Keywords
Coronary artery bypass grafting; Quality of life; Nurse; SF-36
Introduction
Coronary artery disease is the most common disease and one of the leading cause of death worldwide [1]. Coronary artery bypass grafting is one of the primary treatment for this disease, [2,3] and is referred as one of the most common surgical procedure in the United States [4]. In Greece, it is considered a routine operation used in patients with coronary artery disease [5].
Quality of life is a complex concept and is eluded a universally definition [3]. It is defined as a multi-dimensional assessment of an individual’s perception of the physical, psychological and social aspects of life that can be affected by a disease process and its treatment [6]. Cella & Nowinski has been defined it in chronic illness as “a summary aggregation of a broad array of life conditions and circumstances, such as environmental conditions, social surroundings, physical conditions and personal resources that include mental health and life perspective” [7]. The coronary artery bypass has an impact on physical and mental health status and generally in quality of life [2].
In recent years, there has been a growing concern about assessing quality of life in patients underwent coronary artery pass graft surgery. Some of them are primarily focused on assessing it in postoperative period [2,8-10]. It was found that quality of life is remained to the same level in pre- and postoperative period [8]. Merkouris et al., investigated the quality of life after 4 and 12 months after coronary artery bypass graft and found that a high percentage of patients reported improvement in all domains of their quality of life while a substantial number reported signs of cognitive dysfunction [10]. Other researchers reported that the health status of patients underwent surgery presented a statistically significant improvement in half of the domains of physical and mental health compared with the preoperative status [2]. In the same results is ended up by Linsday et al., in their research that conducted in 240 patients underwent coronary artery bypass graft surgery [9].
Various studies on investigating the factors that affected the quality of life have demonstrated there is relationship between quality of life and psychosocial [11,12], demographic factors [11,13,14] and patient related characteristics [11,14]. It was found that factors such as ggender [11,15], diabetes mellitus, low ejection fraction, emotional reaction, sleep, affected quality of life [11]. As it is observed from the literature gender plays an important role in adjustment in life after the surgery [16] and women experienced significant disruption to their life [17]. Jokinen et al., [14] in their review of randomized controlled trials reported patient-related characteristics (e.g. demographics and underlying comorbities), surgical technique-related factors and health care –related attributes are contributors that affect preand postoperative self-perceived quality of life [14].
Furthermore, there are many studies that examined quality of life among patients underwent coronary artery bypass grafting and significant others [18,19]. Rantanen et al., [18] in one longitudinal study assessed the quality of life of both patients and significant others one, six and twelve months after surgery. They found improvement of quality of life in both groups and this improvement is greater in patients than in significant others. In a similar study, it was investigated the factors that affect the quality of life in these groups. Cardiac symptoms on physical exertion and other additional diseases are the explanatory factors among patients whereas chronic diseases were associated with quality of life among significant others [19].
Quality of life in patient undergoing coronary artery bypass grafting has been attracting the interest of Greek nurse researchers since the 2000’s [20]. Also, there is a great deal of evidence on this subject [10,20,21]. Nevertheless, most of the published studies have been carried out in Athens the capital of Greece and they are conducted in majors Hospitals of Athens [10,20]. These reasons stimulated the researchers’ interest to investigate the phenomenon further.
Aims
The aim of the present study was a) to investigate the quality of life of patients underwent coronary artery bypass graft after six months of it b) to determine factors influencing the quality of life of these patients.
Methods
Sample and setting
The design of the study was non-experimental, descriptive and prospective. Data were collected between March 2009 and September 2010. The sample was convenience and consisted of 84 patients underwent coronary artery bypass grafting surgery (CABG) in one hospital of a major city in Northern Greece. The sample was recruited after six months of the surgery. Inclusion criteria for participation in the study were: 1) underwent surgery before six months 2) willingness to participate 3) being over 18 years old 4) having the ability to speak and read Greek.
The total number of patients underwent the surgery at major hospital was 290 during 18 month period that the study was undertaken. The study patients represented a convenience sample of all patients who underwent surgery meeting the above criteria.
Procedure
Ethical approval for the study was received by the hospital authorities, which are acting as an ethics committee. Permission to access the particularly clinical setting was given by the same authorities.
Patients were assessed 6 months after the operation during their visit in the hospital for medical reappraisal. The potential participants were approached by a member of the research team. The study aims were explained and the patients were asked if they were willing to participate. An informed consent was obtained from those who agreed to participate and to the patients was given the opportunity to ask questions about the study. A total of 90 questionnaires were distributed and finally 84 agreed to participate in the study (response rate of 94%).
Instruments
Data were collected with a questionnaire that included the SF- 36 and socio-demographic characteristics. Socio-demographic variables included gender, age, country of birth, main language spoken, marital status, number of people in the household, school leaving age, highest level of education, current employment status, and current or last occupation.
The sf-36 health status survey is a 36 –item, standardized quality of life assessment tool. It consists of 36 multiple choice questions that measures eight health constructs: physical functioning (10 items), physical role functioning (role physical)/role limitation due to physical problems (four items), bodily pain (two items), general perception of health (five items), energy and vitality (four items), social functioning (two items), emotional role functioning (role emotional)(three items) and mental health (five items). Scores are converted to a 0-100 scale, which allows us to measure the scales numerically. Higher values on the transformed 0–100 scale for each health domain indicate better health status. The lowest scores indicate the lowest state of health and show functional limitation, severe social and role disability, and distress. High scores indicate the absence of limitations and disability [22,23]. The internal consistency of the questionnaire was checked by Cronbach’s alpha and proved to be good (Cronbach’s alpha=0.89).
Data analysis
Statistical analysis was carried out using SPSS for Windows (Release 15.00). For analyzing demographic and social characteristics of the sample were used descriptive statistics. Kolmogorov- Smirnov test was performed in order to check if the values of the sample have a normal distribution. For correlation analysis was used Pearson’s rho in order to investigate the relation between patients’ characteristics and the domain of quality of life. Also, a linear regression analysis was used. The internal consistency reliability of the scales was estimated by Cronbach’s alpha [24].
Results
The participants were 84 patients in the hospital in a major city of Northern Greece. The sample was predominately male (n= 61, 72, 6%) and a high percentage of them is above 50 years (85, 7%). Most of them were married (n=72, 85, 8%) and had a primary educations (n=45, 53, 6%). The majority of them (n= 13, 15, 5%) were employee, retired (n=11, 13, 1%) and housekeepers (n=23, 27, 4%). Table 1 presents the demographic and educational characteristics of the sample. The patients co- morbidities are hypertension (n=24, 28, 6%), diabetes mellitus (n=13, 15, 5%), history of angina (n=12, 14, 3%). Also the majority of the sample do not smoke (n= 72, 87, 5%).
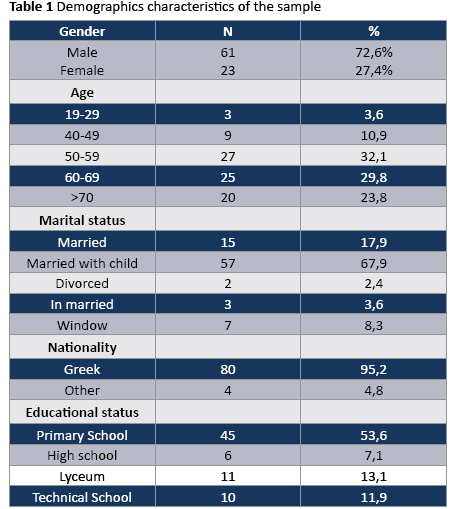
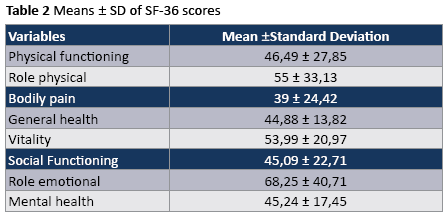
Table 2 shows means and standards deviations. The variables that have higher means are the followings: role emotional (68, 25 ± 40, 71), role physical (55 ± 33, 13), vitality (53, 99 ± 20, 97) and social functioning (45, 09 ± 22, 71).
Τable 3 presents the factors influence the domains of quality of life. According to Pearson’s rho criterion it was estimated that social role is influenced directly by patients’ sex (p=0, 15), nationality (p=0, 13), occupational status (p=0, 16) and smoking (p=0, 32). Physical role is affected by family status (p=0, 50) and educational status (p=0, 45). In addition, vitality is influenced by sex (p=0, 50), nationality (p=0, 29) and comorbities (p=0, 24) whereas general health is influenced by nationality (p=0, 18) and smoking (p=0,41). Role physical is affected by occupational status (p=0, 31), mental health is influenced by age (p=0, 31), educational status (p=0, 40) and occupational status. Finally, emotional role is affected only by educational status (p=0, 03) and smoking (p=0, 16).
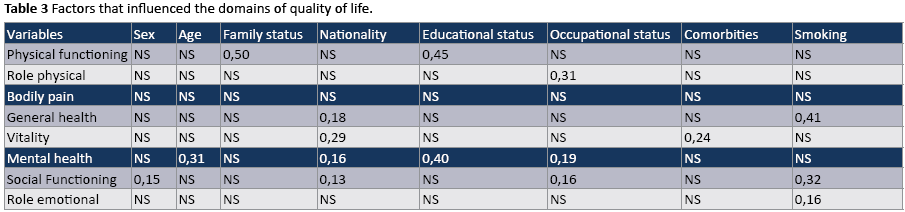
Table 4 illustrates frequencies of the answers about rating their health compared one year ago. The majority of the subjects (N=35, 41, 7%) stated that their health is about the same, while the 23, 8% (N=20) said that their health is somewhat better now than one year ago. Percentage of 14, 3% (n=12) stated that their health is much worse than one year ago, 13, 1% (n=11) said that their healthy is somewhat worse now than one year ago and a little percentage of 7,1% (n=6) stated that it is much better now than one year ago. In Figure 1 is depicted the percentages of the answers in a bar chart.

Table 5 shows the results of a linear regression analysis. By applying linear regression analysis, it was revealed that where quality of life was examined in relation with patients’ characteristics, it was found that it is affected by age (p=0,049). Specifically, it was revealed that for every increasing unit of age, quality of life was increased 2,471 times.

Discussion
Quality of life is an important issue for patient underwent coronary artery bypass grafting because the person has to learn how to leave with the consequences of the primary disease. Generally, there are many studies assessed quality of life three, six, twelve months after surgery [25]. This study has contributed to the assessment of quality of life in patients underwent this kind of surgery and live in a major city of Northern Greece. The SF-36 health measure was used as the main health outcome measure and demonstrated a median level of quality of life. The majority of the sample was male and married. This is consistent with other Greek studies that conducted in elderly population after coronary artery bypass graft surgery. Also, it is an expected outcome because males are in higher risk to suffer from coronary artery disease and undergo this kind of surgery [26].
According to the findings of the research the comorbities of the patients were hypertension, diabetes mellitus, and history of angina. This is similar with the findings of other studies that reported the same comorbidities [4,9]. There is a need for further research in greater population with special clinical tools in order to determine precisely the comorbidities and how these are associated with quality of life or general health status in this group of patients.
In this study, the mean scores of the SF-36 subscales varied between 39 and 68, 25. The patients had lower scores for physical functioning, bodily pain, social functioning, mental health and this finding is consistent with one research [3] in which assessed the quality of life after six months of the surgery [3] Low scores proved the statement of Danta & Ciol “individuals with coronary artery disease who underwent CABG surgery and who low values for at least one of the three subscales may be candidates low selfperceived quality of life” [3].
In this study, patients had lower scores for almost all subscales of SF-36 when compared to other studies that evaluated the patients 12 month after surgery. [3,9]. This observed difference may be happened because of the longer follow –up time after surgery. However, if the median health scores reflects reality and is experienced more widely, it is important for health care professionals to incorporate in their decision-making this result. Therefore, further research is needed in order to clarify this particular issue that is connected with follow-up time.
The correlation analysis of demographic and various patients’ characteristics has highlighted some interesting associations. The correlation between sex vitality and social role perspectively is an expected outcome because in other studies sex is reported as an important factor that affected overall the quality of life [8,11,15]. In addition, the correlation between age, occupational and educational status with mental health is consistent with the support that age, unemployment and lower socio-economic status have been associated with poorer mental quality of life [27]. Another interesting finding of this study is that educational status affected physical role, mental health, emotional role and vitality is affected by comorbidities. This is partially consistent with the statement of Thompson et al according to with non-randomized studies suggest less education, previous myocardial infraction are factors that contribute significantly to patients’ poorer quality of life after coronary artery bypass grafting surgery [28,29]. Also, smoking affected general health, social role and emotional role is consistent with the finding of other studies [27]. Furthermore, family status influence physical role and this is consistent with the finding of Colak et al., [2] in which surgical, neurological and psychological complications after surgery in conjunction with offerings to family affected significantly the physical role. The results show that there is a correlation between nationality and some subscales such as general health, vitality, mental health. Although there is a specific correlation, we cannot draw safe conclusions because there few other nationality’s patients in this study group. It is worthwhile to mention that the size of the sample of other nationalities is very small so we cannot draw safe conclusions. Therefore, further research is needed in order to conclude if the nationality is an important factor influence quality of life.
The majority of patients stated their health is about the same or somewhat better compared it with one year ago. This study is not longitudinal and it has asked patients to recall their health status before surgery. This is susceptible as an optimism bias because patients after surgery or after major treatment incline to believe that treatment made them better [8]. Therefore, there is a great need for further longitudinal research in order to investigate health status before surgery and six months after it.
One arising subject that emerged from regression analysis is that age was the only one statistically significant factor contributing to overall quality of life (all domains of SF-36). A possible explanation for this finding is that age is a potential risk factor for coronary artery disease. Also, this is not consistent with the findings of other studies [9,11] in other studies it was found that social network was the most important factor contributing to general health status post-operatively [9] and Baig et al., in their systemic review reported the importance of family support in improving quality of life [6]. This difference may be attributed to different research method that used, the different patient characteristics and the time is conducted the different follow-up time that conducted the research. Our study cannot explain this observing difference and we believe that more research is needed to clarify this particular issue.
Limitations of the study
The questionnaire was distributed only in one hospital situated in a major city of Northern Greece. So we cannot safely generalize our results to the entire population underwent coronary artery bypass grafting surgery in Greece. Furthermore, the conclusions of the present study are somewhat limited because this research is not longitudinal and we cannot assess the trajectory of health status before and after surgery. Future longitudinal studies need to assess populations all over the country in order the results could be generalized to the Greek population.
Conclusions
The results of the present study have shown that quality of life in patients underwent coronary artery bypass grafting is affected. The main domains, related with the quality of life, that affected are physical functioning, bodily pain, social functioning and mental health, so health care professionals have to plan interventions to improve it. Also, nurses should frequently assess the patients, encourage patients and their family and promote their families to participate in the process of patients’ rehabilitation. Furthermore, although the present study cannot draw safe conclusions about all domains of quality of life in patients all over Greece, we believe that the findings of our research may be of interest to multidisciplinary team in order to intervene efficiently in improvement of quality of life.
3799
References
- Pyrgakis VN (2009) Mortality from coronary artery disease in Greece: where in Europe do we belong? Hellenic J Cardiol 50: 161-163.
- Colak Z, Segotic I, Uzun S, Mazar M, Ivancan V, et al. (2008) Health related quality of life following cardiac surgery--correlation with EuroSCORE. Eur J Cardiothorac Surg 33: 72-76.
- Spadoti Dantas RA, Aparecida Ciol M (2008) Quality of life after coronary artery bypass surgery. West J Nurs Res 30: 477-490.
- Rumsfeld JS, Ho PM, Magid DJ, McCarthy M Jr, Shroyer AL, et al. (2004) Predictors of health-related quality of life after coronary artery bypass surgery. Ann Thorac Surg 77: 1508-1513.
- Michalopoulos A, Tzelepis G, Dafni U, Geroulanos S (1999) Determinants of hospital mortality after coronary artery bypass grafting. Chest 115: 1598-1603.
- Baig K, Harling L, Papanikitas J, Attaran S, Ashrafian H, et al. (2013) Does coronary artery bypass grafting improve quality of life in elderly patients? Interact Cardiovasc Thorac Surg 17: 542-553.
- Cella D, Nowinski CJ (2002) Measuring quality of life in chronic illness: the functional assessment of chronic illness therapy measurement system. Arch Phys Med Rehabil 83: S10-17.
- Covinsky KE, Lin F, Bittner V, Hlatky MA, Knight SJ, et al. (2008) Health-related quality of life following coronary artery bypass graft surgery in post-menopausal women. J Gen Intern Med 23: 1429-1434.
- Lindsay GM, Hanlon P, Smith LN, Wheatley DJ (2000) Assessment of changes in general health status using the short-form 36 questionnaire 1 year following coronary artery bypass grafting. Eur J Cardiothorac Surg 18: 557-564.
- Merkouris A, Apostolakis E, Pistolas D, Papagiannaki V, Diakomopoulou E, et al. (2009) Quality of life after coronary artery bypass graft surgery in the elderly. Eur J Cardiovasc Nurs 8: 74-81.
- Peric V, Borzanovic M, Stolic R, Jovanovic A, Sovtic S, et al. (2008) Predictors of worsening of patients' quality of life six months after coronary artery bypass surgery. J Card Surg 23: 648-654.
- Peric V, Borzanovic M, Stolic R, Jovanovic A, Sovtic S, et al. (2008) Predictors of worsening of patients' quality of life six months after coronary artery bypass surgery. J Card Surg 23: 648-654.
- Škodová Z, van Dijk JP, Nagyová I, Rosenberger J, Ondušová D, et al. (2011) Psychosocial predictors of change in quality of life in patients after coronary interventions. Heart Lung 40: 331-339.
- Sawatzky JA, Naimark BJ (2009) The coronary artery bypass graft surgery trajectory: Gender differences revisited. Eur J Cardiovasc Nurs 8: 302-308.
- Jokinen JJ, Hippeläinen MJ, Turpeinen AK, Pitkänen O, Hartikainen JE (2010) Health-related quality of life after coronary artery bypass grafting: a review of randomized controlled trials. J Card Surg 25: 309-317.
- Tung HH, Wei J, Chang CY (2007) Gender differences in quality of life for post coronary artery bypass grafting patients in Taiwan. J Nurs Res 15: 275-284.
- Banner D, Miers M, Clarke B, Albarran J (2012) Women's experiences of undergoing coronary artery bypass graft surgery. J Adv Nurs 68: 919-930.
- Banner D (2010) Becoming a coronary artery bypass graft surgery patient: a grounded theory study of women's experiences. J Clin Nurs 19: 3123-3133.
- Rantanen A, Tarkka MT, Kaunonen M, Tarkka M, Sintonen H, et al. (2009) Health-related quality of life after coronary artery bypass grafting. J Adv Nurs 65: 1926-1936.
- Rantanen A, Kaunonen M, Tarkka M, Sintonen H, Koivisto AM, et al. (2009) Patients' and significant others' health-related quality of life one month after coronary artery bypass grafting predicts later health-related quality of life. Heart Lung 38:318-322
- Merkouris A, Diakomopoulou E, Papagianaki V, Argiriou M, Apostolakis E (2002) Quality of life after coronary artery bypass grafting pilot study. Nosileftiki 41:337-349
- Merkouris A, Apostolakis E, Pistolas D, Papagiannaki V, Diakomopoulou E, et al. (2009) Quality of life after coronary artery bypass graft surgery in the elderly. Eur J Cardiovasc Nurs 8: 74-81.
- Ware JE (1997) SF-36 Health Survey Manual and InterpretationGuide: Introduction. Medical Outcome Trust Boston, USA.
- Ware JE Jr (2000) SF-36 health survey update. Spine (Phila Pa 1976) 25: 3130-3139.
- Morrison EF (1993) The measurement of aggression and violence in hospitalized psychiatric patients. Int J Nurs Stud 30: 51-64.
- Aydin S, Yavuz T, Duver H, Kutsal A (2006) Quality of life in the elderly after coronary bypass surgery. Int Heart J 47: 59-65.
- Le Grande MR, Elliott PC, Murphy BM, Worcester MU, Higgins RO, et al. (2006) Health related quality of life trajectories and predictors following coronary artery bypass surgery. Health Qual Life Outcomes 4: 49.
- Thomson P, Niven CA, Peck DF, Eaves J (2013) Patients' and partners' health-related quality of life before and 4 months after coronary artery bypass grafting surgery. BMC Nurs 12: 16.

