Keywords
Health education; Hemorrhage; Reproductive health
Introduction
Background
Female genital mutilation (FGM/C) or female circumcision, includes all procedures involving partial or total removal of the external female genitalia or other injuries to the female genital organs whether for cultural or other non-therapeutic reasons [1,2]. There are four main types of FGM/Cs:
Type 1: Clitoridectomy/Sunna involves the removal of the clitoral hood with or without removal of all or part of the clitoris.
Type 2: Excision varies from the removal of the clitoris and/or clitoral prepuce to the removal of part or the entire clitoris together with part or all of the labia minora (the inner vaginal lips).
Type 3: Infibulation involves the removal of the clitoris, the labia minora, and part of the labia majora after which the edges of the wound are sutured to leave a small opening (vaginal orifice).
Type 4: Unclassified and the intermediate practice refers to the amputation of the clitoris and parts of the labia minora [2-4]. Among the four types, Type 2 is commonest while the most extreme is type 4 [1].
There have been no comprehensive global surveys of prevalence of FGM. However, WHO estimated that 132 million of girls and women have under gone the operation and two million girls are at risk each year in 28 African countries including Ethiopia with estimated prevalence of 90% [1,2].
The health consequences vary according to the type and severity of the procedure performed. The immediate complications include severe pain, shock, hemorrhage, urine retention and injury to adjacent tissue or death. Long-term consequences include urinary incontinence, painful sexual intercourse, sexual dysfunction, difficulties with childbirth, scaring and infertility [3]. Worldwide, between 100 and 140 million girls and women had experienced FGM/C. It is estimated that at least 2 million girls are at risk from FGM/C every year. Type 1 and two are the most common forms of FGM/C; 80% of cases and infibulations accounted for 15% of cases [2,5]. Most women and girls with FGM/C lived in 28 sub- Saharan African countries with few figures from Asia and the Middle East. Due to the migration of people who practiced this tradition, FGM/C is today evident in Australia, Canada, the United States and the European Union [4]. The prevalence of FGM/C varied from nation to nation such as Niger (5%), Ghana (5%), Benin (17%), United Republic of Tanzania (18%), Nigeria (19%), Eritrea (89%), Sudan (90%), Egypt (97%) and Ethiopia (80%) [4,6-10]. According to Demographic and Health Survey report of Ethiopia, 74% of girls and women nationwide had subjected to FGM/C. The Regional distribution of FGM/C prevalence was: 91.6% in Afar, 85.1% in Harare, 68.5% in Amhara, 87.2% in Oromia, 65.7% in Addis Ababa, 97.3% in Somali, 67.6% in Benishangul Gumuz, 29.3% in Tigray, 27.1% in Southern and 92.3% in Dire Dawa Region [11]. The most responsible identified factors for practicing FGM/C were believes, religion, education and tradition, gender-related factors, health and Socio-economic factors [12,13].
Methods
Study period and area
The study was conducted in Kabri-bayah town of Somali region; which is located in East Ethiopia. Kabri-bayah is located at 676 km from Addis Abeba the capital city of Ethiopia and 50 km from Jigjiga capaital of the region. Based on the 2007 Census conducted by the Central Statistical Agency of Ethiopia (CSA), an estimated 188,075 people are living in this district of which 42,975 (22.8%) are women in reproductive age group. Kebiribaya district has about 29 kebeles of which 25 kebeles are rural kebeles and the remaining 4 kebeles are urban kebeles. There are an estimated 28,496 households in the district majority of the households are in the rural kebeles. The district has a mild climate and receives twice annual rain fall a year. The study was conducted from Feb to March 2017.
Study design and sampling
A community based cross-sectional quantitative study design was used. The source population was all women in reproductive age 15-49 in the selected kebele. The sample size was calculated using a single population proportion formula with the following assumption: Keberbeya district was randomly selected from the fafan district. All kebeles in keberbiyah was considered to randomly select 2 kebeles. Sample size was proportionally allotted for the selected kebeles depending up on the number of Eligible women in the randomly selected kebeles. A systematic sampling was applied to identify the required households from the selected kebeles. One eligible woman was expected from each household. One woman was randomly selected in the event where a household had two or more eligible women [14-18].
Sample size determination
The sample size was calculated using a single population proportion formula with the following assumption: Prevalence of FGM was shown to be 85% with desired precision of 4% at 95% confidence level, design effect of 2 and power of 80%. Then:
= 306 by considering 10% nonresponse rate the final sample size was calculated to be 337
When P=prevalence of FGM (85%)
CI=95%
D=margin of error (4%)
no=sample size
Data collection method and tools
Data from the study participants was collected by using structured and interview administered questionnaire which is adapted from the behavioral surveillance will be translated to a local language. The questionnaire in Somali language was retranslated to the English language by experts in both languages. Questionnaire in English language was used for data collection. Socio demographic characteristics like age, religion, ethnicity, etc. and reproductive health history such as contraceptive use, communication of sexual issues with their partner etc. are included in the questionnaire. Data was collected people having diploma and supervised by B.Sc Holder [19]. Training was given for all data collectors and supervisors for two days regarding the data collection instrument, Ethical consideration and objectives of the study by the principal investigators.
Data management and analysis
The quantitative data was checked for completeness and consistency by double entry verification. Data was entered in to computer by using EpiData Version 3.1 and analyzed by using SPSS (statistical packages for Social Sciences) version 16.0 after template formation and data clearance. First descriptive analysis was carried out to explore the sociodemographic characteristics of the respondents. Bivariate analysis was used to examine the relationship between the outcome variable and selected independent variables. Odds ratio was used to determine the association between the outcome and selected independent variables [20-22]. Finally, a multivariable logistic regression analysis was used to determine the independent predictors of the outcome variable.
Female genital mutilation
All procedures involving partial or total removal of the external female genitalia for the cultural and non-therapeutic reason.
Infibulation: Procedures involving removal of the clitoris and object.
Defibulation: Cutting of the infibulation to slightly enlarge the opening and exposing the vulva usually done at delivery, at marriage, for difficulty of delivery and sexual intercourse respectively.
Operational and term definitions
Type l FGM: Excision of the prepuce with or without excision of part or the entire clitoris.
Type II FGM: Excision of the clitoris with partial or total excision of the labia minora.
Type III: Excision of part or all of the external genitalia and stitching the vaginal opening also called infibulations.
Ethical Considerations
First Ethical clearance was obtained from Jigjiga University College of Medicine and health sciences department of public health Ethics committee and study protocol was approved. Then, a written letter was obtained from Jigjiga University Research and community service directorate Somali region health bearua was communicated through formal letter from JJU research and community service directorate [23-25]. Information about the study will give for the participants, including purpose and procedures, potential risk and benefits so that encourage provision of accurate and honest responses. Study subject was told participation is their volunteer and there was no interpretation of a single response (fully confidential). An informed consent was obtained from the study subjects and they will be told that they have a full right to refuse to response either partly or completely. But, participant was also informed that their genuine responses are vital importance for my study.
Results
Three hundred twenty women of reproductive age group participated in the survey making a response rate of 94.9%. While seventeen (5.1%) of the participants were refused to participate in the study. Nearly half 162 (39.1%) of participants were in the age group of 25-34 with mean age of the respondents to be 28.3 years (Ranges from 15-49, SD-6.16 years, median age 28). Almost majority of the respondents 301 (94.4%) of the participants are Somali followed by Amhara 8 (2.6%) and 11 (2.9%) others.
Regarding the religion of the study participants, majority of them were Muslims 304 (95.4%) whereas the remaining respondents are practicing orthodox 10 (3.1%), Protestant 4 (1.2%) and others 2 (0.6%).
More than three fourths 244 (76.8%) of the study participants were house wives, while the rest are government workers 14 (4.1%) private workers 42 (12.2%) respectively. Moreover, about 231 (71.7%) of them cannot read and write whereas 89 (27.8%) have modern education above grade 12, and of which 5 (1.6%) have college/university level education.
Regarding study participants’ marital status significant proportion of the study subjects 138 (43.1%) were married, 157 (49.2%) of them were single, 10 (3.1%) widowed and 15 (4.6%) were separated (Table 1).
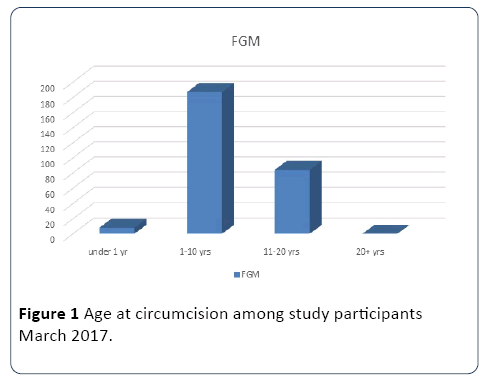
Figure 1: Age at circumcision among study participants March 2017.
Table 1 Socio-demographic characteristics of the respondents somali region Ethiopia, march 2017.
| Variables |
Frequency |
Percentage (%) |
| Age of women in years |
| 15-24 |
78 |
24.3 |
| 25-34 |
162 |
39.2 |
| 35-44 |
95 |
29.6 |
| ≥ 45 |
22 |
6.9 |
| Total |
320 |
100 |
| Age at FGC(n=279) |
| Under 1 year |
11 |
3.9 |
| 1-10 yrs |
184 |
65.9 |
| 11-20 yrs |
84 |
30.2 |
| 21+ |
0 |
0 |
| Total |
279 |
100 |
| Ethnicity |
| Somali |
301 |
94.1 |
| Oromo |
5 |
1.6 |
| Amhara |
8 |
2.5 |
| Others |
6 |
1.8 |
| Total |
320 |
100 |
| Religion |
| Musilim |
304 |
95 |
| Orthodox |
10 |
3.2 |
| Protestant |
4 |
1.2 |
| Others |
2 |
0.6 |
| Total |
320 |
100 |
| Occupational status |
| Housewife |
244 |
76.2 |
| Private worker |
42 |
13.2 |
| Gov’t |
14 |
4.3 |
| Others |
20 |
6.2 |
| Total |
320 |
100 |
| Educational Status |
| Tertiary |
12 |
3.7 |
| Secondary |
77 |
24.2 |
| Illiterate |
231 |
72.1 |
| Total |
320 |
100 |
Demographic variable
Ethnicity: The predominant ethnic group in the sample was somali followed by Amhara and Oromo and the prevalence of FGM also varies among the Ethic groups with highest prevalence among Somalis.
Age: The highest prevalence of FGM was among the older age group specifically among women older than 25 years of age.
Religion: Muslim was the predominant religion of the study participants and significant majority of the study participants undergone FGM were Muslims.
Education: In this study, 27.8% of women had at least a secondary education, and 3.7% reported some tertiary training. The highest proportion of FGC (66.6%) was found among women with the least education (primary or less schooling). In contrast, women with some tertiary education were only one-third as likely to have undergone cutting. The average monthly income of participants was found to be 697.2 Et.Birr (SD-641.1 Et.Birr, Range: 300-4500 birr). Significant number of participants, earn <1000 birr per month. Majority of the study subjects 244 (65%) are house wife followed by private workers and gov’t employee 42 (13.1%), 14(4.3%) respectively (Figure 1).
Significant proportions 184 (59.9%) of the respondents reported they have undergone FGM at 1-10 years followed by 11-20. Only few 11 (3.9%) respondents said they have circumcised before 1 years of age where as no respondent reported being circumcised after the age of 20+ years.
Prevalence of FGM
The overall prevalence of FGM was determined to be 279 (87.1%) with highest proportion of FGM to be among older age groups.
Of the total participants, nearly half of them, 186 (58.1%) were married at or before 18 years of age and 174 (54.3%) of them gave birth at or before 20 years of age. About 156 (48.5%) participants have more than three family size and the average family size of participants was 4.5 (SD-2.0, Ranges from 1-8). Moreover, significant proportion 156 (48.5%) of the participants 129 (40.1%) of participants want to have more than three children.
Knowledge of study participants about FGM
Regarding the participants’ knowledge about FGM all the study participants have heard about FGM. The main source of information about FGM for almost all 212 (66.2%) the participants were media (TV and radio) followed by health workers 81 (2.6%) specifically from HEWs. The remaining respondents said they have heard about FGM from theirs friends and neighbors.
Significant proportion of 291 (91.2%) the participants said FGM has negative health effect on women when 19 (6.1%) said FGM has no harm to women. Only 10 (3.1%) said they don’t know its benefit or effect on women (Figures 2 and 3).
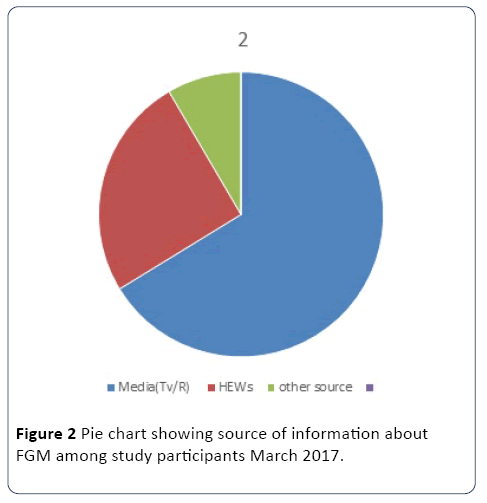
Figure 2: Pie chart showing source of information about FGM among study participants March 2017.
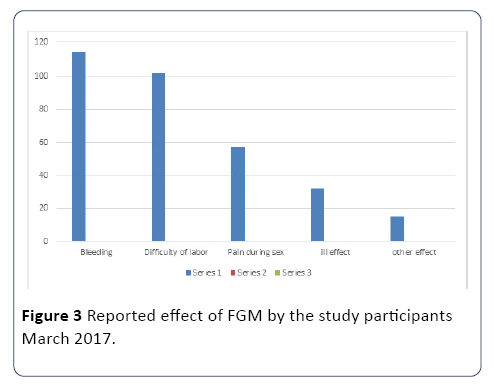
Figure 3: Reported effect of FGM by the study participants March 2017.
Majority 114 (35.6%) of the study participants reported bleeding is the main effect of the FGM followed by significant proportion 102 (31.8%) of participants reported difficult during labor as the complication of FGM. Only few 57 (17.8%) and 32 (0.1%) respondents reported pain during sex and ill effect as the complications of FGM respectively.
Common reasons why FGM was practiced
The overwhelming proportion 198 (61.8%) of study participants reported that they are practicing FGM to reserve virginity followed by 58 (18.1%) and 43 (13.4%) practicing FGM for religious and as well as to avoid sex related problems respectively (Figure 4 and Table 2).
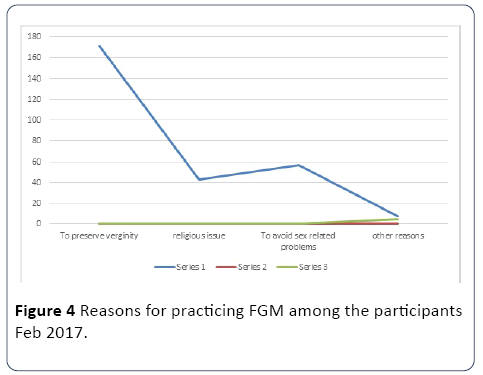
Figure 4: Reasons for practicing FGM among the participants Feb 2017.
Table 2 Association of selected sociodemographic variables with pre-marital sex among the respondents, Oromia region, Ethiopia, February 2017.
| Variables |
FGM |
COR |
AOR (95% CI) |
| |
Yes (%) |
No(%) |
|
|
| Age in yrs |
| 15-24 |
14 |
64 |
0.25 (0.05-0.78) * |
0.35(0.21-0.89) * |
| 25-34 |
148 |
12 |
2.5(0.95-6.92) |
3.70(0.98-11.51) |
| 35-44 |
95 |
0 |
2.5(1.00-4.31) |
6.34(0.99-12.32) |
| >=45 |
22 |
0 |
1 |
1 |
| Ethnicity |
| Soami |
267 |
34 |
1 |
1 |
| Ahmara |
4 |
4 |
2.41(0.33-7.88) |
3.21(0.74-12.23) |
| Oromo |
5 |
1 |
3.54(0.99-7.66) |
7.77(0.55-19.1) |
| Others |
3 |
2 |
4.23(0.33-5.95) |
5.23(0.78-8.25) |
| Religion |
| Muslims |
271 |
33 |
1 |
1 |
| Orthodox |
6 |
4 |
1.19(1.00-12.1) |
9.12(0.75-19.6) |
| Protestant |
1 |
1 |
1.22(0.77-3.45) |
2.33(1.00-5.11) |
| Others |
1 |
1 |
|
|
| Educational status |
| Illiterate |
219 |
12 |
2.47(8.99-18.11)* |
3.70(2.01-8.41)* |
| Secondary |
55 |
22 |
1.23(0.11-11.2) |
2.10(0.87-4.21) |
| Tertiary |
5 |
7 |
1 |
1 |
| Occupation |
| House wife |
229 |
15 |
1 |
1 |
| Private worker |
31 |
11 |
0.35(0.11-1.00)* |
0.78(0.51-1.00)* |
| Gov’t employee |
9 |
5 |
1.33(0.11-9.23) |
3.61(0.89-9.11) |
| Others |
10 |
10 |
2.45(1.00-5.44) |
6.12(0.78-10.1) |
FGM was associated with level of education, age of participants and their occupations. The prevalence of FGM was found to be high among old age groups. All study participants 117 (37.7%) whose age was greater than 35 years have undergone FGM. Those women whose age is below 25 years were about 35% less likely to undergone FGM compared to their counterpart (AOR: 0.35; 95% CI 0.21-0.89).
Similarly, occupation of women was negatively associated with FGM practice. Private workers had less chance of being circumcised compared to housewife. AOR: 0.78 95% CI (0.51-1.00). Of mother who undergone FGM 229 (82.1%) were illiterate. The probability of undergoing FGM is 3.7 times higher among illiterate women compared to those in tertiary education. AOR: 3.70 95% CI 2.01-8.41
Significant proportion 271 (97.2%) of the study participants reported that they undergone FGM at home while only few respondents 8 (2.8%) said they undergone FGM at a home of their relatives. No respondent undergone at health institution or by health professionals. All respondents who undergone FGM said the FGM was done by none health professionals at home. Almost all respondents said FGM was decided by mother 225 (70.3%) while few respondents 91 (28.4%) agreed that both mother and father decide whether to be circumcised or not. No participants said only Father can decide by himself about to be undergone FGM or not (Table 3).
Table 3 Attitude of reproductive age women in Kabri-bayah towards FGM March 2015, Somali region Ethiopia.
| Attitude |
Variable |
Frequency |
% |
| FGM should be stopped |
Strongly agree |
106 |
33.2 |
| Agree |
128 |
40.0 |
| Neutral |
39 |
12.1 |
| Disagree |
36 |
11.3 |
| Strongly disagree |
11 |
3.4 |
| Total |
320 |
100 |
| FGMshould be continued |
Strongly agree |
11 |
3.4 |
| Agree |
36 |
11.3 |
| Neutral |
42 |
13.1 |
| Disagree |
103 |
32.2 |
| Strongly disagree |
128 |
40 |
| Total |
320 |
100 |
| Women with FGMhave poor sexual pleasure |
Strongly agree |
71 |
22.1 |
| Agree |
147 |
45.9 |
| Neutral |
60 |
18.9 |
| Disagree |
28 |
8.7 |
| Strongly disagree |
14 |
4.4 |
| Total |
320 |
100 |
| Female students (Women) should actively participate in FGM eradication |
Strongly agree |
77 |
24.2 |
| Agree |
149 |
46.5 |
| Neutral |
54 |
16.8 |
| Disagree |
25 |
7.8 |
| Strongly disagree |
15 |
4.7 |
| Total |
320 |
100 |
| Can mass media, community and religious leaders create awareness about FGM |
Strongly agree |
78 |
24.3 |
| Agree |
156 |
48.7 |
| Neutral |
56 |
17.6 |
| Disagree |
11 |
3.5 |
| Strongly disagree |
19 |
5.9 |
| Total |
320 |
100 |
Significant majority of the respondents 106 (33.2%) strongly agreed that FGM should be stopped while nearly half of them 128 (40.0%) do agree with the idea about FGM should not be stopped.
Regarding the continuations of FGM few respondents 11 (3.4%) reported that they strongly agreed that FGM should be continued while certain proportions 36 (11.3%) of the study participants reported that they were agreed with the continuation of FGM. Only few respondents 14 (4.4%) strongly disagreed with negative impact of FGM on the sexual pleasure while significant majority of the participants 218 (68.1%) reported that FGM has a negative impact on sexual pleasure.
The role of mass media, religious leaders and community leaders were reported by significant majority of the study subjects 234 (73.1%) with regard to awareness creation about FGM while only few respondents 19 (5.9%) strongly disagreed with the role of mass media and religious leaders to create awareness about the effect of FGM.
Almost all 312 (97.1%) of the study subjects were reported that FGM highly practiced in their locality with significant proportion 275 (85.5%) of the participants revealing traditional culture favors the practice of FGM (Table 4).
Table 4 FGM practice among reproductive age group in kebeibeya, somali region Ethiopia, march 2015.
| S/n |
Variable |
Frequency |
Percentage % |
| 1 |
Is FGM practiced in your locality |
| |
Yes |
312 |
97.6 |
| |
No |
5 |
1.5 |
| |
I don’t know |
3 |
0.9 |
| |
Total |
320 |
100 |
| 2 |
Who mostly practice FGM |
| |
Rural community |
135 |
42.2 |
| |
Urban community |
62 |
19.4 |
| |
Both |
123 |
38.4 |
| |
Total |
320 |
100 |
| 3 |
Do traditional culture favors FGM |
| |
Yes |
275 |
85.9 |
| |
No |
25 |
7.8 |
| |
I don’t know |
20 |
6.3 |
| |
Total |
320 |
100 |
| 4 |
Who mostly performs FGM |
| |
Non-medical people |
320 |
100 |
| |
Health professional |
0 |
0 |
| |
Others (specify) |
0 |
0 |
| |
Total |
320 |
100 |
| 5 |
Were you circumcised |
| |
Yes |
279 |
87.1 |
| |
No |
41 |
12.9 |
| 6 |
Where were you circumcised |
| |
At home |
279 |
100 |
| |
Health institution |
0 |
0 |
| 7 |
Who decides FGM to be done in your family |
| |
Mother |
225 |
70.3 |
| |
Father |
0 |
0 |
| |
Both father and mother |
91 |
28.4 |
| |
Other |
4 |
1.3 |
| |
Total |
320 |
100 |
Regarding decision making about FGM to be carried out they are mothers who decided in majority 225 (70.3%) of the study subjects. No father gave decision alone according to a report from study participants.
All study participants reported they are non-professional people who perform FGM in the community.
Discussion
Even though FGM/C is a very deeply rooted harmful tradition practice which will result in several complicated health problems including loss of body parts within the community, it is preventable if there is a coordinated action on it at community level starting from awareness creation to punishing those who become ignorant to the program The operation, which lasts around 15-20 minutes, is carried out by traditional birth attendant and other untrained professionals living in the community with un sterile settings [11,12].
Based on the current study findings, about more than half, 62.7% of study participants were circumcised at different levels of their age. This finding was lower when compared with study findings from Sudan where its practice was over 90% and in Egypt as its practicing rate was 95.7% [10,12]. This figure was also slightly low as compared with findings of EDHS 2011 report, which was 68.5% among 15-49 aged women for Amhara Region [11]. This may be due to the variation in study area and period, variation in efforts of health extension workers and timely increase to visit health institutions for other services. The presence of high of FGM/C in regional level is an indicator of the presence of other districts or zones with higher FGM/C prevalence than the current study area.
Another study conducted by Egyptian ministry of health and population in 2003 reported 94.6% of married women had been exposed to FGM and 9.1 off those women agreed to carry out FGM on their daughters [26,27].
This difference might be because the historic and religious differences between the two country. Even if there were no documented evidences certain sources suggest FGM was primarily started in Egypt which may contribute to high prevalence of FGM in the country. The finding of the study is also low compared to the prevalence of FGM in afar region of Ethiopia which indicated 91.6% of married women undergone FGM [28].
Conversely the finding of this study was higher compared to study conducted in Tigray regional state which reported the prevalence of FGM to be 23%. Cultural and religious difference between the two regions contributed to the difference [29].
Study conducted in Egypt reported that significant proportion of people practice FGM as a social norm and majority of them 61.9% women undergone FGM in Egypt has agreed to carry out FGM for their daughters too [28].
In this study the effect of religion and ethnicity was not studied in depth except its high descriptive proportion among some religions compared to others which might be because of chance.
In addition to this there are no uniform distributions of Muslims and Christians in the country. In some part of the country there might be high prevalence of FGM among Christians or among Muslims in other districts. This is a big indication for further detail investigation.
The likelihood of girls and women to undergone FGM was related with socioeconomic factors. In this study illiterate women are high likely to undergone FGM compared to their counterpart. This finding is in line with study conducted in Bale zone reporting high proportion of FGM was done among illiterate women and those with low income. In Ethiopia majority of the people are living in the rural setting where there is no access to education and other health care services [28,30].
In consultation with local community association the ministry of health in Ethiopia has the strategy to stop FGM. In this study, significant proportion of the study participants agreed to stop FGM. Some participants recommend the continuation of FGM.
This finding is in line with study conducted in Egypt reporting 61.9% of women who undergone FGM has a plan to carry out for their daughters [28].
Even if FGM has been considered as a source of income for the practitioners it has negative health effect among the victims. Only few participants reported the complications and health impacts of FGM. This finding is in line with study conducted in somali reginal state showing few health effects of FGM [31].
In our study, almost all study participants undergone type I FGM with only few study participants reported they underwent type II.
Conclusion
The study showed that the prevalence of FGM remains high despites of several efforts made by local authority to stop a practice. Age, educational status and occupation were found to be associated with FGM.
Competing Interests
The authors declare that they have no competing of interests.
Authors’ Contributions
BA is a principal investigator who involved in conceived the original idea, proposal writing, designed the study, got funding for the study, data collection, drafting of the manuscript and participated in all implementation stages of the study and drafted and finalized the write up of the manuscript. LM, MD and AT involved in, proposal writing, reviewing, data collection and participated in all stages of the study implantation. Both authors read and approved the final manuscript.
Acknowledgements
We would like to acknowledge Jigjiga University, for giving us this chance to undertake this research. We would also like to thank Somali regional health bureau for providing us necessary back ground information during this proposal preparation. Last but not least our appreciation goes to study participants for their time and genuine information.
20129
References
- Leye E, Powell RA, Nienhuis G, Claeys P, Temmerman M (2006) Health care in Europe for women with genital mutilation. Health Care Women Int 27: 362-378.
- Sakeah E, Beke A, Doctor HV, Hodgson AV (2006) Males’ preference for circumcised women in Northern Ghana. Afr J Reprod Health 10: 37-47.
- Oduro AR, Koram KA (2006) Trends in the prevalence of female genital mutilation and its effect on delivery outcomes in the Kassena-Nankana District of Northern Ghana. Ghana MedJ 40: 87-92.
- Wise Muslim Women’s Shura Council (2010) Female genital cutting: Harmful and un-Islamic.
- Monjok E, Essien EJ, Holmes L (2007) Female genital mutilation: Potential for HIV transmission in sub-Saharan Africa and prospect for epidemiologic investigation and intervention. Afr J Reprod Health 11: 33-42.
- Nour NM (2008) Female genital cutting: A persisting practice. Rev ObstetGynecol 1: 135-139.
- Population reference bureau (2010) Female genital mutilation/cutting. Data and trends update.
- Kaplan-Marcusán A, Rio N, Navarro M, Castany-Fàbregas MJ, Nogueras MR, et al. (2010) Female genital mutilation: Perceptions of healthcare professionals and the perspective of the migrant families. BMC Public Health 10: 193.
- Kolawole, Kwaak A (2010) Review of determinants of female genital mutilation in Nigeria. J Med Medical Sci 1: 510-515.
- Emam EA, EL-Maghawri AM, Labeeb SA (2011) Cultural awareness about female genital mutilation among female employees of Minia University. J Am Sci 7: 611-617.
- No authors listed (2006) Ethiopiademographic and health survey, 2005. J Health FMOH CSA, Ethiopia.
- Ethiopian Public Health Association (EPHA) (2009) Extract No.6,7andResearch methodology and ethics training proceedings manual.
- Haile D, Fuseaha HM, Tilahun T (2004) Women’s affairs office in collaboration with national community on HTP. Ethiopian women lowers association andUNICEF.
- BergR,DenisonE,Fretheim A (2010) Factorspromotingandhinderingthepracticeof female genitalmutilation/cutting(FGM/C).
- UNFPA (2013) Globalconsultationonfemalegenitalmutilation/cutting,technicalreport, 2009.
- Population Reference Bureau(PRB) (2010)Female genital mutilation/cutting.Dataand Trends, Washington.
- Tag-Eldin MA, Gadallah MA, Al-Tayeb MN (2008) Prevalence of female genital cutting among Egyptian girls. Bulletin of the World Health Organization 86: 269-274.
- Kandil M (2012) Female circumcision: Limiting the harm. F1000 Research.
- Mitike G, Deressa W (2009) Prevalence and associated factors of female genital mutilation among Somali refugees in eastern Ethiopia: A cross-sectional study. BMC Public Health 9: 264.
- Yirga WS, Kassa NA, Gebremichael MW, Aro AR (2012) Female genital mutilation: Prevalence, perceptions and effect on women’s health in Kersa district of Ethiopia. Int J Womens Health 4: 45-54.
- Abdulcadira J, Margairazb C, Boulvaina M, Iriona O (2011) Care of women with female genital mutilation/cutting. Swiss Med Wkly 140: 131-137.
- Karmaker B, Kandala NB, Chung D, Clarke A (2011) Factors associated with female genital mutilation in burkinafaso and its policy implications. Int J Equity Health 10:20.
- Mariam GA, Hailemariam A, Belachew T, Michael K, Lindstrom D (2009) Support for the continuation of female genital mutilation among adolescents in Jimma Zone, Southwest Ethiopia. Ethiop J Health Sci 19: 119-129.
- Bjälkander O, Bangura L, Leigh B, Berggren V, Bergström S, et al. (2012) Health complications of female genital mutilation in Sierra Leone. Int JWomen’s Health 4: 321-331.
- Kizilhan JI (2011) Impact of psychological disorders after female genital mutilation among Kurdish girls in Northern Iraq. EurJ Psychiat 25: 92-100.
- Egyptian fertility care society, population council (1996) Asia and East operation research and technical assistance final report. Egypt population council, Cairo.
- Elithabeth H (1994) Social, cultural and ethnic factor determining the practice of F.G.M in Ethiopia.
- Daniel B, DesaalegnM, Mahammedawal K (2014) Prevalence of female genital cutting and its effect on human health in bale zone. BMC Public Health14:1076.
- Barrak BF (1995) Study of accustom in Somalia: Female circumcision, medicine tropical.

