Keywords
infertility - female reproductive age - causes of infertility
Introduction
Childbearing and raising of children are extremely important events in every human’s life and are strongly associated with the ultimate goals of completeness, happiness and family integration. It is widely accepted that human existence reaches completeness through a child and fulfils the individual’s need for reproduction. Human fertility, compared with other species of animal kingdom, is unfortunately low [1-4].
According to recent studies by the World Health Organization (WHO), approximately 8-10% of couples are facing some kind of infertility problem. Globally, this means that 50-80 million people are facing the problem of getting an integrated family. In the USA, approximately 5 million people have infertility problems, while in Europe the incidence is estimated around 14% [1-4].
The incidence of infertility is associated with geographic differences. For example, in some west-African communities infertility rate is around 50%, while in some western European countries is 12%. Likewise, differences are observed both in developed countries, where rates range from 3.5% to 16.7%, as well as in less developed countries, where rates of infertility range from 6.9% to 9.3%. It has also been observed that the causes are related to geographical differences. Especially in Western countries, the most common risk factor of infertility is age, while in Africa is sexually transmitted diseases [1-4].
Infertility is defined as the inability of getting pregnant after trying for at least 6 months or one year, for women over 35 years old, without use of birth control means and while having normal sexual intercourse. Assisted reproduction includes all the methods used for fertilization, which is not achieved through sexual intercourse [5].
In the past, people had little control over their fertility and couples that could not get a child had no other choice but to accept the fact. In contrast, although today infertility is a relatively common problem that touches deeply the soul of couples involved in this, medical science has increased the chances of giving solutions to the problem with the Assisted Reproduction.
The first successful fertilization of human eggs in the laboratory was in 1978. The fact of the first child-birth by this process was a real milestone because it gave hope to the infertile couples as it offered a possible solution to the problem. Furthermore, in the USA, the first successful childbirth in 1981 through Assisted Reproduction led to rapidly increasing application of this method and the creation of specialized centers [5-6].
The purpose of this study was to investigate the causes of infertility in women of reproductive age.
Material and method
The study population consisted of infertile women who sought medical assistance to a private Center for Assisted Reproduction and were selected by random sampling method. For data collection, a specially designed questionnaire for the purpose of the research was used. The questionnaire included both the demographic characteristics of the population and questions regarding the causing factors of infertility. The data collection lasted for two months.
The type and the wording of questions were carefully selected in order to preserve the anonymity of the participants and create confidence.
The statistical program SPSS 13 (Statistical Package for the Social Sciences) was used for the data analysis.
Results
The studied population consisted of 110 infertile women.
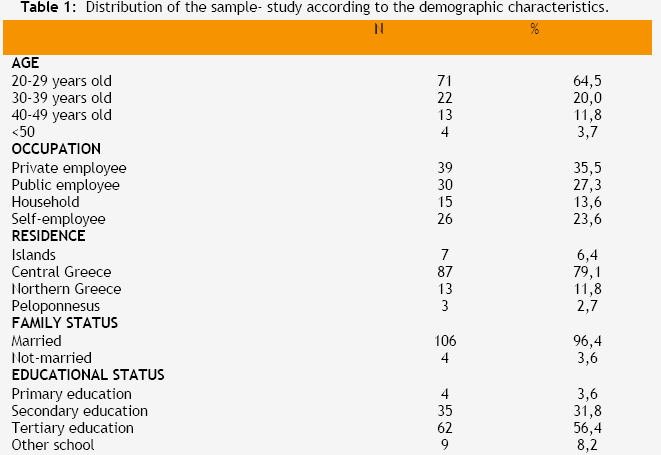
Regarding age, 64.5% of the 110 women coming to the center of the Assisted Reproduction and agreeing to participate were 20-29 years old, 20.0% were 30-39 years old, 11.8% were 40-49 years old and 3.7% were above 50 years old. Regarding family status, 94.4% (106) of the women were married and 3.6% (4) were single. The last ones were addressed in Assisted Reproduction not because of a specific gynecological problem that wouldn’t allow them to have children, but because they wanted to have children with the use of artificial insemination.
Regarding educational status, 56.4% of the participants were university graduates or graduates from technical institutions, 27.3% were high school graduates, 8.2% were graduates from different institutions, 4.5% were gymnasium graduates and 3.6% were primary school graduates.
Regarding the profession of the study population, 35.0% were employees in the private sector, 27.0% were employees in the public sector, 24.0% were self-employees and 14.0% dealt with household.
Regarding residence, 79.1% of the couples lived in Central Greece, 7.0% in the islands and 3.0% in Peloponnesus. (Table 1).
The results of the present study showed that the most common cause of female infertility was problems in the fallopian tubes in 27.4% of the cases, while the second most common cause was the infertility by « unknown causes», in the 24.5%.
53.6% of respondents with infertility of «unknown cause» had made several attempts of Assisted Reproduction.
The third most common cause was disorders of menstruation in the 20% of the cases, following infertility due to problems in the uterus in the 9.1% of the cases. Finally, in 2.7% of the participants infertility was due to age, an additional 2.7% due to sexual disorders and the last cause was the ovarian failure, which was common for the majority of the women tested. (Table 2).
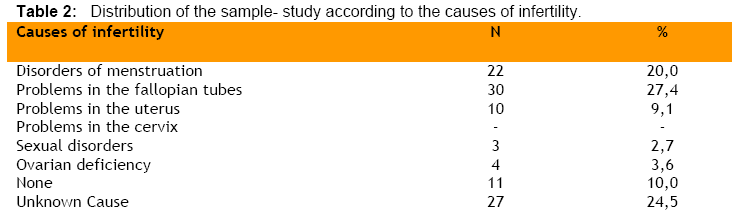
None of the women who responded to our questionnaires was facing cervix problems.
As to the habits of the participants, 45.5% were smokers and 54.5% non-smokers. (Table 3).

Discussion
According to the literature, infertility seems to be a multidimensional health issue which occurs not only due to health problems related to the fallopian tubes, the ovaries, and the endometrium, but it may also be a result of the choices imposed by the modern lifestyle, like the higher average age of people who get married, stress, non-conducive legal framework for assisted reproduction, etc.
The results of the present study showed that a high proportion of women aged 20-40 years took part in a program of assisted reproduction, possibly because this is the reproductive age period among women. However, it should be noted that, statistics in Greece show that it is mainly older women who participate in Assisted Reproduction [1,7].
It is widely accepted that during the last twenty years, the average age of having children has increased and this is a key factor for infertility. As the age of giving birth is increased, the reproductive capacity is decreased, the ovary becomes less efficient, the frequency of sexual intercourse is decreased and the possibility of chromosomal abnormalities and miscarriage is increased [1,7].
The results also showed that the majority of women who took part in the study were employees in the public or the private sector. One possible interpretation of the finding is that women who work, are in daily contact with other people, exchange ideas, are well informed and receive various stimuli in the working environment, which makes them face the assisted reproduction in a more positive way. As a matter of fact, the general changes in women’s belief and view about their role in modern society, makes it easier for them to ask help in an Assisted Reproduction center. In addition, the entry of women in the professional arena, the high professional competition, and the effort to obtain a comfortable life and financial security are important factors that lead to a delayed childbearing. Specifically, women who have very high career goals, often try to delay pregnancy by using contraceptives for very long time, which unfortunately have negative effects in a couple’s fertility. Finally, the daily stress and the new high-demanding way of living have adverse effects on the reproductive capacity [8-15].
Regarding educational level, the largest proportion of the participants who were in a program of assisted reproduction was high school or University graduates. According to the literature, age and demographic factors such as socio-economic status and education, are positively associated with seeking help in Assisted Reproduction centers. More in detail, women with higher income and educational level, as well as those who have insurance coverage, are subjected more often to Assisted Reproduction treatments compared to those who have a lower income. Specifically, couples that have low income are forced to seek help after several non-successful physiological attempts, because of the high cost of the treatment or the small insurance coverage. However, this entails loss of valuable time and direct inclusion in a particular program applied to women of an older age [14,17-22].
Unfortunately, until now in Greece, inadequate insurance arrangements for the treatment of infertility and the rudimentary refund that is given to the patients, has made it very difficult for the women to try one of these possible treatments. According to the law in Greece, all public insurance companies are obliged to provide a small amount of money, approximately 360 euros for each Assisted Reproduction attempt. Overall, the number of attempts that a woman can make after the approval from the insurance company does not exceed four, and the time between attempts varies from three to four months, depending on the company [23-24].
The largest proportion of couples in this study lives in Central Greece. One possible explanation for this finding is that women prefer centers of Assisted Reproduction in large cities, away from their residence, because they think that they will be of a better treatment and they will ensure privacy and medical confidentiality. Due to lack of official control committee for the quality of the Assisted Reproduction centers, special attention is required, because the selection of the applied methods and the control of their effectiveness are not always feasible. The process of defining the criteria for granting operating licenses to these centers is also crucial. Each center should have the necessary infrastructure, as well as highly trained medical and nursing staff in order to meet each couple’s need [17-22].
The fact that the majority (96.4%) of the women in the study are married, shows that having children within marriage is a powerful institution in Greece. Another possible explanation is that the diagnosis of infertility, and thus the discovery of the problem, becomes perceptible only when the women get married and decide to have children. Apart from the married women, there were 4 single women, who had visited one of the Assisted Reproduction centers without having an infertility problem. Their hope was to have children with artificial insemination, where fertilization is achieved with sperm from donors. This method has been applied in Greece for several decades, but the results are not known, at national level at least, because most of the centers are private and do not show their data to the National Statistical Service [24].
In many parts of the world there is a strong social and religious opposition to the selection of artificial insemination as a method of child-bearing. Some years ago, the use of donor sperm was considered as a condemnable act contrary to the ethical concepts of the Greek and some European societies. Today though, it is regulated by several European legislations. According to the literature, it is mainly single or women of an older age that choose this method, a conclusion that is in line with our findings. Results from a recent study in Denmark showed that 1/3 of the sperm donors had a positive attitude towards artificial insemination for women without a partner but then, the motivation of the donors was mainly economic. Similarly, positive attitude towards artificial insemination for women without a partner was found from a study carried out in Greece, in which approximately 50% of the participants were ready to donate or accept donation of sperm. The anonymity of the donor has been the subject of many investigations, which concluded that the notification of their identity is a key factor of sperm donation. In Greece, there are private sperm banks, which may ensure anonymity and financial benefits to donors, but are not controlled as to the origin of semen. Therefore, specific legislation is necessary for the establishment and operation of sperm banks [25-33].
As for the causes of female infertility, these relate mostly to the hypothalamus, the pituitary gland, the ovaries, the fallopian tubes, the body of the uterus, the cervix of the uterus and the vagina. Both the anatomical and functional adequacy is essential for successful conception [34].
The conclusion from the participants’ responses was that problems related to the tubes are the primary cause of female infertility and then follows the «unknown cause».
The main cause of infertility related to the fallopian tubes is any condition affecting the normal function and anatomy of the fallopian tubes and prevents the meeting of sperm with the ovum and the consequent conception. The development of ectopic intrauterine tissue occurs mainly in women aged 30-40 years old and is called "disease of high social class" because it occurs more often in advanced countries. This specific condition is more common among the women that have given birth many times before and those that give birth in an older age. Finally, the use of contraception methods, such as intrauterine spirals, can sometimes contribute to infertility because they can cause inflammation and destruction of the fallopian tubes [35,36].
Although the most important step in the Assisted Reproduction is investigating the cause of infertility, in this study, it was observed that 10.4% did not know the cause of infertility. The failure to identify a clear cause of the infertility after a full screening of both partners is defined as infertility of «unknown cause» [34-38].
In the present study, 20% of the infertility was due to menstrual disorders, which often occur as a result of metabolic diseases. It is known that the function of the thyroid gland is directly affected by the relationship of hypothalamic-pituitary gland-ovarian hormones. The increased function of the thyroid is likely to cause disorders in menstrual cycle, and an increase or decrease in women’s sexual activity, while the decreased function of the gland causes a decrease in sexual activity, and/or increased flow during menstruation, bleeding of the uterus, and more rarely secondary amenorrhea. Also, neoplasms may be the cause of thyroid dysfunction, and disorders in the pituitary gland may cause decreased function of the thyroid. Finally, changes in the menstrual cycle can occur under stress conditions [34-38].
The second common cause (9.1%) of infertility was problems in the uterus. The main problems that are related to the body of the uterus and cause infertility are malformations, abnormal positions of the uterus, inflammation, intrauterine symphysis, atrophy of the endometrium, and malignant neoplasm [34-38].
Four women had experienced ovarian failure. The main cause of infertility related to the ovaries is inability of ovulation, a condition where the release of the egg is for some reason prevented. Other common problems are inflammation of the ovaries, endometriosis, polycystic ovarian syndrome and neoplasms. Also, infertility may be associated with impairment of luteal phase where after ovulation, the fertilized egg is not possible to be implanted in the uterus [34-37].
According to our results, sexual disorders are the cause of infertility in a percentage of 2.7%. Sexual disorders may be a result of the above mentioned health problems or follow problems in the couple’s relationship.
Besides the health problems related to the female anatomy, another major factor that causes infertility is smoking. The harmful effects of smoking on health, during the reproductive age of men and women, have started to be investigated during the last 20 years. Several studies have highlighted the harmful effects of active and passive smoking on fertility, in women of reproductive age, as well as a significant reduction in the possibility of a successful outcome after assisted reproduction attempt. While smoking is one of the main causes of infertility and most of the population in Greece is aware that has many negative consequences, about half of the female population smokes regularly, and only 20% of these considers to quit smoking [38-42].
Other causes that are likely to cause infertility, but not explored in this study, are: diseases affecting the function of the ovaries, dietary problems such as excessive increase or decrease in body weight, exposure to radiation, chemical agents, cytotoxic drugs, orgasm disorders and psychological causes.
Conclusion
Childbearing and family are considered a right of every human being. Infertility is a health problem that requires appropriate treatment strategy. Modern medical science has developed advanced therapies to assist reproduction over the last 20 years. The main causes of female infertility are the problems of the fallopian tubes, disorders of menstrual cycle, problems in the uterus, sexual disorders, age, ovarian failure, and other unknown causes.
The Greek state must try to understand the problem of this portion of the population and show interest, in order to allocate the necessary resources to solve it. The medical and socio-economic support of infertile women, which means easier access to medical services, higher insurance coverage, broader social support, and information are important requirements for resolving the problem.
3642
References
- Gnoth C., Godehardt E., Frnk-HerrmannP., Friol K., Tigges J., Freundl G. Definition and prevalence of subfertility and infertility. Hum Reprod. 2005 ;20(5):1144-7.
- Benagiano G., Bastianelli C., Farris M. Infertility: a global perspective. Minerva Ginecol. 2006 Dec;58(6):445-57.
- Kelly-Weeder S., Cox CL. The impact of lifestyle risk factors on female infertility. Women Health. 2006;44(4):1-23.
- Boivin J., Bunting L., Collins JA., Nygren KG. International estimates of infertility prevalence and treatment-seeking: potential need and demand for infertility medical care. Hum Reprod. 2007;22(6):1506-12.
- Ombelet W., Cooke I., Dyer S., Serour G., Devroey P. Infertility and the provision of infertility medical services in developing countries. Hum Reprod Update. 2008;14(6):605-21.
- The CDC, American Society for Reproductive Medicine, and Society for Assisted Reproductive Technology. 2001 assisted reproductive technology success rates. Atlanta, GA: US Department of Health and Human Services, CDC, 2003.
- Baird DT., Collins J., Eqozcue J., Evers LH., Gianaroli L., Leridon H., et al. Fertility and ageing. Hum Reprod Update. 2005;11(3):261-76.
- Klein J., Sauer MV. Assessing fertility in women of advanced reproductive age. Am J Obstet Gynecol. 2001;185(3):758-70.
- Rowe T. Fertility and a woman's age. J Reprod Med. 2006 ;51(3):157-63
- Tabs D., Radunović N. Significance of maternal and paternal age in assisted reproduction programs. Med Pregl. 2002;55(11-12):535-8.
- Boivin J., Bunting L., Collins JA., Nygren KG. International estimates of infertility prevalence and treatment-seeking: potential need and demand for infertility medical care. Hum Reprod. 2007;22:1506–1512.
- Baird DT., Collins J., Egozcue J., Evers LH., Gianaroli L., Leridon H., et al. Fertility and ageing. Hum Reprod Update. 2005;11(3):261-76.
- Pal L., Santoro N. Age related decline in fertility. Endocrinol Metab Clin North Am. 2003;32(3):669-88.
- Palomba S., Falbo A., Del Negro S., Russo T., Zullo F. Use of oral contraceptives in infertile patients: A descriptive review. Gynecol Endocrinol. 2006;22(10):537-46.
- Hamilton BE., Ventura SJ. Fertility and abortion rates in the United States, 1960-2002. Int J Androl. 2006;29(1):34-45.
- Engelhardt H., Kögel T., Prskawetz A. Fertility and women's employment reconsidered: a macro-level time-series analysis for developed countries, 1960-2000. Popul Stud (Camb). 2004;58(1):109-20.
- Maroto-Navarro G., del Mar García-Calvente M., Mateo-Rodríguez I. The challenge of maternity in Spain: social and health difficulties. Gac Sanit. 2004;18 Suppl 2:13-23.
- Sołtysiak E. The influence of socioeconomic factors on female fertility. Ginekol Pol. 2005;76(12):986-90.
- Stephen EH., Chandra A. Use of infertility services in the United States: 1995. Fam Plann Perspect. 2000;32(3):132-7.
- Bitler M., Schmidt L. Health disparities and infertility: impacts of state-level insurance mandates. Fertil Steril. 2006;85(4):858-65.
- Jain T. Socioeconomic and racial disparities among infertility patients seeking care. Fertil Steril. 2006;85(4):876-81.
- Izugbara CO., Afangideh AI. Urban women's use of rural-based health care services: the case of Igbo women in Aba City, NigeriaJ Urban Health. 2005;82(1):111-21.
- Schenker JG. Assisted reproduction practice in Europe: legal and ethical aspects. Hum Reprod Update. 1997;3(2):173-84.
- Pennings G. The right to choose your donor: a step towards commercialization or a step towards empowering the patient? Hum Reprod. 2000;15(3):508-14.
- American Society For Reproductive Medicine. Assisted Reproductive Technology In The United States – Fertility and Sterility. 2002;77(1): 81-31.
- Westlander G., Janson PO., Tägnfors U., Bergh C. Attitudes of different groups of women in Sweden to oocyte donation and oocyte research. Acta Obstet Gynecol Scand. 1998;77(3):317-21.
- Chliaoutakis JE. A relationdhip between traditionally motivated patterns and gamete donation and surrogacy in urban areas of Greece. Hum Reprod. 2002 August;17(8):2187-91.
- Purewal S., van den Akker OB. British women's attitudes towards oocyte donation: ethnic differences and altruism. Patient Educ Couns. 2006;64(1-3):43-9.
- Ernst E., Ingerslev HJ., Schou O, Stoltenberg M. Attitudes among sperm donors in 1992 and 2002: a Danish questionnaire survey. Acta Obstet Gynecol Scand. 2007;86(3):327-33.
- Daniels K., Feyles V., Nisker J., Perez-y-Perez M., Newton C., Parker JA., et al. Sperm donation: implications of Canada's Assisted Human Reproduction. Act 2004 for recipients, donors, health professionals, and institutions. Obstet Gynaecol Can. 2006;28(7):608-15.
- Lieberman BA., Brison DR. Mixed opinions on egg sharing. Lancet. 2003;362(9394):1502.
- Svanberg AS., Lampic C., Bergh T., Lundkvist O. Characterization of potential oocyte donors in Sweden. Hum Reprod. 2003;18(10):2205-15.
- Speroff L., Glass R., Kase N. Clinical Gynecological Endocrinology and Infertility – Lippincott Williams and Wilkins 1999, U.S.A. 1035-1036, 1038-1043
- Hart R. Unexplained infertility, endometriosis and fibroids. BMJ.2003;327(7417):721-4.
- Sépaniak S., Forges T., Monnier-Barbarino P. Cigarette smoking and fertility in women and men. Gynecol Obstet Fertil. 2006;34(10):945-9.
- Practice Committee of the American Society for Reproductive Medicine. Smoking and infertility. Fertil Steril. 2006;86(5 Suppl):S172-7.
- Berthiller J., Sasco AJ. Smoking (active or passive) in relation to fertility, medically assisted procreation and pregnancy. J Gynecol Obstet Biol Reprod. 2005;34 Spec No 1:3S47-54.
- de Mouzon J., Belaisch-Allart J. Consequences on women's fecundity and on assisted reproductive technology. J Gynecol Obstet Biol Reprod (Paris). 2005 ;34 Spec No 1:3S112-8.
- Soares SR., Simon C., Remohí J., Pellicer A. Cigarette smoking affects uterine receptiveness. Hum Reprod. 2007;22(2):543-7.

