Keywords
burnout, nursing personnel, regional hospital, work environment.
Introduction
Freudenberger first used the term burnout in 1974 saying that it is the feeling of the failure and exhaustion that can be observed in social workers that worked in institutions and it was the result of immoderate requirements of energy, effort and qualifications (Freudenberger, 1974). Burnout is long-term reaction to occupational stress and appears mostly to those practicing social vocation (Gabassi et al, 2002). The aetiology of burnout syndrome is multidimensional, as research has proved the impact of psychological, social educational and financial factors in its configuration. Professionals that have frequent contact with individuals are more sensitive to develop burnout (Cordes & Doherty,1993; Vegchel et al, 2004). As their emotional resources are depleted, workers feel they are no longer able to give of themselves at a psychological level (Maslach & Jackson, 1981).
Burnout as a syndrome has three dimensions (Maslach & Jackson, 1984; Anagnostopoulos & Papadatou, 1992):
α) emotional exhaustion
β) depersonalization
γ) lack of personal accomplishment
Emotional exhaustion refers to workers disability to offer emotionally to the recipients of their services. Emotional exhaustion results from decrease or loss of self-confidence and interest in one's profession as well as feelings of fatigue and weakness (Demir et al, 2003). A common symptom for the individual is to see with awe the prospect that the next day will have to go to his work again.
Depersonalization refers to the negative and cynical confrontation of recipients of their services. A typical example of such behavior is the inclination to refer to patients not with their names but with the number of their bed /room, or the disease.
The growth of this impersonal behaviour towards patients, their co-workers, and the organization makes the worker feel inadequate, ineffective, makes him underestimate his efforts and in the end makes him fail to achieve his goals in the professional field. It is the point where feelings of low personal accomplishments start to appear, especially when work doesn’t ensure positive feedback and remuneration (Maslach & Jackson, 1986).
Causes of professional burnout are many and factors that contribute in its appearance contain:
Work load (Bakker et al, 2003), high expectations of patients and their families, excessive responsibility in work environment, working with unqualified and few personnel (Demir et al, 2003).
• Trauma incidents at work such as bad prognosis of patients that they are responsible for (Van der Ploeg et al, 2003). Lack of satisfaction, lack of motives, role conflict (Posig & Kickul, 2003).
• Lack of support by co-workers, by managers (Brown & O’Brien, 1998, Westman & Etzion, 1999).
• Shift changes and long work hours (Demir et al, 2003).
The social-demographic factors that lead in increased sensitivity in the appearance of burnout according to research concern new individuals (Gabbe et al, 2002; Chopra et al, 2004) with high educational level, with small previous experience, not married , and working many hours the week (Adali, 1999).
Socio-demographic factors such as age, job experience, marital status, having children, educational level or income, and job-related factors such as excessive work load, absence of job resources, lack of autonomy have been found related to burnout (Maslach et al, 2001). Employees are vulnerable if they have little say about how to do a job, every specific of work execution being dictated or laid-out in lengthy job descriptions. When people are saying that they are burning out, they are indicating that work has lost its meaning for them, that they feel disillusioned (Felton JS, 1998).
Burnout relates with psychosomatic symptoms such as sleep disorders, diet disorders, headaches, ulcer, loss of libido, but also with emotional symptoms such as hypersensitivity, cynicism, phobias, depression, apathy, or intellectual symptoms as weakness of concentration that leads the individual to negative forms behavior (increased alcohol consumption and nicotine), disturbance in his personal relations but also in reduction of his productivity, his efficiency and in negative attitude towards work (Fredeunberger, 1974; Maslach and Jackson, 1981; Maslach, 1981; Demerouti, 2001). Perhaps the most visible impact of burnout is the change in people's work performance (Felton JS, 1998).
This negative attitude towards work results to bad labour relations, absenteeism, errors at work, low level of healthcare quality (Maslach et al, 2001). In England, 40 million work days are lost every year due to disorders caused by stress. It was stressed that 30 million dollars have been spent in Australia due to job stress. In US as well, overall 550 million work days are lost due to problems related to stress (Hoel et al 2001).
Aim of the study
The present study aims to determine the burnout levels of nurses employed in a major Regional University hospital and the correlation of factors of burnout level with demographic and professional factors.
Methods
The present study was descriptive with synchronical comparisons and cross-correlations.
Tools of measurement
Two forms were used for data collection in this research. A general information questionnaire, recorded the demographic (age, education, marital status) and professional features (professional status, weekly work hours, participation in professional activities) of the sample of the study. It was formulated by the investigators according to similar questionnaires found in Greek and international literature. The questionnaires were anonymous.
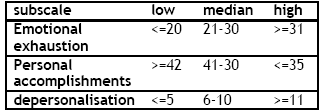
The second form used in this research is Maslach Burnout Inventory (MBI), developed originally by Maslach (1981). It is translated into Greek and its reliability was recalculated by Anagnostopoulos and Papadatou 1992. Maslach Burnout Inventory (Maslach et Jackson 1986) evaluates experienced burnout and has three subscales. Emotional Exhaustion (EE) subscale which includes nine articles. EE describes the feelings in the individual of being exhausted by his/her job. Depersonalization (DP) subscale includes five articles. This subscale defines the behaviour that hurts self-esteem and is without emotion, towards the individuals whom she gives care. Personal Accomplishments (PA) subscale has eight articles. This subscale defines the feelings of being able to cope with the problems an individual working directly with people is confronted with in the work environment (Maslach and Jackson, 1981). High scores in EE and DP subscales and low scores in PA subscale indicate high levels of burnout. Moderate burnout corresponds to moderate scores in each subscale. Low scores in EE and DP subscales and high scores in PA subscale indicate that burnout is at a low level (Maslach and Jackson, 1981).
The MBI has 22 statements regarding different burnout dimensions, and each item has seven choices ranging from “never” (=0 point) to “every day” (=6 points). Participants rated the frequency of experiencing feelings related to each subscale using a 7-point scale with the verbal anchors: Never, A few times a year or less, Once a month or less, A few times a month, Once a week, A few times a week, and Every day, centred under the numerals 0 through 6. (Maslach & Jackson, 1996).
Scores of subscales of burnout
The criteria for choosing the particular tool were that it is reliable, valid, while it has been used in a lot of countries and in various labour spaces (Maslach & Jackson, 1996). The evaluation of Greek publication showed that “it is a short, structural valid and internally reliable body of recording of emotions of individual toward his work and his attitude toward those who they provide services, at least nursing” (Anagnostopoulos & Papadatou, 1992).
Statistical analysis
The data analysis was realised with statistical methods of descriptive and inductive statistics. The level of statistical importance was fixed equal or smaller of 0,05. The statistical parcel of SPSS for Windows (version 15) was used. In the statistical analysis, the relation between all variables in part I and burnout scores were evaluated. One Way Variance Analysis (ANOVA) (F-test), Tukey Test, chi-square (χ2), Significance of the Difference Between Two Means Test (t-test), Kruskall Wallis were used in statistical analysis. In analysing the data, three statistical tests were employed: t-test to compare the means in two groups, and ANOVA to compare the means in multiple groups. ANOVA was preferred in order to make use of the post hoc techniques (Tukey, Scheffe) to determine the real differences between categories of the independent variable.
Ethics
Approval to conduct the study was obtained from the Boards of Directors and the Nursing service Administration of the Hospital. The nurses were not able to complete the questionnaires on the same day because of work pressure. The agreement to complete the questionnaire was considered as consent to the participation in the study. Information was given orally on the inquiring team, the aim of study, the maintenance of anonymity and confidentiality of data, the voluntary attendance and the possibility of interruption any moment.
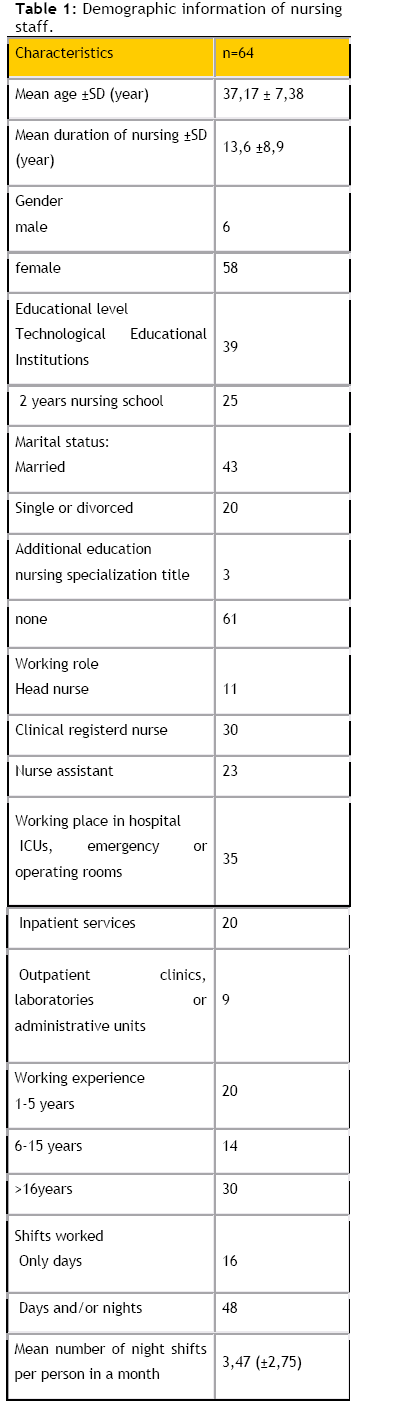
Results
The questionnaire was distributed in 150 registered nurses and nurses assistants in Regional University Hospital at the duration of one month (November 2006) and were returned 64 answered (response rate 42,6%). In table 1 is shown all the demographic information of nursing staff. 95,31% of the sample were women (Ν=58) .36% of the sample were nurses assistants, 55% were clinical nurses, and 9% were head nurses. Most nurses were married with 1-2 children and they had a work experience of up to13,6 years (1year minimum-30 years maximum) (SD 8,9 years). The majority of nurses (60,9%) were graduates of Technological Educational Institutions and 39,1% had 2 years of education in Nursing. None of the registered nurses possessed Masters Degree or Ph.D. and only 4,7% has a nursing specialization title. 15,6% of the sample worked in ICU, the double percentage in clinics with up to 40 bed capacity, while the 20,3% worked in surgery and the 18,7% in ER, and the 14% in outpatient department. Concerning the work environment, 25% of the nurses in our sample were working only one shift (day shift) and 75% were working in a rotation shift. Only 2% had 4 night shifts a month, 31% up to 8 night shifts a month and 67% in our sample made more than 8, while the mean number of night shifts were 3,47 (SD 2,75). Nurses assistants were working mean 2,28 days in the weekend while registered nurses 2,82 days in the weekend. 43,8% of our sample had never changed working environment while 57,2% had changed working environment up to 5 times. The percentage of nurses that reported that their place in the particular department that worked constituted their personal choice was the 39,1%, while 60,9% it claimed that other decided for them. Only the 15,6% of sample answered that wants their child to follow the same profession and the 60,9% from them it would not choose again the same profession. 21,88% of the sample want to abandon the profession at an early date while the 34,38% in certain years. The 85,9 of the sample attributes the hindrance of achievement of interdisciplinary collaboration in the doctor – centred model of hospitals.
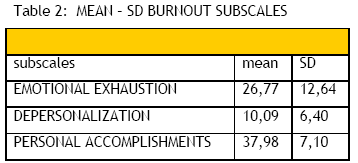
In the present study it was found that the 9,37% of sample experience high level of burnout and 6,24% of the sample low level. Low emotional exhaustion appear to have 34,4% of the sample, and high 45,3% of the sample. Low depersonalization has 26,6 of the sample and high 40,6% of it. While low personal accomplishments are not presented in the sample, and high PA are present in 71,9% of the sample (table 2).
The factors of burnout were examined in combination with the qualitative characteristics, as sex, the marital status, the level of education, with χ2 (table 3) and in combination with the quantitative demographic characteristics as the age, the weight, the height, the number of children, with ANOVA one way and it did not find to relate themselves considerably. What found to relate itself considerably is the sense of personal accomplishments with the existence of children (p=0,01). Explanation constitutes that the existence of children ensures positive feedback for the individual.
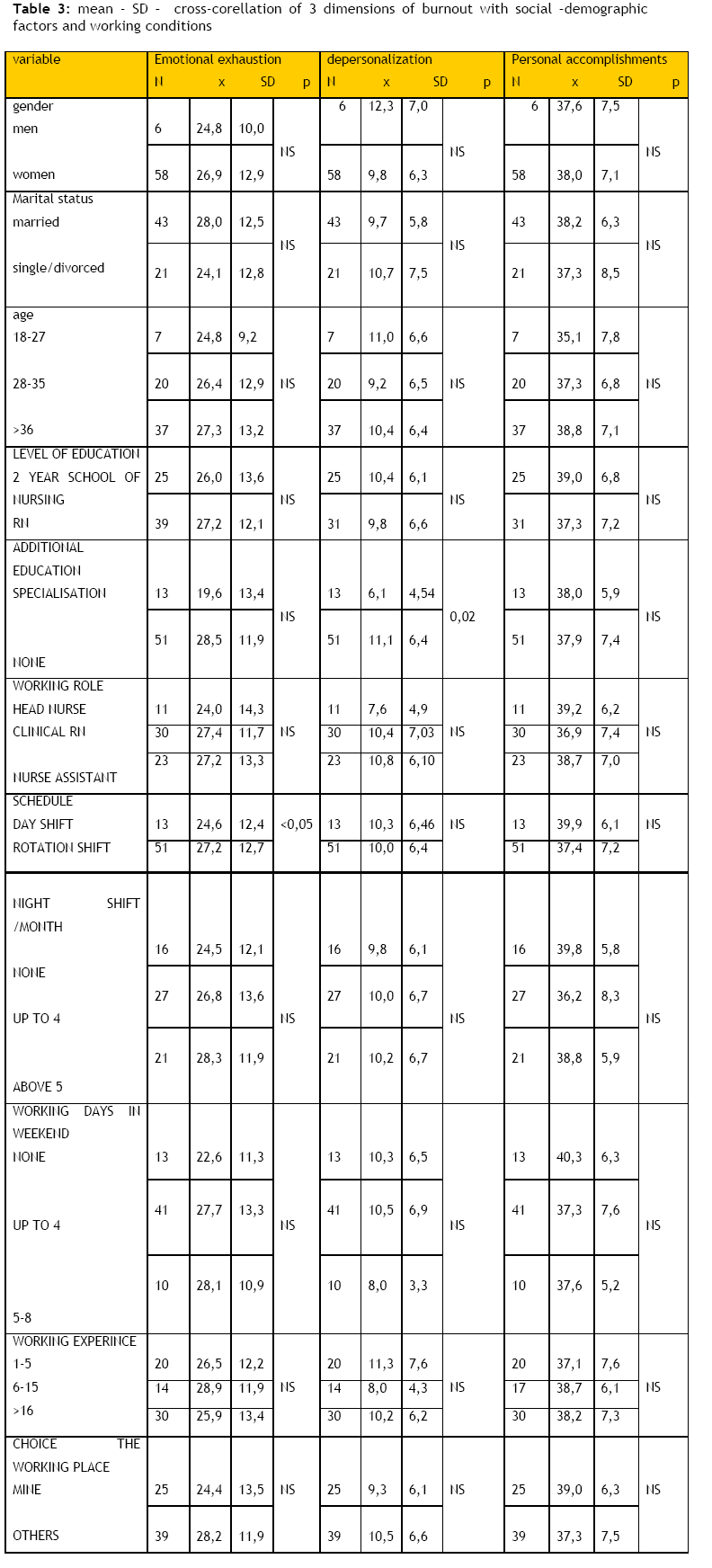
Cross-correlation of burnout with professional factors
Qualitative and quantitative professional and other characteristics as independent variables such as years of previous experience, the type of schedule (shift, morning), the days of work at the weekend, the place of work, the additional education were correlated with 3 burnout dimensions. Performing chi-square test, additional education was found to correlate significantly with depersonalization (p=0,02) (table 3). Explanation constitutes that the growth of impersonal behaviour toward patients, collaborators and organisation is related considerably with the feeling of insufficiency, inefficiency, depreciation of oneself and failure of achievement of objectives in the professional sector. The 3 burnout dimensions were correlated with quantitative professional characteristics as the years of previous experience, the days of work in the weekend, the night services, with ANOVA one way test and it did not find to relate considerably.
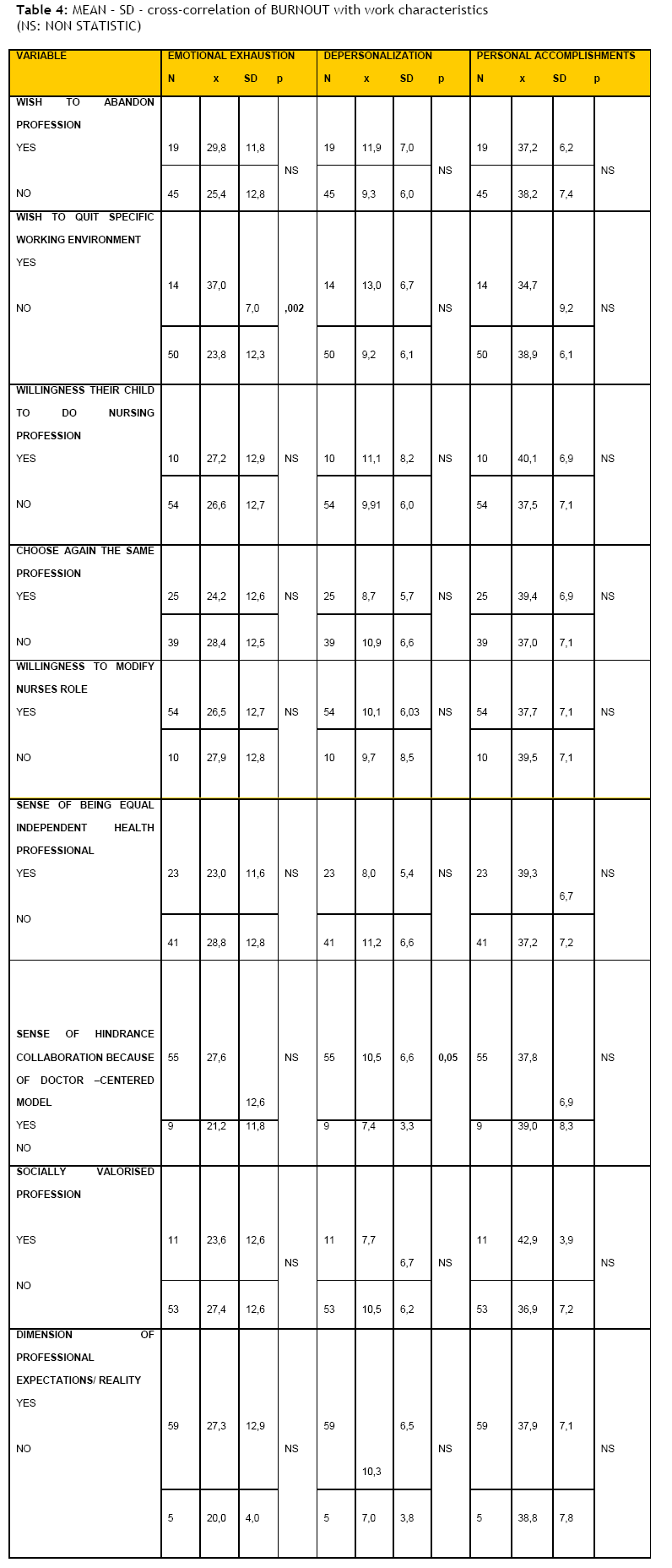
Performing chi-square test emotional exhaustion was found to correlate significantly with working in shifts (p<0,05). Emotional exhaustion also influences the willingness of retirement from the particular hospital (p=0,002). Depersonalization correlates significantly with hindrance of interdisciplinary collaboration because of the model of hospital that is centred to doctors. (p=0,05) (table 4).
Discussion
In the present study it was found that burnout of nursing personnel was oscillated in mediocre levels. This discovery is also strengthened by previous researches that were made in General Greek hospitals. (Adali et al, 2002; Asimakopoulou, 2004; Kandri et al, 2004). When comparing the total scores and the personal and workplace features of the questionnaire, we came to the conclusion that the sociodemographic data are not significant for the formation of burnout something that was also found in Palfi et al, (2008) research. As it was expected, taking into consideration the results of other researches the emotional exhaustion influences the willingness of nurses to retire. Severe burnout gives rise to problems such as quitting one's job, job dissatisfaction. (Beemsterboer and Baum, 1984; Fredeunberger, 1974; Maslach and Jackson, 1981; Maslach, 1981.
Individuals experiencing emotional exhaustion want to abandon their working facility. Depersonalization correlates significantly with hindrance of interdisciplinary collaboration, something that shows that indifference and impersonal confrontation of patients is related considerably with the hindrance of interdisciplinary collaboration. (Ouzouni, 2005).
The decreased sense of personal accomplishments leads to feelings of decreased social award of nursing profession. Important element constitutes also that the nurses feel that exists dimension of their professional expectations with the reality in percentage 92,2%. It is important to be pointed out that the nurse feels that makes a socially valorised profession as long as she/he feels that constitutes an equivalent member of sanitary team and a simultaneously and independent health professional. Stewart and Arklie, 1994 found out that nurses whose roles are not clearly defined and do jobs which are not their duty have higher levels of burnout. It is known that Greek Hospital are doctor-centered something that increases the hindrance of interdisciplinary collaboration. A big percentage of sample (84,4%) wishes the modification of their role in the professional health team, while the 89,9% of RN would want the modification of their with actions that he/she will be responsible for as an independent health professional, while only 35,9% of the sample feels professionally equal with other health professionals. Shift-working, including working nights, and increases in the length of time worked during the day, have been shown to be burnout factors both in this study and previous studies. (Shimizu et al, 2005). Younger nurses reported higher levels of burnout than nurses over 30 or 40 years old. Brewer and Shapard’s (2004) meta-analysis about the effects of age and experience on burnout provides support for this outcome.
The results suggest that improvement in this field should be a priority intervention, that is, specific interventions should be planned to help prevent job burnout, low levels of job satisfaction and subsequent turnover. ( Piko BF, 2006)
Individual and organisational Burnout Management
The early recognition of burnout syndrome as a result of extended stress and disappointment will contribute to the growth of professionalism, to the change of organisational structures in the working environment and finally to healthcare quality in the provided services. It has been found that the least exhausted individual has confidence in his faculties and is able to handle the problems that emerge (Elliot et al, 1996). Active effort of resolution of problems was found to relate with low levels of burnout. (Maslach, 1982; Armstrong-Stassen, 2004). Certain techniques of confrontation of the problem are the maintenance of balanced life, the attendance in teams of psychological support in order to share the emotions and the experiences. (Anagnostopoulos & Staurou, 2005).
The individual should place realistic objectives, learn to manage stress, to understand his limits. The learning of techniques of relaxation and management of time, the programs of physical exercise, as well as the techniques of consolidation of social contacts and support have been proposed extensively in the world bibliography for dealing with burnout.
The problem however does not only influence the individual but also entire the organisation and should be evaluated proportionally from the administration in order appropriate measures are taken. The organisations should educate their personnel to handle the crises and should also undertake initiatives for the minimisation of professional stress. More specifically it is proposed: (Kostandinidis et al, 2006):
a) The placement of suitable professional in the suitable place increases his probabilities of output but also benefit of qualitative care
b) The clarification of professionals’ role and duties and their inclusion in the decision-making.
c) The possibility of breaks and special authorisations given by administration
d) The increase of possibilities for professional development.
e) The operation of teams for psychological support
f) The given possibility of continuing training and education
g) The interdisciplinary collaboration between the members of healthcare team (doctors, nurses, psychologists, psychiatrists, social workers) which presupposes the recognition of role, duties, but also limits of each expert and his contribution in the comprehension of approach and handling of each case.
The methods of prevention and confrontation of burnout concern the better planning of hospital spaces and other spaces of health, the enrichment of work, the inclusion of nurses in decision-making, the clarification of roles and duties of doctors and nurses, the opportunity given for continuing training and education, as well as the organisation of advisory teams for workers that face problems.
Conclusion
In conclusion level of burnout in the nursing personnel of a Regional University Hospital oscillated in mediocre levels. It presents emotional exhaustion, which is related with the shifts, depersonalization which is related with the hindrance of interdisciplinary collaboration and finally both of them influence the decision to abandon the specific working environment. Finally, the decreased sense of personal accomplishments leads to feelings of decreased social award of the nursing profession.
3660
References
- Adali Ε. (1999). Comparative study of burnout of nurses in pathological departments, ICU and Emergency. Doctoral thesis National Kapodistrian University of Athens Nursing department, Athens.
- Adali Ε, Priami Μ, Euaggelou Ε, Ifanti Μ, Mougia Β. (2002). Burnout and working environment of psychiatric nursing personnel. Nosileftiki: 41:105-114.
- Armstrong-Stassen M. (2004). The influence of prior commitment on the reactions of layoff survivors to organizational downsizing. Journal of Occupational Health Psychology: 9(1): 46-60.
- Asimakopoulou Μ. (2004). Burnout, professional satisfaction and the engagement in work in Social Sector. Final work University of Patras Department of Administration of Enterprises, Patras.
- Anagnostopoulos F, Papadatou D. (1992). Productive synthesis and internal cohesion of questionnaire of recording burnout in sample of nurses. Psychological Subjects: 5(3):183-202.
- Anagnostopoulos F, Staurou S. (2005). Burnout of EKAB personnel and satisfaction of patients. Επιθεώρηση Υγείας:97(16):11-26.
- Bakker A, Demerouti E, Taris T, Schaufeli W, Schreurs P. (2003). A multigroup analysis of the job demands-resources model in four home care organizations. International Journal of Stress Management: 10(1):16-38.
- Brewer EW, Shapard L. (2004). Employee burnout: a metaanalysis of the relationship between age or years of experience. Human Resource Development Review: 3:102–123.
- Brown C, O’Brien K. (1998). Understanding stress and burnout in shelter workers. Professional Psychology: Research & Practice: 29(4):383-385.
- Chopra S, Sotile M, Sotile W. (2004) Physician Burnout. JAMA: 291(5):633.
- Cordes C, Dougherty T. (1993). A review and integration of research on job burnout. Academy of Management Review: 18:621-656.
- Demerouti Ε. (2001) Burnout: definition and its relation with the labour conditions in various professional sectors. In: Basilaki E, Triliba S, Bezevegis E. Stress, anxiety and their confrontation, Athens: Ellinika Grammata.
- Demir A, Ulusoy M, Ulusoy M.F. (2003). Investigation of factors influencing burnout levels in the professional and private lives of nurses. International Journal of Nursing Studies: 40(8): 807-827.
- Elliot T, Shewchuk R, Hagglund K, Rybarczyk B. (1996). Occupational burnout tolerance for stress, and coping among nurses in rehabilitation units. Rehabilitation Psychology: 41(4):267-284.
- Felton J.S. (1998). Burnout as a clinical entity —its importance in health care workers. Occup Med: 48(4):237-250.
- Freudenberger H J. (1974). Staff burnout. Journal of Social Issues:30(1):159-165.
- Gabassi PG, Cervai S, Rozbowsky P, Semeraro A, Gregori D. (2002). Burnout syndrome in the helping professions. Psychol Rep: 90(1):309-14.
- Gabbe SG, Melville J, Mandel L, Walker E. (2002). Burnout in chairs of obstetrics and gynecology. Am J Obstet Gynecol: 186:601-612.
- Hoel H, Sparks K, Cooper CL. (2001). The cost of violence/ stress at work and the benefits of a violence/stress-free working environment. Report Commissioned by the International Labour Organization (ILO) Geneva, (online) Available from: https://www.ilo.org/public/english/protection/safework/whpwb/econo/costs.pdf (reached: 05.11.2007).
- Kandri T, Kalemi G, Moschos N. (2004). Phenomenon of «burnout syndrome» in doctor and nursing personnel in Trauma Unit in General Hospital of Nikaia. Nosileftiki: 1:116-125.
- Korompeli A. (2004). Why ICUs are stressful. Abstracts of 2nd Scientific Conference Urgent and Intensive Nursing, Volos.
- Konstandinidis T.K, Moustaka H, Malliarou M. Professional Stress, burnout syndrome in hygiene and safety of work. Publication of Program of Postgraduate Study Hygiene and Safety of Work, Alexandroupoli, 2006.
- Maslach C, Jackson SE. (1981) The measurement of experienced burnout. J Occup Behav: 2:99-113.
- Maslach C. (1982). Burnout. The cost of caring. New Jersey: Prentice- Hall Inc.
- Maslach C, Jackson SE. (1984). Burnout in organizational settings. Applied Social Psychology Annual: 5:133-153.
- Maslach C, Jackson SE. (1986). Maslach Burnout Inventory manual 2nd ed. Palo Alto California: Consulting Psychologists Press.
- Maslach C, Jackson SE, Leiter PM. (1996). Maslach Burnout Inventory manual 3rd ed. Palo Alto, California: Consulting Psychologists Press.
- Maslach C, Schaufeli WB, Leiter MP. (2001). Job Burnout. Annual Review of Psychology: 52:397-422.
- Οuzouni C. (2005). Exploratory study of factors that cause stress in the nursing personnel of psychiatric units of short hospitalisation. Νosikeftiki: 44(3):355-363.
- Palfi I, Nemeth K, Kerekes Z, Kallai J, Betlehem J. ( 2008). The role of burnout among Hungarian nurses. International Journal of Nursing Practice: 14: 19–25.
- Piko BF. (2006). Burnout, role conflict, job satisfaction and psychosocial health among Hungarian health care staff: A questionnaire survey. International Journal of Nursing Studies: 43: 311–318.
- Posig M, Kickul J. (2003). Extending our understanding of human burnout: Test of an integrated model in no service occupations. Journal of Occupational Health Psychology: 8(1): 3-19.
- Shimizu T, Feng Q, Nagata S. (2005) Relationship between turnover and burnout among Japanese hospital nurses. Journal of Occupational Health: 47: 334–336.
- Stewart MJ, Arklie M. (1994) Work satisfaction, stressors and support experienced by community health nurses. Canadian Journal of Public Health: 85 (3):180–184.
- Van der Ploeg E, Dorresteijn S, Kleber R. (2003). Critical incidents and chronic stressors at work: Their impact on forensic doctors. Journal of Occupational Health Psychology: 8(2):157-166.
- Vegchel N, Jonge J, Soderfeldt M, Dormann C, Schaufeli W. (2004). Quantitative versus emotional demands among Swedish human service employees: Moderating effects of job control and social support. International Journal of Stress Management: 11(1):21-40.
- Westman M, Etzion D. (1999). The crossover of strain from school principals to teachers and vice versa. Journal of Occupational Health Psychology: 4(3):269-278.

