Keywords
Low back pain, psychological factors, social factors.
Introduction
Back disorders encompassa spectrum of condition, from those of acute onset and short duration of lifelong disorders, and include osteoarthritis, disc degeneration, osteoporosis, and common low back pain. Neck pain is an entity in and of itself. The prevalence of many of these disorders increases markedly with age, and many of the disorders are affected by lifestyle factors, such as obesity and certain types of physical activity. Although the economic and public health effects of back disorders and especially low back pain are enormous, epidemiologic research into the problem is in a formative stage, is the increasing number of older people throughout the world, the burden on the individual and society as a whole is expected to inctease dramatically. While not a disease, back pain is a major cause of disability, especially in areas where compensation systems take it into cognizance [1,2].
Low back pain (LBP) is usually defined as pain, muscule tension, or stiffness localized below the costal magrin and above the inferior gluteal folds, with or without leg pain (sciatica) [1]. LPB is a major health problem around the world which accounts for considerable socioeconomic and health care burden [2].
The life time incidence of LBP has been reported between 60-80 %, [3,4] and out of these incidents in about 80-90% cases pain subsides within first 2-3 months rest of the patients (around 10-20%) develop chronic pain syndromes [5]. Chronic low back pain patients comprises 73-77% of all the patients with lower back pain disorders [6,7]. Approximately 90% of cases of back pain have no identifiable cause and are designated as nonspecific. Many doctors order elaborate studies when nonspecific back pain is presented, including radiographs and magnetic resonance imaging. The results are little guidance to treatment decisions. Inconsistencies remain in the literature over the relative contributions of physical and psychological risk factors to the occurence of back disorders and back pain. Relatively little is known about risk factors for the transition from acute to chronic LBP can be classified as individual, psychosocial, or occupational factors (Table 1) [1].
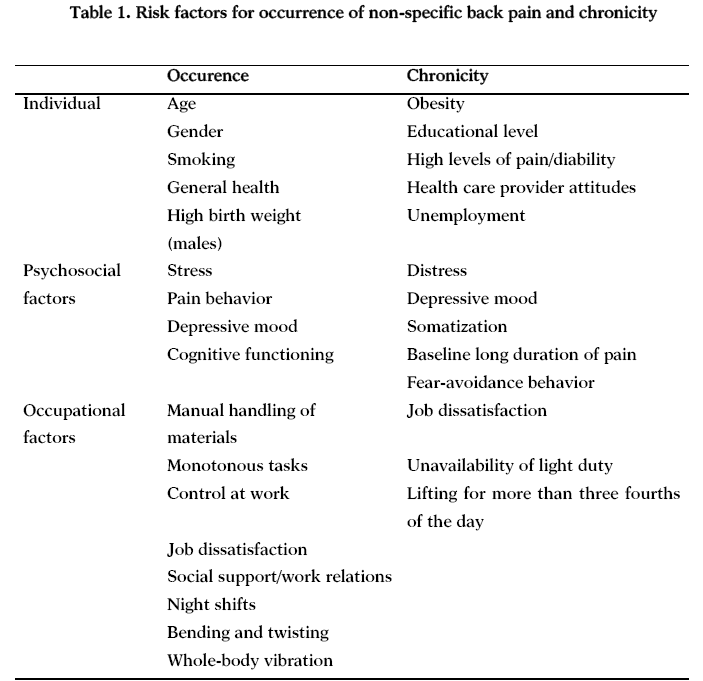
The presence and severity of LBP is associated with several socio-demographic factors, among them sex, age, education level, smoking, and occupation [8-10]. Studies on the association between occupational risk factors and low back pain are hampered by the difficulties of measuring specific exposures. Many studies are limited by the absence of more quantitative measurements of manual material handling task parameters, and risk of low back injury may be entirely a result of the design of the workplace as opposed to individual differences among the workers [11]. Occupational factors be able to defined as workplace factors and others. Workplace factors including physical and psychosocial factors and their interaction, are strong determinants of back pain. Other factors such as heavy physical work, night shifts, lifting, bending, twisting, pulling, and pushing have often been associated with low back pain [10,12]. Psychological variables associated with low back include stress, distress, mood and emotions, cognitive functioning, pain behavior, and depressive disorder [13]. Numerous studies have explored and have identified associations between psychological factors or social factors or social factors and low back pain. These associations ocur before the fact, i.e. in subjects who have yet to develop back pain, and after the fact, i.e. in patients who have developed back pain [14]. The many publications occupational LBP and have examined risk factors, it is the most expensive source of compensated work related injury in modern in dust rialised countries. Moreover, both the rate and the degree of disability accruing from LBP are increasing worldwide [15]. Epidemiologic studies provide some support that psychosocial factors in the work enviroment are in fact related to LBP. The aim of this paper was to provide and review of the impact of physical, psychosocial factors, and psychological stres on occupational LBP.
Occupational risk factors for low back pain
Musculoskeletal pain, in particular LBP, is one of the most common occupational health problems and accounts for a large number of workers’ compensation days and disability in modern industriablised societies. LBP has been found to affect more workers and result in higher costs to industry than any other musculoskeletal disorders. Traditionally, the most widely investigated occupational risk factors for LBP have been biomechanical demands of the job. In more recent years, psychosocial characteristics of work have been investigated as potential risk factors for LBP. Each of these approaches has provided some evidence about the complex relationship among work tasks, work placeenviroment, and LBP. A conceptual model of the potential relationships among psychosocial work characteristics, biomedical work demands, and LBP is presented in Fig 1.
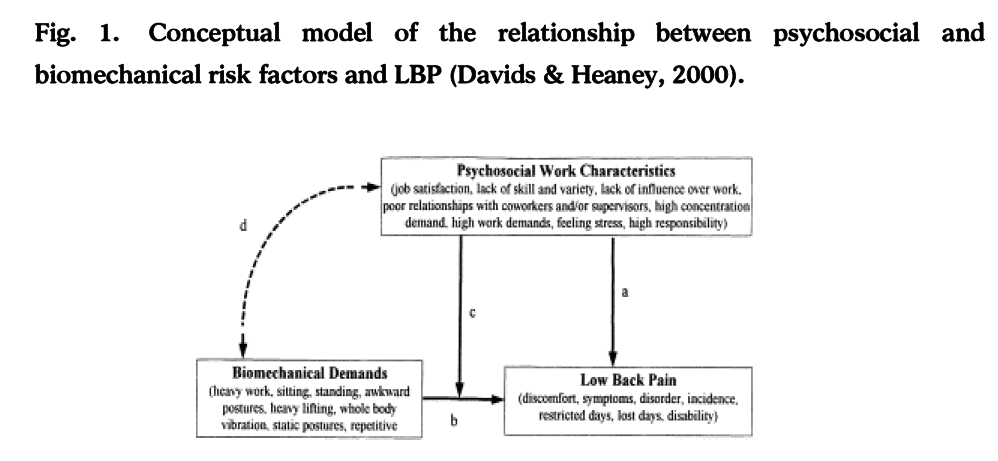
Figure 1: Conceptual model of the relationship between psychosocial and biomechanical risk factors and LBP (Davids & Heaney, 2000).
Psychosocial factors (see pathway a) and biomechanical factors (see pathway b) may independently contribute to the etiology and progression of LBP. Psychosocial factors may also influence the relationship between biomechanical factors and LBP (see pathway c), such that biomechanical demands have a greater effect on LBP under poor psychosocial work conditions. Additionally, poor psychosocial work characteristics and high biomechanical demands may covary (e.g., tend to concentrate in smilar jobs and occupations). This covariation (see pathway a) raises the possibility of confounding if both types of risk factors are not accounted for in risk models. Until fairly recently, biomechanical demands and psychosocial work characteristics were rarely investigated as risk factors for LBP within the same study [16].
The association of physical and nonphysical factors with occupational low back pain
The association of nonphysical factors with LBP has been one of the more robust findings in the literature seporting factors associated with LBP. Two factors, psychological state and aspects of work satisfaction, have been the main focus of research. LBP has been consistently associated with neurotic signs such as depression, anxiety, and heightened somatic awareness in LBP sufferers drawn from patient populations. While several studies have suggested similar associations between psychological factors and LBP in nonpatient populations, the findings have not been consistent. Aspects of the work enviroment and work satisfaction have also been found to be associated with LBP in industrial and general popultion studies. Several studies have reported that sufferers of LBP and back injury claimants are more likely to be dissatisfied with their jobs, attract poor appraisal from supervisors, and be more likely to experience a poor psychosocial work enviroment, but contradictory findings have also been reported [15]. Its believed that occupational LBP is caused by multiple factors, generally categorised into biomechanical and psychosocial approaches.
The biomechanical approach has been based on the premise that physical aspects of the job contribute to LBP. Biomechanical factors have been hypothesized to cause LBP through two mechanisms: excessive load and repetitive loading on the spinal structures. Excessive loads can result from lifting heavy loads, awkward postures, and high trunk velocities while repetitive loading results from an evevated number of lifting cycles over long period time. Biomechanical factors such as lifting, awkward postures, static postures, repetitive trunk motions, whole-body vibration, and heavy loads have been found to be risk factors for LBP. Loads on the spine that accompany the above risk factors have also been found to be moderately associated with LBP [16]. Psychosocial factors at work have also been shown to play important roles in the development of LBP. Important psychosocial factors included work demands and decision latitude, symptoms of stress, social support, type A behaviour, and psychological distress. After reviewing 59 relevant studies, Bonger et al., [17] concluded that monotonous work, high perceived workload, time pressure, low control on the job, lack of social support from colleagues, and stress symptoms were related to musculoskeletal problems. Carayon et al., [18] reviewed work organisation, job stress, and work related musculoskeletal disorders, and concluded that work organisation and psychosocial factors at work could contribute to upper extremity disorders. They further indicated that work organisation and ergonomic factors might interact to affect the musculoskeletal system. Chen et al., [19] explored the relation between psychosocial factors and musculoskeletal pain in Chinese offshore oil installation workers. According to results of this study, the prevalence of musculoskeletal pain over the previous 12 months varied between 7.5 % for elbow pain and 32 % for LBP; 56 % workers had at least one complaint significant associations were found between various psychosocial factors and musculoskeletal pain in different body regions after adjusting for potential confounding factors. Occupational stressors, in particular stres from safety, physical enviroment, and ergonomics, were importantnpredictors of musculoskeletal pain, as was coping by eating behaviour. Eating behaviour coping stkyes as eating, drinking alcol/tea/coffee, and smoking. Other coping styles, escaping/abreaction, external/social, and internal were also found to have an impact on pain in different body regions.
Psychosocial factors at work have also been shown to play important roles in the development of LBP. Gaffari et al., [20] tested the hypothesis that workplace psychosocial factors such as demand, control, support, job satisfaction and job appreciation can predict the future onset of disabling LBP in Iranian industrial workers. A total of 744 subjects reported current LBP, a total of 52 new episodes of disabling LBP were observed during the 1-year follow-up. Male employers reported higher demands, lower control and lower support than female employers.
There are many studies have evaluate prevalence, etiology and the association of sociodemographic variables with occupational low back pain in Turkey but there are limited number of studies have tested the relationship between psychosocial factors and occupational LBP. In a study examined the level of depression and quality of life and their relationship with severity of pain in chronic low back pain patients. According to researchers the depression level and the pain severity are closely related in patients with chronic low back pain. Pain severity and the level of depression negatively affected the life quality and functional capacity of the patients., [21] Demet et al., [22] investigated low back pain of housewives and determined relationships between psychological status, education and physical health in housewives. The results of this study were the housewives with chronic back pain and do not exercise regularly limit activities of daily living and, the housewives’ the level of depression were high. In another study determined if there was a relationship between smoking and low back pain. Researchers concluded that smoking is not a risk factor for low back pain [23]. In view of the risky physical demands and psychosocial features of police work, policemen are at risk for low back pain. Beyaz & Ketenci [24] investigated occupational low back pain and therapeutic approaches in policemen. Policemen reported causes of LBP; non-ergonomic and worn-out seats, poor physical integration, previous low back pain, the time spent in the vehicle, personal occupational heavy equipment such as duty belt, stress and occupation years. Low back pain is a common problem in textile industry workers. In another study investigated the prevalence and risk factors of self reported low back pain among textile workers. The study population consisted of 1153 factory workers of which 84.7% were males. Twenty eight percent of the workers experienced at least once low back pain during the last six months. The prevalence of mechanical low back pain was 7%. Being female, working more than ten years in textile industry, smoking and working in the office were the risk factors for self-reported low back pain, and making exercise regularly was a preventive factor. Workers who exercise regularly routine reported of low back pain [25-27]. Ozcan et al. [28] investigated the risk factors and the prevalence of occupational musculoskeletal pain in workers who working at metal work. The prevalence of musculoskeletal pain 83.0% in the last 12-months. The prevalence of complaints of pain in the last 12-months, 64.8% low back, 52.9% back, neck 48.0%. The risk factors of occupational musculoskeletal pain have been found that 20 kg load lifting, load-pulling, load-carrying. Occupational LBP is a very common complaint in the health care professionals. In a study determined the prevalence of occupational LBP, the association of personal and work related factors with occupational LBP in health care workers at the university hospitals. The results of this study were yearly back pain prevalence was 34.3% and chronic low back pain prevalence was 16%. Positive family history and smoking were found to be related to an increased risk of low back pain. Sex, weight, race, social status, history of pregnancy or sports activities and daily living activities were not found to be related to low back pain [29]. Yilmaz & Ozkan [30] determined the prevalence of LBP in nurses who working at the public hospitals. Researchers found that 39.9% of the nurses had experienced an episode of LBP and statistical correlation between LBP and working period, sleep regime and income level. In another study described musculoskeletal problems resulting from work setting and occupation in medical doctors who work in a hospital. Researchers established that 41 of 123 subjects had at least one musculoskeletal problem resulting from work setting and working so long time with the same position and repiting the same activities during wok day lead to a risk factor about musculoskeletal problems in medical doctor [31].
Conclusion
Although there are enough studies related to effect of psychosocial factors on occupational LBP in our country, psychosocial factors play an important role in low back pain is now well documented and generally accepted. A person' ability to recover may be determined by such things as motivation, ambitions, social support, attitude at work and family dynamics. The development of occupational LBP are effective physical factors as well as psychosocial factors. According to findings of review studies may be suggested that occupational LBP may be improved by management of psychological distress, provide of social support, develop of positive coping styles, evaluate of depression, burnout, job satisfaction.
3156
References
- Manek NJ, MacGregor AJ. Epidemiology of back disorders:prevalence, risk factors, and prognosis. Curr Opin Rheumatol. 2005; 17:134-140.
- Maniadakis N, Gray A. The economic burden of back pain in the UK. Pain. 2000; 84: 95-103.
- Twomey LT, Taylor JR. Physical Therapy of the Low Back. 3rd ed. London, UK: Churchill Livingstone, 2002.
- O’Sullivan P. Diagnosis and classification of chronic low back pain disorders: Maladaptive movement and motor control impairments as underlying mechanism. Manual Therapy. 2005; 10: 242–255.
- Carey TS, Garrett JM, Jackman AML. Beyond the good prognosis: Examination of an inception cohort of patients with chronic low back pain. Spine. 2000; 25(1)115-120.
- Indahl A, Velund L, Reikeraas O. Good prognosis for low back pain when left untampered. Spine. 1995; 20(4): 473-477.
- Coste J, Delecoeuillerie G. Clinical course and prognostic factors in acute low back pain: an inception cohort study in primary care practice. BMJ.1994; 308 (6928): 577-580.
- Stranjalis G, Tsamandouraki K, Sakas DE, Alamanos Y. Low back pain in a representative sample of Greek population: analysis according to personal and socioeconomic characteristics. Spine. 2004; 29:1355-60.
- Raspe H, Matthis C, Croft P, O’Neill T. Variation in back pain between countries: the example of Britain and Germany. Spine. 2004; 29:1017-21.
- Kaila-Kangas L, Kivimäki M, Riihimäki H, Luukkonen R, Kirjonen J, Leino-Arjas P. Psychosocial factors at work as predictors of hospitalization for back disorders: a 28-year follow-up of industrial employees. Spine. 2004; 29:1823-30.
- Ferguson SA, Marras WS, Burr DL. The influence of individual low backhealth status on workplace trunk kinematics and risk of low back disorder. Ergonomics. 2004; 47:1226-37.
- Eriksen W, Bruusgaard D, Knardahl S. Work factors as predictors of intense or disabling low back pain; a prospective study of nurses’ aides. Occup Environ Med. 2004; 61:398-404.
- Turk DC, Okifuji A. Psychological factors in chronic pain: evolution and revolution. J Consult Clin Psychol. 2002;70(3):678-90.
- Bogduk N. Psychology and low back pain. International Journal of Osteopathic Medicine.2006; 9:49-53.
- Feyer A, Herbison P, Williamson A, de Silva I, Mandryk J, Hendrie L, et al. The role of physical and psychological factors in occupational low back pain:a prospective cohort study. Occup Environ Med. 2000; 57:116-120.
- Davids KG, Heaney CA. The relationship between psychosocial work characteristics and low back pain:underlying methodological issues. Clinical Biomechanics. 2000; 15:389-406.
- Bongers PM, de Winter CR, Kompier MA, Hildebrandt VH. Psychosocial factors at work and musculoskeletal disease. Scand J Work Environ Health. 1993;19:297-312.
- Carayon P, Smith MJ, Haims MC. Effect of psychosocial factors on low back pain in industrial workers. Occupational Medicine. 2008;58:341-47.
- Chen WQ, Yu T-S, Wong TW. Impact of occupational stres and other psychosocial factors on musculoskeletal pain among Chine offshore oil installation workers. Occup Environ Med.2005; 62:251-56.
- Ghaffari M, Alipour A, Farshad AA, Jensen I, Josephson M, Vingard E. Effect of phychosocial factors on low back pain in industrial workers. Occupational Medicine. 2008; 58:341-47.
- Gonge H, Jensen DL, Bonde JP. Are psychosocial factors associated with low-back pain among nursing personel? Work&Stres. 2002; 16(1):79-87.
- Derebery JV, Tullis WH. Low back pain exacerbated by psychosocial factors. West J Med. 1986;144:574-9.
- Ay S, Evcik D. Depression and quality of life in chronic low back pain [In Turkish] Yeni Tip Dergisi. 2008;25:228-31.
- Ucar D, Bozkurt M, Ucar BY, Bulut M, Azboy I. Chronic low back pain in housewives. Klinik ve Deneysel Arastirmalar Dergisi. 2011;2(3):295-98. [Article In Turkish]
- Albayrak I, Sahin N, Karahan AY, Ugurlu H. The relation of smoking with low back pain. Genel Tip Derg. 2010;20(2):55-9. [Article In Turkish]
- Beyaz EA, Ketenci A. Low back pain in policemen. [In Turkish] Agri. 2010;22(1):1-6.
- Bakirci N, Torun SD, Sulku M, Alptekin K. Mechanic low back pain among the workers in three textile factories in İstanbul. Toplum Hekimligi Bulteni. 2007;26(2):10-15. [Article In Turkish]
- Ozcan E, Alptekın K, Uysal B, Teksöz B, Issever H, Ozcan EE. Physical risk factors for musculoskeletal complaints among metal workers. International Occupational. Health and Safety Regional Conference. November 01-03,2008, Istanbul, Turkey.
- Altınel L, Kose CK, Altinel EC. Prevalence of back pain and pain related factors in professional health care workers. Tip Arastirmalari Dergisi. 2007;5(3):115-20. [Article In Turkish]
- Yilmaz E, Ozkan S. Determination of the prevalence of low back pain among nurses working in hospitals Turk J Phy Med Rehab. 2008;54:8-12.
- Buker N, Aslan E, Altug F, Cavlak U. An analysis study of musculoskeletal problems in medical doctors. Dumlupinar Universitesi Fen Bilimleri Enstitusu. 2006;10:163-70. [Article In Turkish]

