the scheme (THO 1, CP2, HCP2,CBHI manger 1) and only one key informants was dissatisfied (VHCP 1).
“The scheme does not cover all disease such as tooth related treatment and almost half of the prescribed drugs are not available in drug store therefore the clients are not utilized the card for getting drugs as they purchase from the town pharmacy “(2 PHCU Head and 1 CMR).
To improve the quality of outpatient care and to increase the satisfaction level of CBHI members on the service they get they recommended: employing more staff as reduce waiting time as utilization is increased due the insurance and especially at least one health professional should have to be assigned for CBHI program at health center level to facilitate the whole process (THO1, HCP1, and CP1), continues training of existing staff on client care behavior, easy financing system on reimbursement and other strategies should have to be created on drug issues such as creating link with private pharmacies to deliver drugs to clients who couldn’t get in the compound (2 PHCU head, HCP & CMR)
With regards to health care provider- patient relationship, majority (5) of the participants were satisfied with the services of the professional with commendations such:
“The health care provider listens to the patients’ problems before examination and prescribing drugs as said by one of the patient’s care taker. The health care providers thoroughly carry out physical examinations on the patients on consultation rooms,” noted by one of the officials of the health center.
On what they found missing/deficient in this facility: the main pressing issue according to some of the health care provider (CT8) was to do with few high case load in the facilities in the different departments [38].
“There are high case load after implementations of CBHI only,” said by a health care provider.
Discussion
This study has revealed that the overall satisfaction level of the clients with the services rendered at Health facilities in Arsi Nagele District is 63.4 % and this is higher than reports from other studies conducted in Jimma District which showed 57.1% [17] and lower than the study conducted in Damotwoyde district is located in the Wolaita zone which was 98.2 % of household heads reported that they were happy with the permitted healthcare institutions quality [6]. The difference might be attributed to the fact that this study was conducted in a health facilities where there are relatively adequate number of health professionals and better diagnostic facilities may exist and also where CBHI is fully implemented and the other lower result can be due to study place of this study which reduce remembering risk as it conduct in facility. In addition, study time and design might have also contributed. The overall high satisfaction rate shown here may help and encourage to scale up of the CBHI scheme and service quality in rural part of the country as there is evidence that CBHI increases healthcare utilization [12].
In this study, age was associated with CBHI satisfaction which is patients who aged from 15-24 years were 34% less likely to satisfied with service compared to those above 45 years; in a similar study in Nigeria, older clients were more satisfied with service provision than younger clients [28]. Also the study conducted in on patient satisfaction of national health insurance showed that there was a significant relationship between gender, marital status, education level, and occupation [29].
The study has revealed that lack of drugs and supplies in the health center pharmacies was the major problem, as getting all prescribed drug only 23.1% of the clients get which is lower than the study conduct in one of the pilot district South Ethiopia has which was 96.4%. This finding reveled that in which health care service that the CBHI program should accent [6]. However, our finding has similar fining with that of the study conducted in the hospitals of the Amhara region where about 1/3rd of the clients did not get the prescribed drugs [7].
Failure to obtain the prescribed drugs from the health facilities pharmacy is in line with a report from a study conducted in South Africa also revealed that access to drugs was one of the most suggested priorities for improvement of public health services and associated with lower satisfaction [8].
Twenty percent of the clients in the present study were dissatisfied with the provision of information about the health centers services and their health problems. This is quite a low dissatisfaction rate when compared to the study conducted in Tigray zonal hospitals with 46.7% dissatisfaction rate [9]. The reason for the big difference could be due to the difference in the number and type of health care providers in those mentioned service delivery places and the variety of activities they run in their respective areas.
Highest satisfaction rate (82.7%) is founded regarding to the way the health care providers examined the clients which are similar finding with the study conducted in Ghana which insured patients are satisfied with the overall quality of care:waiting time, friendliness of staff and satisfaction of the consultation process [1] and higher than the study conducted in Turkey were 53.6% satisfied by humaneness of health care provider [3]. Then in Burkina Faso CBHI members’ has poor perception on their healthcare provider which become an important reason for dropping out of the Nouna Community Based Insurance scheme too [33]. The variation may be due to health professionals at different level are expected to demonstrate the standard way of patient examination.
Similar study conducted in south Wollo Zone Tehuledere district has similar finding with the qualitative finding of this study in the following variable: CBHI introduction increased overall quality of health services especially, laboratory services, referral system and cleanness of the facilities and in contrary as PHCUMs explanation; CBHI brings high utilization or patient in flow brings low quality of services and brings long waiting time, drug shortage and miss treatment as professionals shortage is the main fissure [21].
The qualitative finding of this study also found that CBHI process, reimbursement and drug availability,service quality particularly with respect to CBHI office opening times, the membership card collection process, waiting time and corruption (management) were significantly associated with CBHI satisfaction as the study conduct on Kenya’s Kilifi [8].
key informants response both in this study and in other study conduct in east Gojjam Zone, Anededworeda reveal that providing quality health service is the one purpose of the scheme, nonetheless it is not achieved specially in terms of quality, drugs,equipment, skillful health service delivery professionals [34]. From this the investigator concludes that absence of quality health service at health center has its own contribution for poor satisfaction of CBHI members.
Conclusion
The level of satisfaction among CBHI client was low 63.4% compared to the national as more than 80% of the CBHI members were satisfied or very satisfied by the diagnosis, the cleanliness of the facility, and the courtesy of the staff [15]. Thus age, family, laboratory services, service provider friendliness, drug and supply availability, waiting time to receive service and drug unavailability were the main indictors of CBHI members’ poor satisfaction in this study, with this finding the following concerned bodies need to improve their service accordingly.
Competing Interests
The authors have declared that no competing interests.
Data Availability
The data will be available upon request.
Funding
This study had not specific fund.
Authors’ Contributions
GF, AY, AT and TE developed the concept and method, collects data and drafts the manuscript, analyzed and interprets the data.
Acknowledgments
We are grateful to Madda Walabu University for supporting this study. We are also very grateful to mothers and data collectors to undertake this study.
37655
References
- Fenny A, Enemark U, Asante F, Hansen K (2014) Patient Satisfaction with Primary Health Care – A Comparison between the Insured and Non-Insured under the National Health Insurance Policy in Ghana. Global Journal of Health Science6.
- Jadoo SAA, Puteh SEW, Ahmed Z, Jawdat A (2012) Level of Patients’ Satisfaction toward National Health Insurance in Istanbul City (Turkey). World App Sci J 17:976–985.
- Ali EE (2014) Health care financing in Ethiopia: implications on access to essential medicines. Value Health Reg Issues 4: 37-40.
- Anagaw DM, Robert S, Zelalem Y, Getnet A, Arjun SB (2015) Enrollment In Ethiopia’s Community-Based Health Insurance Scheme. World Development 74: 58–76.
- Badacho AS, Tushune K, Ejigu Y, Berheto TM(2016) Household satisfaction with a community-based health insurance scheme in Ethiopia. BMC research notes 9: 424.
- Bernhat HM, Wiadnyana IGP, Wihardjo H, Pohan I (1999) Patient satisfaction in developing countries. Soc Sci Med 48:989–996.
- Catherine M, Beryl H, Jane C, Lucy G (2007)The role of community-based organizations in household ability to pay for health careminKilifi District, Kenya. Health Policy Plan 22:381–392.
- Chuma J, Musimbi J, Okungu V, Goodman C, Molyneux C (2009) Reducing User Fees For Primary Health Care In Kenya: Policy On Paper Or Policy In Practice? Int J Equity Health 8: 15.
- Creswell JW, Creswell JD(2017) Research design: Qualitative, quantitative, and mixed methods approaches. Sage publications.
- CSA (2014) Ethiopia Demographic and Health Survey. Addis Ababa: Ethiopia.
- Derseh A, Sparrow R, Debebe Z, Alemu G, Bedi A (2013) Enrolment In Ethiopia’s Community Based Health Insurance Scheme. International Institute of Social Studies of Erasmus University pp: 1–35.
- Devadasan N, Criel B, Damme W, Lefevre P, Manoharan S, et al. (2011) Community Based Health Insurance And Patient Satisfaction—Evidence From India. Indian J Med Res 133: 40-49.
- Dror D, Hossain S, Majumdar A, Pérez KT, John D, et al.(2016) What Factors Affect Voluntary Uptake Of Community-Based Health Insurance Schemes In Low- And Middle Income Countries? A Systematic Review and Meta-analysis. Plos One 11: E0160479.
- Ethiopian Health Insurance Agency(2015) Evaluation of Community-Based Health Insurance Pilot Schemes in Ethiopia: Final Report. Addis Ababa, Ethiopia.
- Fadlallah R, El-Jardali F, Hemadi N, Morsi RZ, Samra CAA, et al. (2018) Barriers and facilitators to implementation, uptake and sustainability of community-based health insurance schemes in low-and middle-income countries: a systematic review. Int J Equity Health 17: 13.
- Assefa F, Mosse A, Hailemichael Y (2011) Assessment of Clients’ Satisfaction with Health Service Deliveries at Jimma University Specialized Hospital. Ethiop J Health Sci 21: 101–109.
- Tesfay G (2014) The impact of community based health insurance in health service Utilization in Tigray: A Case of kilte Awlaeloworeda. Mekelle University.
- Gottret P, Schieber G, Waters HR(2008) Good practices in health financing: lessons from reforms in low and middle-income countries. The World Bank.
- Jadoo SAA, Puteh SEW, Ahmed Z, Jawdat A (2012) Level of patients’ satisfaction toward national health insurance in Istanbul city (Turkey). World Applied Sciences Journal 17: 976-985.
- Jembere M (2018) Community Based Health Insurance Scheme As A New Healthcare. Financing Approach in Rural Ethiopia: Role On Access, Use And Quality Of Healthcare Services, The Case Of Tehuledere District, South Wollo Zone, Northeast Ethiopia. Fam Med MedSci Res 7: 227.
- Kebede KM, Geberetsadik SM (2019) Household satisfaction with community-based health insurance scheme and associated factors in piloted Sheko district; Southwest Ethiopia. PLoS One 14: 1–13.
- Kothari CR (2004) Research methodology: Methods and techniques. New Age International.
- Mebratie AD (2015) Essays on evaluating a community based health insurance scheme in rural Ethiopia. ISS PhD Theses. International Institute of Social Studies of Erasmus University (ISS).
- Mebratie AD, Sparrow R, Yilma Z, Alemu G, Bedi AS (2015) Enrollment in Ethiopia’s community-based health insurance scheme. World Development 74: 58-76.
- Ronald M (2014) Client Satisfaction With Health Care Services Of A Community Health Insurance Scheme.International Health Sciences University.
- Mohammed S, Sambo MN, Dong H (2011) Understanding client satisfaction with a health insurance scheme in Nigeria: factors and enrollees experiences. Health Res Policy Syst 9:20.
- WHO(2003) Community based health insurance schemes in developing countries: facts, problems and perspectives. Geneva.
- WHO(2008) 2008 Report on the Global AIDS Epidemic, World Health Organization.
- WHO(2010)The world health report: health systems financing: the path to universal coverage: executive summary. Geneva.
- Rad EH, Kavosi Z, Moghadamnia MT, Arefnezhad M, Arefnezhad M, et al. (2017) Complementary health insurance, out-of-pocket expenditures, and health services utilization: A population-based survey. Med J Islam Repub Iran 31: 59.
- Robyn PJ, Bärnighausen T, Souares A, Savadogo G, Bicaba B, et al. (2013) Does enrollment status in community-based insurance lead to poorer quality of care? Evidence from Burkina Faso. Inter J Equity Health 12:31–32.
- Tesfagiorgis E(2016) The Impact of Community-based Health Insurance on Health Service Utilization in AnededWoreda.
- Wang H, Pielemeier N (2012) Community-based health insurance: An evolutionary approach to achieving universal coverage in low-income countries. Journal of life sciences 6: 320-329.
- Andinet W, Zerfu GD, Abebe S (2016) Community-based health insurance and out-of-pocket healthcare spending in Africa: Evidence from Rwanda.
- Vialle-Valentin CE, Ross-Degnan D, Ntaganira J, Wagner AK (2008) Medicines coverage and community-based health insurance in low-income countries. Health Res Policy Syst 6:11.
- Yismaw M (2017) Role of Community Based Health Insurance on Health Service provision and Healthcare Seeking Behavior of Households in Rural Ethiopia: the Case of Tehuledere District, South Wollo Zone. Addis Ababa University.

