Keywords
Caregiver; Child; Asthma; Parents
Introduction
The concept of “caregiving” is the process of taking the responsibility of caregiving activities and their outcomes [1]. The term “caregiving” has been analyzed by several discipline such as nursing, sociology, psychology from different perspectives [2]. In nursing literature, Swanson et al. [3] are the pioneers conducting a concept analysis on family caregiving. In their analysis, caregiving process has been considered to have four distinctive features; tasks, transition, roles and process. Tasks include daily routines, quantity of care and direct/indirect caring. Transition on the other hand focuses on the management of caring process and its transition from family to the institution. Roles cover caring of the family and mutual supporting behaviours.
The concept of “caregiver burden” is rather complicated and multidimensional. Zarit et al. [4] defined caregiver burden as ‘the degree to which a carer’s emotional or physical health, social life or financial status had suffered as a result of caring for their relative. Dang et al. [5] emphasises that caregiver burden involves physical, social and financial conditions of caregivers. Caregivers provide not only direct caring but psycho-social support also related with the disease. Delivering care to the child with a chronic disease requires an additional role so that some priorities need to be redesign and energy should be redirected [6]. The caregiver providing primary care often overwhelmed with negative effects of caregiving burden if she is unprepared for continuous caring [7,8]. In this review caregiver burden refers to high level of physical, psychological, emotional, behavioral and financial burden experienced by parents who are caring for children with asthma.
Parenting to a child with chronic disease is a struggle. At the present time, health care shifts to outpatient and public based services due to the developments in the field of medicine thus parents need to participate in the caring process more actively [9,10]. Furthermore, family unit’s getting smaller and increasing divorce rates enhance the caregiving responsibilities of parents. Due to increasing responsibilities of parents many studies have focused on identifying of parents’ needs, understanding of their overcoming and problem-solving abilities. The aim of this review is to analyze the effects caregiver burden of parents who have a child with asthma.
Methods
Search strategy
The electronic databases PubMed, Cumulative Index to Nursing an Allied Health Literature (CINAHL), Cochrane Library, PsycINFO, Ovid and the Web of Science databases were searched to access relevant articles. Searching was realized by two separate reviewers in January, 2016 and the articles published between 2000-2015 were selected. Additionally, the reference lists of each articles were scanned since it might have been missed in database searches. The search terms in databases were “caregiver”, “caregiving”, “burden”, “pediatric asthma”, “parent”. The combination 5 key words were used as searching strategy. In databases all the articles meeting inclusion criteria were carefully examined, based on their abstract and title.
Quality assessment of the studies were performed by using “Joanna Briggs Institute Critical Appraisal Checklists” [11]. This checklist includes 11 items. The sample question for the assessment of descriptive studies from checklist; ‘Were the criteria for appraising studies appropriate?’ Responses included; ‘yes’, ‘no’, ‘unclear’ or ‘not applicable’. The options at the last section of the checklist, ‘include’, ‘exclude’ and ‘seek further info’ demonstrated the final decision of the reviewer. When one of the reviewers choose ‘seek further info’ option we discussed to determine whether the article would be included.
Inclusion and exclusion criteria
The studies must have met following inclusion criteria: (1) were published between 2000 and 2015, (2) were published in English, (3) participants must be parents–mother, father or both (parents who have a child with asthma) (4) subject of the studies must be pediatric asthma (5) descriptive, prospective or retrospective observational, experimental or quasiexperimental studies (6) must allow online access to the fulltext of the article.
Following exclusion criteria has been adopted: (1) review of literature or case reports, (2) the child’s having another health problem besides asthma (3) studies developing or testing scales.
Search results
When we entered the keywords into databases, 42 studies were found and their titles were reviewed. The selection of articles were realized in two phases. In the first phase two separate authors reviewed the abstract of articles and authors selected 31 articles meeting abstract based inclusion criteria for a detailed review. In the second phase two authors read the full-texts of selected articles and those articles that did not meet the inclusion criteria were excluded. As a result; 22 articles meeting the required criteria were obtained. Then, two separate authors read the full-texts of selected articles. No conflict appeared between authors in both phases (Figure 1).
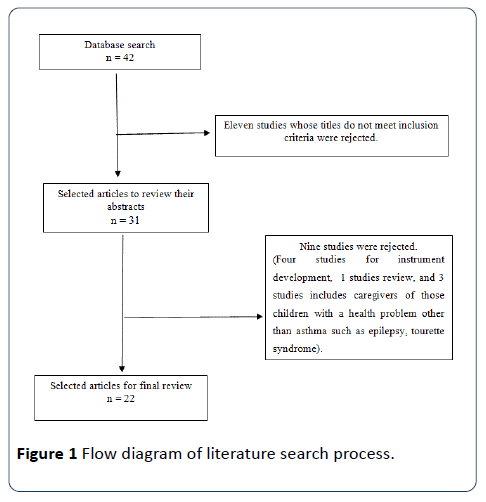
Figure 1: Flow diagram of literature search process.
Results
Initially, 42 studies that met the searching strategies stated above were found on databases. Twenty two of them remained following the analysis of their abstracts according to inclusion criteria. All the articles were published in English and 18 of the studies were descriptive design (Table 1).
Table 1 Summary of literature results.
| Author(s) |
Purpose |
Sample size |
Data collection methods |
Design |
Children age |
Instrument |
Outcomes |
| Bellin et al. [18] |
To test the longitudinal effects of risk and preventive factors on caregiver’s quality of life. |
300 |
Self report |
Randomized controlled |
03-10 |
Perceived Stress Scale |
Lower quality of life is related with higher life-stress.Poorer asthma and emergency services are the significant determinants for caregiver’s lower quality of life. |
| Pediatric Asthma Caregiver’s Quality of Life Questionnaire |
| Cerdan et al. [15] |
To test the effect of children's asthma severity and sociodemographic factors on parental quality of life. |
101 |
Self-report |
Descriptive Correlational |
7-17 |
Paediatric Asthma Caregiver's |
There was a significant negative correlation betweencaregiver's quality of lifescores and asthma day symptoms, asthma night symptoms, and asthma exercise symptoms. Asthma severity and other asthma factors increased,caregiver's quality of life scores decreased. |
| Quality of Life Questionnaire |
| The Asthma Severity Questionnaire |
| Crespo et al. [26] |
To test the links between caregiver burden, family environment, and quality of children with asthma andthe primary caregiver. |
97 |
Self report |
Descriptive Relational |
8-18 |
The Revised Burden Measure |
Parents’ perceptions of family environment mediated the link between caregiver burden and parents’ quality of life. More positive perceptions of family environment were linked to better QoL for parents and children. |
| World Health Organization |
| Quality of Life [WHOQOL BREF] |
| The Family Environment Scale |
| DISABKIDS Chronic Generic Module |
| Dalheim-Englund et al. [20] |
To test the relation betweencaregiver’s quality of life and other variables. |
371 |
Self report |
Descriptive |
7-17 |
Paediatric Asthma Caregiver's Quality Of Life Questionnaire (PACQLQ) |
There is a positive significant relation between the severity of asthma and caregiver’s quality of life. Several other factors affecting parents quality of life are available as well asasthma. |
| Dean et al. [22] |
To test children andcaregivers' quality of life and efficiencies. |
360 |
Self report |
Descriptive |
06-12 |
Child Health Questionnaire Parent Form 28 (CHQ-PF28) |
Caregivers of children with asthma face many challenges.Uncontrolled asthma symptoms have a negative influence on child and parent’s quality of life. |
| Work Productivity and Activity Impairment Questionnaire. |
| Caregivers' Quality of Life (QOL) |
| Everhart et al. [13] |
To test the relationship between a cumulative risk model and caregiver quality of life (QOL) in pediatric asthma. |
193 |
Self report |
Descriptive |
5-12 |
Pediatric Asthma Caregiver’s |
The cumulative risk model significantly predicted caregiver QOL. Caregivers experience difficulties to overcome with the disease of the child when they expose to multi risks factors. |
| Quality of Life Questionnaire (PACQLQ) |
| Impact on the Family Scale |
| Family Inventory of Life Events |
| Fieseet al. [6] |
To test the relation between asthma management routines and health care utilization, medical adherence and quality of life. |
153 |
Self report |
Descriptive |
5-18 |
Asthma Routines Questionnaire Adherence to Clinical Trials Interview |
The perceived burden of routine asthma care was negatively linked to both parents’ and children’s QoL. |
| Functional Severity of Asthma Questionnaire |
| Caregiver Quality of Life |
| Pediatric Quality of Life |
| Fiese et al. [6] |
To test whether family disease management practices affect child’s emotional functionality. |
60 |
Self report |
Descriptive |
5-13 |
Functional symptom severity |
There is a negative significant relation between burden of asthma care and quality of life of the child and anxiety level. Caregiver and child interaction is linked with perceived burden of asthma routines. |
| Family Routines Questionnaire Asthma Version |
| Pediatric Asthma Quality of Life Questionnaire |
| Multidimensional Anxiety Scale for Children |
| Halterman et al. [16] |
To test the relationship between quality of life of caregivers and asthma severity and socio-demographic factors. |
180 |
Self-report |
Descriptive |
3-7 |
Paediatric Asthma Caregiver's Quality of Life Questionnaire (PACQLQ). |
Caregivers quality of life is directly associated with child’s asthma severity. |
| Laforest et al. |
To test the quantity of asthma-related work-loss of caregivers. |
Undefined |
Database search and self report |
Retrospective observational |
6-16 |
Questionnaire form prepared by researchers. |
Caregivers report that 30% of them have experienced work-loss during 12 months and more than 13% of them have experienced it more than 5 days. There is a negative relationship between work-loss and poorly asthma control. |
| Laster et al. [23] |
To identify the barriers perceived by children with asthma and their caregivers. |
28 |
Interviews |
Qualitative |
8-17 |
Focus groups interviews |
Children and parents’ beliefs and perceptions are distinctive determinants for daily medication use. Psychological distress is a burden for the management of a chronic disease. |
| Moonie et al. [24] |
To test the relation between the child’s quality of life and caregiver’smissed work days. |
248 |
Self report |
Descriptive |
6-19 |
Pediatric Asthma Quality of Life Questionnaire (Parent report ) |
There is a negativerelation between child’s quality of life and caregiver’s missedwork days. |
| Morawskaet al. [9] |
To test the child behavior and asthma management tasks parents experience difficulties. |
255 |
Self report |
Descriptive |
2-10 |
Strengths and Difficulties Questionnaire (SDQ) |
Dysfunctional parenting related withasthma behaviour difficulties. |
| Parenting Scale, |
| Asthma Behavior Checklist (ABC) |
| Asthma Parent Tasks Checklist (APTC) |
| Nagano et al. [27] |
To testrelationships between a mother’s stress-related conditions and parenting attitudes and their children’s asthmatic status. |
274 |
Self report |
Descriptive |
2-12 |
“Stress Inventory |
Different types of parental stress coping behaviors and parenting styles might affect asthma control of the child. Anger and emotional suppression have a negative influence on asthma prognoz of the younger children. |
| Ta-ken Diagnostic Test |
| for Parent-Child Relationship (Parent Form) |
| Price et al. [19] |
To test the relation between caregiver’s quality of life and disease burden. |
98 |
Self report |
Relational -Descriptive |
Undefined |
Pediatric Asthma Caregiver's Quality of Life Questionnaire |
Asthma has a great influence on caregiver’s quality of life. A significant relationship between health care utilization and quality of life has been detected. |
| Brief Symptom Inventory |
| Reichenberg and Broberg [14] |
To test the way how parents grade impaired activities and emotional concerns affect caregiver’s quality of life. |
61 |
Self report |
Descriptive |
7-9 |
Paediatric Caregiver's Quality of Life Questionnaire (PACQLQ) |
There are differences in the answers of fathers and mothers to the PACQLQ. Mothers were more disturbed at night, felt more helpless and frightened and the child's asthma interfered more with their work. |
| Sampson et al. [12] |
To conceptualize stress within asthma experiences of caregivers. |
40 |
Semi-structured interviews |
Qualitative |
Undefined |
Zarit Burden Caregiver Scale |
Caregivers experience stress due to the disease. They experience high level of anxiety owing to sudden morbidity and mortality risks. |
| Peds Quality of Life Family Impact Module |
| Scheckner [21] |
To test the relationship between acculturation, social support, and asthma control among children and their caregivers. |
267 |
Self report |
Descriptive |
5-12 |
The Stephenson Multigroup Acculturation Scale (SMAS) |
Social support reduces some of the burden associated with asthma management enabling caregivers to better control their children’s asthma. Acculturation did not a determinant for asthma control. |
| Social NetworksQuestionnaire |
| The Asthma Control Test (ACT) |
| Silva et al. [17] |
To test the director indirect associationbetween caregiver burden and quality of life through refuse or accept coping. |
182 |
Self report |
Descriptive |
8-18 |
World Health Organization Quality of Life questionnaire (WHOQOL-BREF) |
Higher levels of caregiverburden were negativelyassociated with the parents’ QoL. |
| Terpstra et al. |
To test asthma management interventions based on findings of caregiver for the child and his caregiver. |
58 |
Self report |
Quasi-experimental |
5-12 |
Caregiver self-efficacy Questionnaire |
Direct interventions to parents improved their self-efficiency and motivating adolescent to access asthma resources increased the quality of life of the caregiver. |
| Caregivers quality of life (QOL) |
| Vila et al. |
To test the relationship between emotional and behavioral problems and quality of life. |
100 |
Self report |
Descriptive |
12-19 |
Pediatric Asthma Quality of Life Questionnaire |
Quality of life of the child and the caregiver is not only dependent on medical conditions but also associated with the presence or absence of psychologicalproblems. |
| Pediatric Asthma Caregiver’s Quality of Life Questionnaire |
| The Child Behavior Checklist |
| Toulouse Self-Esteem Scale |
| Williams et al. [28] |
To test the relation between severity of asthma and quality of life of the child and his caregiver. |
240 |
Self-report |
Descriptive |
5-12 |
Child's Quality of Life |
Higher level of asthma severity leads to lower level of quality of life for the caregiver. According to caregiversasthma care of the child as one of their daily-problems. There is a negative significant relation between child’s school absence and caregivers quality of life. There is a positive correlation between the caregiver’s knowledge of symptoms and child’s quality of life scores. |
| Caregiver's Quality of Life |
| Clinical Asthma Triage Scores |
| Caregiver's Asthma Knowledge |
| Asthma Severity Score |
In the studies examined, the sample was composed of 3.666 parents who assumed the role of primary caregivers of children with asthma aged between 2-18 years. The mean ages of caregivers were 32.4 ± 5.2 years and 91% of them were mothers. The mean ages of children with asthma were 8.2 ± 5.3 years and mean duration of their diseases were 6.6 ± 3.5 years. All of the children got daily controller medications. The studies mainly focused on (82.3%) quality of lives of caregivers, one of the studies focused on the effect of caregiving activities on parents’ loss of work, one of them focused on the relation between acculturation-social support and asthma control, and finally one of the studies focused on the effect of disease management practices on child’s emotional functionality.
Quality of life
According to study results examined in this review, poor socio-economic status, low educational status, poorly controlled asthma symptoms, higher rates of health care use and being the single parent are among the risk factors leading poor quality of life [12]. In their study, Everhart et al. [13] assessed the quality of lives of caregivers through multi-risk model (socioeconomic status, single versus two-caregiver households, asthma severity, child QOL, family burden, and family stress) and they found out a non-linear relation between the risk model and quality of life. So it can be deduced that the quality of lives of caregivers are not affected by a single factor but by multiple factors.
There is a negative significant relation between severity of asthma and caregiver’s quality of life. Higher severity of child’s asthma causes lower quality of life for the caregiver [14-19]. Furthermore; there is a similar relation between lower level quality of life and child asthma morbidity and the quality of lives of the caregivers who admitted to the emergency service for their children once or more last year [13]. Quality of life of the caregiver does not differ significantly in terms of age or gender of the child [14]. Moreover, being a single parent affect the quality of life negatively in terms of psychological and social domains [15,20].
In the studies, preventive factors were examined as well as the factors affecting the quality of life. Social support is the major factor relieving the burden of caregiver [21]. Having another adult in the house is stated as factor enhancing the quality of life of the caregiver [22-24]. Moreover; secondary caregiver’s participation in the asthma management process promotes the social support perception of primary caregiver [18].
Stress
Caregivers of the children with asthma expose to several stressors [17,25,26]. In the studies those stressors are identified as caregiving activities (preventing symptoms, intervening to symptoms), financial burden, parental responsibilities and personal distress. In the studies, stress levels of caregivers of children with asthma have been reported as rather higher [17,18,27]. The studies assessing the stress levels pointed out that stress levels of caregivers decreases significantly especially after six months. Asthma diagnosis and asthma management practices are the prominent stressors for the caregiver [18]. Income status, marital status, and caregiver-child relationships are all risk factors causing stress. Stress is classified as daily life stress and asthma management stress. High level perception of daily life stress (unemployment, low-income, neighborhood safety, community violence exposure) and asthma caregiving stress are all associated with lower quality of life [17].
Discussion
Providing daily care to the child is a part of parenting role. However, providing high level of care to the child with a chronic disease can become burdensome that affects the physical and psychosocial health of the caregiver negatively [8,13]. Delivering care to the child with a chronic disease is an unexpected, multidimensional and complex experience for caregivers. Such an unexpected and complex experience might lead to a stressful life and various health problems [6,10].
Childhood diseases affect not only the child himself but also his parents as primary caregivers. Even though it differs the type of the disease and the condition of the child, caregivers need to overcome routine changes such as extra expenses for medication and equipments or extended time for the caring of the child. As for the chronic diseases like asthma, increasing responsibility and extra efforts of the caregivers affect their physical and psychosocial health [15]. The studies conducted on that issue state that the child with asthma and his caregiver are under the risk of reduced physiological functionality, deteriorated well-being and quality of life. In this review it is aimed at the searching of certain studies addressing the life of caregivers having a child with a chronic disease. In the studies examined for the review it was observed that they measure the quality of life to assess well-being level of caregivers. Quality of life is a commonly utilized measurement technique since it ensures a wide assessment of well-being among domains of life. Quality of life is a subjective concept that allows different interpretations and involves physical, emotional and social well-being domains. Furthermore, it implies satisfaction of life within the contexts of daily functionality, financial status, environment and culture. The results of several studies suggest that quality of life of the caregivers of children with chronic diseases is affected negatively [26]. The leading factor for deterioration of quality of life is severity of asthma. Severe asthma suggests lower level of quality of life for parents as caregivers [15,17,28].
Increasing in the severity of asthma, high level care, access to medical care, appropriate medication require more attention to environment design and emotional support to the child. The needs of the child causes his caregiver spend more effort. Such an effort decreases the quality of life of the caregiver since it affects the caregiver’s physical and emotional health. Besides, socioeconomic status is another factor affecting the quality of life of the caregiver. Those caregivers with a lower socio-economic status have a lower quality of life compared to others with higher socioeconomic status [15,17]. According to results of this study, caregivers of the children with asthma often experience anxiety, fear, disappointment, grief and physical distress as the outcomes of caregiving. The stress experienced by the parents is closely related with possible asthma attack. Reichenberg and Broberg [14] states in his study that mothers of the children with asthma express that they feel fear not to help their children during an asthma attack.
To sum up; caregiving includes not only regular parenting tasks but also the management of disease. Asthma management skills are multi-sided; use of drugs, environmental control, intervening to symptoms are among the extra tasks which parents should achieve. Those repetitive and long-term tasks might be a burden for parents and also they reason negative biopsychosocial effects. In order to develop effective asthma programmes, parents need to assess their caregiver burden together with their experiences.
The most important limitation of this review is the limited number of studies evaluating caregiver burden directly even though good number of studies evaluating the effect of asthma on parents are available. Besides; the studies on caregiver burden for asthma are descriptive and the number of interventional studies on that issue are too limited. This review might a light the future interventional studies by identifying the effects of parental caregiving burden for pediatric asthma.
Conclusion
It is obvious that providing care to the child with asthma affects parents as caregivers negatively. One of the important outcomes of this review is the identification of asthma affects not only the child but his primary caregiver by health professionals. Secondly; the limitation of data including interventional strategies for the caregivers of children with asthma. Appropriate caregiving intervention programmes targeting to increase well-being of caregivers, is necessary in the future. The outcomes of those programmes should focus on supporting the parents in order to develop better disease management skills, increase their quality of life, and develop better daily routines. All of the planned interventions will surely improve the quality of life of both parent and the child himself.
Conflict of Interest
The authors confirm that they have no significant financial or personal interest in the products, technology, or methodology mentioned in the submitted manuscript.
17871
References
- Hermanns M,Mastel-Smith B (2012) Caregiving: A qualitative concept analysis. Qual Rep 17: 1-18.
- Mendez-Luck C, Kennedy DP,Wallace SP (2009) Guardians of health: The dimensions of elder caregiving among women in a Mexico City Neighborhood. SocSci Med 68: 228-234.
- Swanson EA, Jensen DP, Specht J, Johnson ML, Maas M, et al. (1997) Caregiving: Concept analysis and outcomes. SchInqNursPract 11: 65-76.
- Zarit S, Todd P, Zarit J (1986) Subjective burden of husbands and wives as caregivers: A longitudinal study. Gerontol 26: 260-266.
- Dang S, Badiye A, Kelkar G (2008) The dementia caregiver – a primary care approach.South Med J 101: 1246-1251.
- Fiese BH, Wamboldt FS, Anbar RD (2005) Family asthma management routines: Connections to medical adherence and quality of life. J Pediatr 146: 171-176.
- Chou KR (2000) Caregiver burden: A concept analysis. J PediatrNurs 15: 398-407.
- Brown E, Gan V, Jeffress J, Khan DA, Wood BL, et al. (2006) Psychiatric symptomatology and disorders in caregivers of children with asthma. Pediatrics 118: 1715-1720.
- Morawska A, Stelzer J, Burgess S (2008) Parenting asthmatic children: Identification of parenting challenges. J Asthma 45: 465-472.
- Streisand R, Tercyak KP (2004) Parenting children with physical and medical problems. In: Long N,Hoghughi M (Eds.), Handbook of parenting: Theory, research, and practice. Sage Publications, London, UK. pp: 181–197.
- Joanna Briggs Institute (2011) Joanna Briggs Institute Reviewers’ Manual. Australia.
- Sampson NR, Parker EA, Cheezum RR, Lewis TC, O'Toole A, et al. (2013) "I wouldn't look at it as stress": Conceptualizations of caregiver stress among low-income families of children with asthma. J Health Care Poor Underserved 24: 275-288.
- Everhart RS, Fedele DA, Miadich SA, Koinis-Mitchell D (2015) Caregiver quality oflife in pediatric asthma: Associations with beliefs and concerns about medications and emergency department use. ClinPediatr 54: 249-256.
- Reichenberg K, Broberg AG (2001) The paediatric asthma caregiver's quality of life questionnaire in Swedish parents. ActaPaediatr 90: 45-50.
- Cerdan NS, Alpert PT, Moonie S, Cyrkiel D, Rue S (2012) Asthma severity in children and the quality of life of their parents. ApplNurs Res 25: 131-137.
- Halterman JS,Yoos HL, Conn KM, Callahan PM, Montes G, et al. (2004) The impact of childhood asthma on parental quality of life. J Asthma 41: 645-653.
- Silva N, Crespo C, Carona C, Canavarro MC (2015) Mapping the caregiving process in paediatric asthma: Parental burden, acceptance and denial coping strategies and quality of life. Psychology Health 30: 949-968.
- Bellin MH (2015) Stress and quality of life in urban caregivers of children with poorly controlled asthma: A longitudinal analysis. J Pediatr Health Care 29: 536-546.
- Price MR, Bratton DL, Klinnert MD (2002) Caregiver negative affect is a primary determinant of caregiver report of pediatric asthma quality of life. Ann Allergy Asthma Immunol 89: 572-577.
- Dalheim-Englund AC, Rydström I, Rasmussen BH, Möller C, Sandman PO (2004) Having a child with asthma-quality of life for Swedishparents. J ClinNurs 13: 386-395.
- Scheckner B, Arcoleo K, Feldman JM (2015) The effect of parental social support and acculturation on childhood asthma control. J Asthma 52: 606-613.
- Dean BB, Calimlim BC, Sacco P, Aguilar D, Maykut R, et al. (2010) Uncontrolled asthma: assessing quality of life and productivity of children and their caregivers using a cross-sectional Internet-based survey. Health Qual Life Outcomes 8: 96.
- Laster N, Holsey C, Shendell DG, Celano M (2009) Barriers to asthma management among urban families: Caregiver and child perspectives. J Asthma 46:731-739.
- Moonie S, Huang S, Sterling DA (2009) Quality of life estimation with structural equation modeling in school aged children with asthma. Global Health Governance 3: 1-16.
- Kaugars AS, Klinnert MD, Bender BG (2004) Family influences on pediatric asthma. J PediatrPsychol 29: 475-491.
- Crespo C, Carona C, Silva N, Frank M, Dattilio (2011)Understanding the quality of life for parents and their children who have asthma: Family resources and challenges. ContempFamTher 33: 179-196.
- Nagano J, Kakuta C, Motomura C, Odajima H, Sudo N, et al. (2010) The parenting attitudes and the stress of mothers predict the asthmatic severity of their children: A prospective study. BioPsychoSocial Med 4: 12.
- Williams S (2000) Effect of asthma on the quality of life among children and theircaregivers in the Atlanta Empowerment Zone. J Urban Health 77: 268-279.

