Keywords
Stress; Self-esteem; Aerobic exercise; Mindbody exercise; Health Qigong; Children
Introduction
Recent epidemiological research has shown that approximately 20% of school-aged children are suffering from psychological health issues, such as chronic stress, anxiety, depression and low self-esteem, which have resulted in poor academic performance, school failure, disruptive behavior at school and significant economic burdens [1]. According to conservative estimates from the National Mental Health Surveillance Survey, more than $247 billion per year is spent on these psychological health issues among children in the U.S. [2].
The question of how to improve children’s psychological health has been of major interest for several decades. Although the most commonly used treatments for mental health issues in children were medications and psychological counseling, many parents preferred the natural ways to improve their children's mental health status. In fact, many studies indicate that regular exercise can improve psychological well-being [3-5]. A meta-analysis including 25 studies with participants aged three to 20 years has demonstrated that exercise can improve self-esteem [6]. Another systematic review including 30 studies has shown that participating in physical activities can reduce stress and improve emotional well-being and self-efficacy among children [7,8].
Despite the accepted perception of the benefits of exercise, only half of the school-aged children participated in physical education, played in sports or did exercise to strengthen or tone their muscles more than once a week in 2013 [9]. It is hypothesized that one of the reasons why children do not participate in regular exercise is because these traditional exercises are competitive, highly physically demanding, and focus on the development of kinesthetic or motor skills, which is not attractive for children who do not enjoy or perform well with these activities [10]. Therefore, alternative exercise modalities for children to improve their psychological wellbeing is warranted.
With the increasing use of Complementary and Alternative Medicine in the U.S., a variety of Eastern mind-body exercises, such as Yoga, Tai Chi, and Qigong, has gained popularity within the past two decades [11]. Scientific literature has shown that these mind-body exercises (e.g., Tai Chi and Yoga) are effective in enhancing positive emotions, reducing stress, and improving relaxation among adults and the elderly [12-14]. However, the impacts of Health Qigong (i.e., a typical mind-body exercise) on children have not been very well studied [15]. Moreover, even less research has compared the relative effectiveness of Health Qigong with traditional Western exercises, such as aerobic exercise and physical education activities.
To fill this gap, the purposes of this study are to 1) examine if Health Qigong is effective in improving children’s psychological well-being and 2) compare the relative effectiveness of Health Qigong with two traditional Western exercises, aerobic exercise and physical education activities, on children’s mental health.
Methods
Participants and procedures
This study was conducted at two Title I elementary schools in the Midwest US. The inclusion criteria for participation were: (a) enrolled in one of the participating elementary schools and (b) turned in both consent and assent forms. One hundred and fifty students met these criteria. Of these, children who were (a) taking anti-anxiety medication, (b) involved with other mind-body exercise programs (such as Yoga, Tai Chi, and Qigong), or (c) unable to finish the 16-week program were excluded. Consequently, 110 students completed the study. For logistical reasons, random assignment to treatments was performed at the classroom unit level rather than the individual level. Of these participants, one third-grade and one fourth-grade class participated in the aerobic exercise group (AE), another thirdgrade and fourth-grade class participated in the mind-body exercise group (MBE) and another two fourth-grade classes attended the regular physical education program (PE). The participating schools were similar about demographics, location, and program structure.
This study included two months of recruitment, one week of pre-test, a 16-week intervention, and one week of post-test. The flow diagram for this study is depicted in Figure 1.
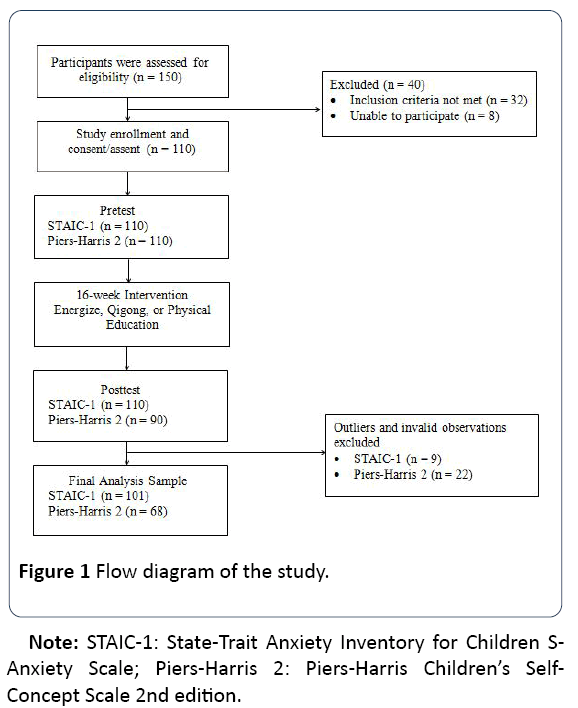
Figure 1: Flow diagram of the study.
Study design
A pre-and post-test quasi-experimental study was conducted to compare the effects of the three different modes of on reducing stress and improving self-esteem in children over a 16-week period using the State-Trait Anxiety Inventory for Children (STAIC) and Piers-Harris Children's Self-Concept Scale 2nd Edition (Piers-Harris 2).
The study protocol was approved by the Institutional Review Board at both Indiana University and the local school district. Both of the consent and assent forms were obtained before the study started.
Instrumentation
The STAIC-1 and Piers-Harris 2 were used to assess stress and self-esteem, respectively.
The STAIC-1 measures how children feel at a particular moment in time [16]. Since this study was conducted in a relatively short-term period of 16-weeks, only STAIC-1 was used. The STAIC-1 consists of a 20-item scale. Each item has three possible response options indicating the extent to which each respondent agrees with the given statement. Typical questions from STAIC-1 include statements like I feel “very calm, calm, not calm,” “very upset, upset, not upset,” or “very pleasant, pleasant, not pleasant.” The STAIC has been deemed one of the best scales available to assess anxiety and stress in children. The Cronbach alpha was 0.89 for STAIC-1 for this study, indicating good reliability.
The Piers-Harris 2 has 60 self-reporting questions with a subtitle “The Way I Feel About Myself.” The survey normally yields a general measure of the respondents’ overall selfesteem and contains six sub-scales: 1) Behavioral Adjustment 2) Intellectual and School Status 3) Physical Appearance and Attributes 4) Freedom from Anxiety 5) Popularity, and 6) Happiness and Satisfaction. Typical questions from this questionnaire include statements like “I can be trusted,” “I do many bad things,” or “I am often afraid.” The children can answer “yes” or “no” for each question. Piers-Harris 2 is regarded as the most psychometrically sound instrument for assessing children’s self-esteem and is highly recommended for use in a classroom setting [17]. The Cronbach alpha was 0.774 for all sub-categories of the Piers-Harris 2 for this study, which indicates relatively good reliability.
Interventions
There were three exercise interventions in this study. All participants attended their respective programs once per week. Aerobic Exercise (Energize in particular) was chosen as one of the interventions. A typical Energize class includes a 10- minute warm-up using the letters E-N-E-R-G-I-Z-E, and 35 minutes of aerobic exercise activities and fitness games. Specifically, the first letter “E” stands for jumping twice, the “N” for clapping three times, the second “E” for five jumping jacks, the “R” for jogging in place for 30 seconds, the “G” for clapping and jumping simultaneously four times, the “I” for sitting down and taking three deep breaths, the “Z” for standing up straight, and the last “E” for five sit-ups. Fitness games include topics such as “Fruit Flies,” “On the Bank, in the River,” “Cha-Cha Slides,” “Funky Monkey,” “Tales,” and “Mingle-Mingle.” Detailed information about the Energize curriculum is published online by the Monroe County YMCA [18].
Mind-body exercise (Health Qigong in particular) was chosen as another intervention. According to Creps, Health Qigong is described as a combination of Yoga and Tai Chi regarding its practice, which features a meditative body movement by imitating interesting plants and animals, deep belly breathing, positive imagination, self-massage, and moving meditation [3]. A typical Health Qigong class usually started with a five minute warm-up of whole-body tapping and deep belly breathing, followed by 35 minutes of mindfulnessbased movements and a five-minute meditation in conclusion. These movements normally included “Blooming like a Sunflower,” “Growing like a Pine Tree,” “Flying likes a White Crane,” and “Resting like a Sleeping Lion.” Movements are normally practiced by using pictures, stories, imagination, songs, and teamwork activities. A detailed description of the mind-body exercise program utilized by these authors is published in a previous study [19].
General Physical Education (PE) activities were chosen as the third intervention because PE is required for students at both elementary schools. A typical physical education class consisted of running, softball, calisthenics, dodge ball, volleyball, capture-the-flag, and short relay races of approximately 100 yards. Most physical education activities are competitive and demand highly physical involvement to develop kinetic and motor skills.
Data collection and scoring
The pre-test data were collected in the second week of the spring semester, and the post-test was conducted the week immediately following the 16-week intervention. The STAIC-1 questionnaire was scored based on the scoring key for STAIC [16]. The Piers-Harris 2 survey was scored based on the AutoScore™ Form [20]. Also, students’ age, gender, race, height and weight, were recorded at baseline to provide basic demographic information.
Data analysis
Data were analyzed using the Statistical Package for Social Science (IBM Statistics SPSS 22). Frequencies and percentages were run on all categorical variables to check for extreme and inconsistent values. Descriptive statistics were calculated for all continuous variables to summarize basic demographic characteristics. Skewness, kurtosis, and Q-Q plots were used to evaluate normality of each outcome variable. Homogeneity of variance between groups was examined by box plots and Levene’s test.
Chi-square tests of independence and analysis of variance (ANOVA) were conducted to determine statistically significant differences in participants’ characteristics among the three exercise groups. A 2 X 3 repeated measures ANOVA was conducted to identify significant changes from pretest to posttest among the three exercise groups. The statistical significance was set at p<0.05.
If the interaction effect of time x exercise groups or the three exercise groups’ main effects were significant, a follow up pair-wise comparison was performed. For all effects, partial eta-squared (η2) values were reported as indexes of meaningfulness (small, partial η2=0.10; moderate, partial η2=0.30; large, partial η2=0.50) to demonstrate the strength of the effect.
Results
Participant Characteristics for STAIC-1 and Piers-Harris 2 at Baseline: Table 1
Table 1 Participant demographics for STAIC-1 and Piers-Harris 2.
| STAIC-1 |
Energize (n=38) |
Health Qigong (n=34) |
Physical education activities (n=29) |
| mean |
SD |
mean |
SD |
mean |
SD |
| Age, years |
9.7 |
0.5 |
9.2 |
0.6 |
9.1 |
0.6 |
| Height, cm |
141.4 |
7.5 |
139.2 |
8.4 |
139.5 |
7.6 |
| Weight, kg |
39.5 |
9 |
38.6 |
7.9 |
37 |
8.2 |
| Gender |
n |
% |
n |
% |
n |
% |
| Girls |
24 |
63 |
16 |
47 |
16 |
55 |
| Boys |
14 |
37 |
18 |
53 |
13 |
45 |
| Race |
| White |
35 |
92 |
28 |
82 |
20 |
90 |
| Others |
3 |
8 |
6 |
18 |
3 |
10 |
| Piers-Harris 2 |
Energize (n=30) |
Health Qigong (n=27) |
Physical education Activities (n=11) |
| mean |
SD |
mean |
SD |
mean |
SD |
| Age, years |
9.8 |
0.5 |
9.1 |
0.6 |
8.8 |
0.4 |
| Height, cm |
140.3 |
7.1 |
137.7 |
7 |
137.4 |
7.8 |
| Weight, kg |
39 |
8.5 |
37.5 |
7.7 |
36.4 |
7.8 |
| Gender |
n |
% |
n |
% |
n |
% |
| Girls |
18 |
60 |
14 |
52 |
7 |
64 |
| Boys |
12 |
40 |
13 |
48 |
4 |
36 |
| Race |
| White |
27 |
90 |
23 |
85 |
10 |
91 |
| Others |
3 |
10 |
4 |
15 |
1 |
9 |
Note: STAIC-1: State-Trait Anxiety Inventory for Children S-Anxiety Scale; Piers-Harris 2: Piers-Harris Children’s Self-Concept Scale 2nd Edition
After removing extreme and inconsistent values, the sample size for the STAIC-1 was 101, composed of 56 females and 45 males. The average age was 9.4 years old. The majority of students (88.2%) were white.
Ninety students completed the Piers-Harris 2 questionnaire. Observations deviating more than two standard deviations from the mean were considered as possible outliers according to the Piers-Harris 2 manual. With the elimination of these extremely low or high scores, the sample size was 68, which consisted of 39 females and 29 males. The average age was 9.3 years old. The majority of students (88.2%) were white.
There were no significant differences for gender (P=0.390) or race (P=0.158) between the three groups. Additionally, no significant differences were observed for either STAIC-1 (P=0.134) or Piers-Harris 2 (P=0.588) between the three groups at pretest.
Results of the repeated measure analysis for STAIC-1 and Piers-Harris 2: Table 2
Table 2 Repeated measures analysis for STAIC-1 and Piers-Harris 2 from pre-to post-test among three exercise groups.
| |
F |
P-value |
η2 |
| STAIC-1 (N=101) |
| Time*Exercise |
0.17 |
0.85 |
0.003 |
| Time |
7.9 |
0.006** |
0.075 |
| Exercise Groups |
2.84 |
0.064 |
0.055 |
| Piers-Harris 2 (N=68) |
| Time*Exercise |
1.5 |
0.23 |
0.044 |
| Time |
16.87 |
<0.001*** |
0.206 |
| Exercise Groups |
1.29 |
0.283 |
0.038 |
Note. STAIC-1: State-Trait Anxiety Inventory for Children S-Anxiety Scale; Piers-Harris 2: Piers-Harris Children’s Self-Concept Scale 2nd Edition. **P<0.01, ***P<0.001
There was neither a significant difference in STAIC-1 as a function of exercise conditions (F (2, 98)=2.84, P=0.064, η2=0.055, 1− β=0.55), nor a significant interaction with exercise conditions by time (F (2, 98)=0.17, P=0.85, η2=0.003, 1-β=0.075). However, a significant main effect of stress reduction over the 16-week intervention period was found (F (1, 98)=7.9, P=0.006, η2=0.075, 1− β=0.8).
Similarly, for Piers-Harris 2, neither a significant difference among the three exercise groups (F (2, 65)=1.29, P=0.283, η2=0.038, 1− β=0.269), nor a significant interaction for exercise conditions by time (F (2, 65)=1.50, P=0.230, η2=0.044, 1− β=0.309) were found. A significant improvement on selfesteem total score over the intervention period was identified (F (1, 65)=16.87, P<0.001, η2=0.206, 1− β=0.982).
No post-hoc pair-wise comparisons were conducted since neither significant interaction effect from pre to post-test among the three exercise groups nor significant group, main effects were found for all three dependent variables.
Discussion
This study examines the relative effects of three modes of exercise in improving children’s psychological health. The findings show a significant reduction (P=0.006) in stress and improvement in self-esteem (P<0.001) over a 16-week intervention period among all three exercise groups, including Health Qigong, aerobic exercise, and physical education activities, which indicates that all exercises are beneficial for improving children’s psychological health.
This finding that conventional Western exercises (e.g., aerobic exercise and physical education activities) are beneficial for improving children’s psychological well-being is consistent with previous studies [21]. Regular exercise can stimulate positive thoughts and feelings by the increases in serotonin, dopamine, and endorphin [22,23]. This theory is also applied to Health Qigong because much literature has indicated that Health Qigong can be considered as a moderateintensity exercise in terms of its practice as a combination of Yoga and Tai Chi [3]. Furthermore, the psychological benefits of Health Qigong may also be due to the emphasis on deep belly breathing, positive imagination, self-massage, and meditative movement, which can induce relaxation response by stimulating the parasympathetic pulmonary neural receptors and enhance self-esteem by imitating interesting plants and animals through active and joyful group activities [19,24,25].
No significant differences were identified for either STAIC-1 (P=0.064) or Piers-Harris 2 (P=0.283) among the exercise groups. The failure to identify significant differences between aerobic exercise and mind-body exercise was not atypical in the field of pediatric psychological health. This may stem from insufficient frequency and duration of the interventions. Health Qigong teachers generally recommend daily practice of the exercise for at least six months to achieve substantial benefits. A similar study which demonstrated significant differences in stress reduction between Yoga and swimming suggested 40 minutes of instruction two days a week for 14 weeks [26]. Another similar study comparing the benefits between Tai Chi and brisk walking in improving quality of life suggested one hour three times per week for 12 weeks identifying a significant difference [27]. Although the present study followed the suggestion of teaching Health Qigong for more than nine weeks, the frequency of the Health Qugong classes may not have been sufficient to manifest obvious measurable advantages over aerobic exercise or regular physical education activities. In addition, the relatively small and unequal sample size can contribute to a low power to identify significant main effect for the three exercise modalities (when not superseded by a significant interaction effect) [28]. While this is appropriate for a pilot study, it may have caused some type 2 errors. Thus, future studies involving larger sample size with a longer intervention period and more frequent practice is warranted in order to determine if these three exercise modes significantly impact psychological wellbeing differently.
There are a few limitations that must be addressed for this study. First, only two self-reported measures (STAIC-1 and Piers-Harris 2) were utilized which may not have been sensitive enough to capture all of the variables that may have changed. To obtain a thorough assessment of a child’s stress level and self-esteem, the STAIC-1 and Piers-Harris 2 findings should be integrated with other clinical data, such as interviews and professional consultations. In particular, several studies researching Qigong for stress reduction involved the measurement of physical bio-markers, such as urinary cortisol and plasma norepinephrine and epinephrine which provide a more objective measure for distinguishing the difference between the impact of Health Qigong and other exercise modalities [3,29]. Second, participation in the study groups was not randomized due to the logistics of using class units rather than individuals. Non-randomization increases the risk of selection bias. Third, the frequency of the intervention was only once a week due to the tight schedule of the elementary school, which may not be sufficient to manifest obvious measurement differences among the three modes of exercise. Lastly, the majority of the participants were white, which may reduce the generalizability of outcomes to other race/ethnic groups.
Conclusion
Our findings indicate that all three exercise modes, including Health Qigong, aerobic exercise, and physical education activities, are effective in improving children’s psychological well-being. Mind-body exercise may be considered as an alternative approach for children who may not enjoy competitive sports or not fit in well with conventional exercise activities. A longitudinal study with larger sample size is warranted to detect how different modes of exercise influence children's mental health status. Future studies should investigate the complimentary benefits of exercises from both Eastern and Western cultures to meet children’s diverse needs for different types of exercises.
22846
References
- Division of Health Interview Statistics National Center for Health Statistics. 2012 National Health Interview Survey Description 2013.
- Perou R, Bitsko RH, Blumberg SJ, Pastor P, Ghandour RM, et al. (2013) Mental health surveillance among children-United States, 2005–2011. MMWR Surveill Summ 62: 1-35.
- Creps M (2012) Students learning ancient Chinese blend of Yoga and Tai Chi in YMCA’s in-school energize program. The Bloomington Herald-Times.
- Dimech AS, Seiler R (2011) Extra-curricular sport participation: A potential buffer against social anxiety symptoms in primary school children. Psychol Sport Exerc 12: 347-354.
- Scully D, Kremer J, Meade MM, Graham R, Dudgeon K (1998) Physical exercise and psychological well-being: A critical review. British J Sports Medicine 32: 111-120.
- Ekeland E, Heian F, Hagen KB, Abbott JM, Nordheim L (2004) Exercise to improve self-esteem in children and young people. Cochrane Database of Systematic Reviews.
- Eime RM, Young JA, Harvey JT, Charity MJ, Payne WR (2013) A systematic review of the psychological and social benefits of participation in sport for children and adolescents: Informing development of a conceptual model of health through sport. Int J Behavioral Nutri Physical Activity 10: 98.
- Landry BW, Driscoll SW (2012) Physical activity in children and adolescents. PMR 4: 826-832.
- Kann L, Kinchen S, Shanklin SL, Flint KH, Kawkins J, et al. (2014) Youth risk behavior surveillance-United States, 2013. MMWR Surveill Summ 63: 1-168.
- Rasberry CN, Lee SM, Robin L, Laris B, Russell LA, et al. (2011) The association between school-based physical activity, including physical education and academic performance: a systematic review of the literature. Prevent Medicine 52: S10-S20.
- Clarke TC, Black LI, Stussman BJ, Barnes PM, Nahin RL (2015) Trends in the use of complementary health approaches among adults: United States, 2002–2012. National Health Stat Reports 79: 1-16.
- Birdee GS, Yeh GY, Wayne PM, Phillips RS, Davis RB, et al. (2009) Clinical applications of yoga for the pediatric population: A systematic review. Academic Pediatr 9: 212-220.
- Cole S (2004) Moving slow in a fast world: The rise of Tai chi in America. IDEA Fitness J 1: 101-103.
- Hagen I, Nayar (2014) US Yoga for children and young people’s mental health and well-being: research review and reflections on the mental health potentials of yoga. Front Psychiatry 5: 35.
- Ng BHP, Tsang HWH (2009) Establishing a health qigong protocol for rehabilitation of patients with copd including commentary by Norweg A and Spruit MA. Int J Therapy Rehabilitation 16: 25-33.
- Spielberger CD, Edwards CD (1973) STAIC preliminary manual for the State-Trait Anxiety Inventory for Children (" How I feel questionnaire"): Consulting Psychologists Press.
- Beck AT, Epstein N, Brown G, Steer RA (1988) An inventory for measuring clinical anxiety: psychometric properties. J Consulting Clin Psychol 56: 893.
- Wang C, Wroblewski N, Dickson S (2012) Energize: A childhood obesity prevention program. Monroe Couty YMCA, IN.
- Wang C, Seo DC, Geib RW (2017) Developing a mind-body exercise programme for stressed children. Health Educ J 76: 131-144.
- Piers EV (1977) The Piers-Harris children's self-concept scale: (The way i feel about myself). Counselor Recordings and Tests.
- Sexton H, Maere A, Dahl N (1989) Exercise intensity and reduction in neurotic symptoms: A controlled follow-up study. Acta Psychiatr Scand 80: 231-235.
- Berger BG, Motl RW (2000) Exercise and mood: A selective review and synthesis of research employing the profile of mood states. J App Sport Psychol 12: 69-92.
- Fu H, Yang X (2005) Scientific principles of exercise and fitness. Hong Kong: Commercial Press.
- Horowitz S (2009) Evidence-based health benefits of qigong. Alternative Complementary Therapies 15: 178-183.
- Jerath R, Edry JW, Barnes VA, Jerath V (2006) Physiology of long pranayamic breathing: Neural respiratory elements may provide a mechanism that explains how slow deep breathing shifts the autonomic nervous system. Medical Hypotheses 67: 566-571.
- Berger BG, Owen DR (1988) Stress reduction and mood enhancement in four exercise modes: Swimming, body conditioning, Hatha yoga, and fencing. Res Quarterly Exercise Sport 59: 148-159.
- Audette JF, Jin YS, Newcomer R, Stein L, Duncan G, et al. (2006) Tai Chi versus brisk walking in elderly women. Age Ageing 35: 388-393.
- Kjos V, Etnier JL (2006) Pilot study comparing physical and psychological responses in medical Qigong and walking. J Aging Physical Activity 14: 241-253.
- Cheung BMY, Lo JLF, Fong DYT, Chan MY, Wong SHT, et al. (2005) Randomised controlled trial of qigong in the treatment of mild essential hypertension. J Human Hypertens 19: 697-704.

