Keywords
Doctors, physicians, attitudes, attempted suicide, parasuicide, self-poisoning.
Introduction
Colon cancer is the third most common cancer in both genders in USA and a leading cause of death from cancers [1]. According to American Cancer Society an estimated of 101.340 cases of colon cancer and an estimated 49.389 deaths from colorectal cancer are expected to occur until the end of this year [2]. In Europe despite the progress of both conservative and surgical forms of treatment for advanced carcinomas the mortality rate is remained high. Greece is one of the countries with the lowest number of cases of colon cancer in Europe [3].
Depression is the most frequently cancer related symptom and is a comorbid disabling syndrome that affects approximately 15-25% of cancer patients [4]. Presence of depression produces complications in treatment and can lead to poor compliance with treatment resulting in worsening the situation [5]. Patients with colon cancer report serious psychological and emotional morbidities [6,7].
Various studies have shown high levels of depression in cancer patients using different methods of assessment [8,9,10]. It is reported that depression in cancer patients may be caused by diagnosis of cancer, long duration of treatment, side effects of treatment, disruption in life and diminished quality of life [8,10]. It is highly associated with oropharygheal, pancreatic, breast and lung cancers and is reported a less high prevalence of depression in patients with other cancers such as colon, gynecological and lymphoma [11].
Depression in gastrointestinal cancer patients has been examined in some studies. Nordin et al., [12] have shown that the levels of anxiety and depression at diagnosis could predict a similar status 6 months later and found that patients’ satisfaction with life is associated with depression. Similar results reported one Turkish study in which 23,6% of patients were determined as depressive and depression was strongly associated with poor quality of life [13]. Depression has also a stronger impact on the global quality of life of patients in a study of Tsunoda [14].
According to other studies depression increased from before surgery to before discharge and did not return to presurgery at 6 months after discharge [15,17]. Depression is more common in middle age patients, in patients undergoing chemotherapy and in those who experience long term hospitalization [15]. In another study it was also confirmed that patients after surgical resection treated with chemotherapy appear mild or moderate depression when compared to patients without indication of chemotherapy. In the same study it was also supported that there was no correlation between the inventories and site of tumor or stage [17]. According to another study 57% of gastrointestinal cancer patients scored high level of depression and there were no significant differences in depression between gender, educational level, marital status and cancer site [18].
In Greece, depression has been assessed in cancer patients, [19] in patients undergoing chemotherapy, [20] in advanced cancer patients [10] and in breast cancer survivors [21] and it is known from ancient years [22]. All these studies assessed depression with different assessment tools but not with CES-Depression scale. The present study seeks to investigate this symptom in Greek colon cancer patients. It is anticipated that the findings of the study can be used to alleviate it in clinical settings through future nursing interventions.
Aim
The aim of the present study was to explore the frequency of depression’s occurrence in colon cancer patients and to evaluate possible factors that affect the whole situation.
Methods
Sample and setting
The study was non experimental and descriptive in design. The convenience sample consisted of 79 patients in two hospitals in Northern Greece. Patients were eligible to participate in the study if they had histological confirmed colorectal cancer, were undergoing colectomy, were not receiving concomitant radiotherapy or chemotherapy and were mentally able to speak and read the Greek language.
Procedure
The study protocol was approved by the hospitals’ authorities and a permission to carry out the research was sought from them. Potential subjects were approached by one member of the research team. The study aims were explained and patients were asked whether they were willing to participate. An informed consent was obtained from those who agreed to participate. Patients completed the questionnaire in a quiet, private room in each hospital. A total of 90 patients were invited and 79 agreed to participate in the study (87%).
Instrument
Subjects were assessed for their level of depression using the Center for Epidemiologic Studies Depression Scale (CES-D). The CES-D is a 20-item, self report scale developed by Radloff (1977) [23]. It is a well-known and widely used scale for the measurement of depression [24]. Respondents indicated how often they have experienced a variety of symptoms during the past week on a four-point Likert scale ranging from 0 (rarely or none of the time) to 3 (most or all of the time). Higher scores indicate higher levels of depression. Scores range from 0-60. A score of 16 which is a cut -off point or above and it is accepted to be a symptom of clinical depression [25,26]. The instrument is a reliable measure of depression as demonstrated by other studies in cancer patients [26]. The Cronbach’s a coefficient for this sample is 0, 87 and as such satisfactory reliability is indicated.
Data analysis
The statistical software SPSS 13 was used to analyze the data. Descriptive statistics were used for demographic characteristics. The data were normally distributed so parametric tests were used. In order to explore the factors that are independently associated with the depression, linear regression analyses were performed with a stepwise method. All p values reported are two-tailed. Statistical significance was set at 0.05
Results
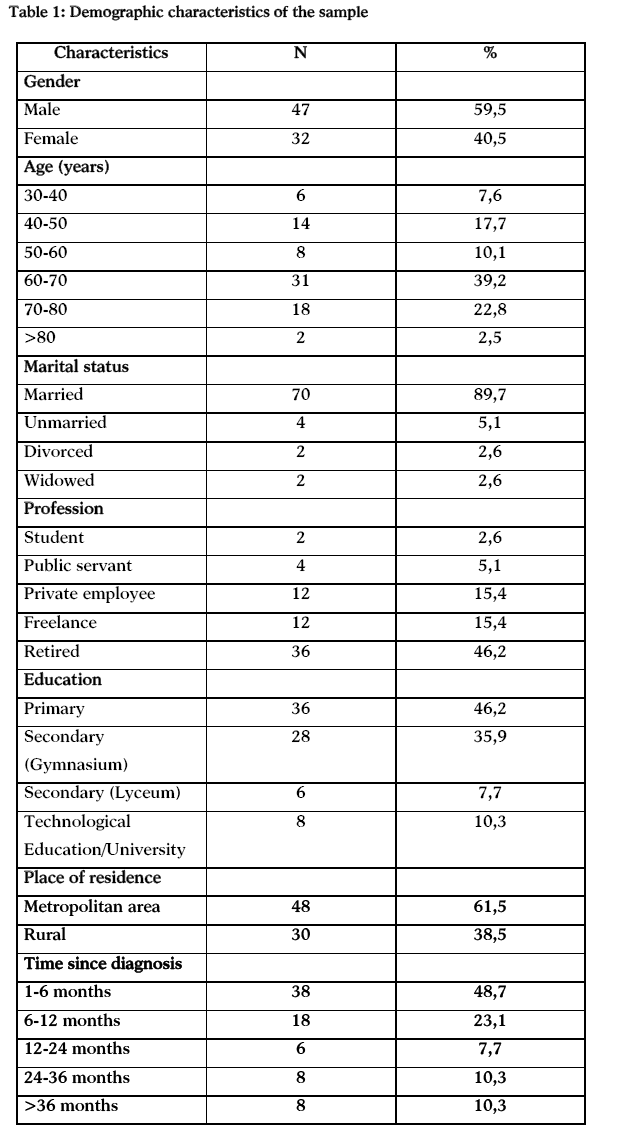
The sample of the present study consisted of 79 patients with a mean age of 60,34 ±13,39 (range 30-88). A percentage of 59,5% (n=47) of patients were male and only 40,5% (n=32) were female. Most of the patients (49,3%) were between 50 and 69 years, were married (89,7%), had received only basic education (46,2%) and 46,2% were retired. In terms of patients residency 61,5% were living in the region of metropolitan area and 38,5% were living in the country side. The results are shown in table 1.
Analysis of data showed that 30,4% of patients scored in CES-D scale lower than 16 indicating absence of depression and 69,4% scored higher than 16 indicating a symptom of clinical depression so they could be considered as depressive.
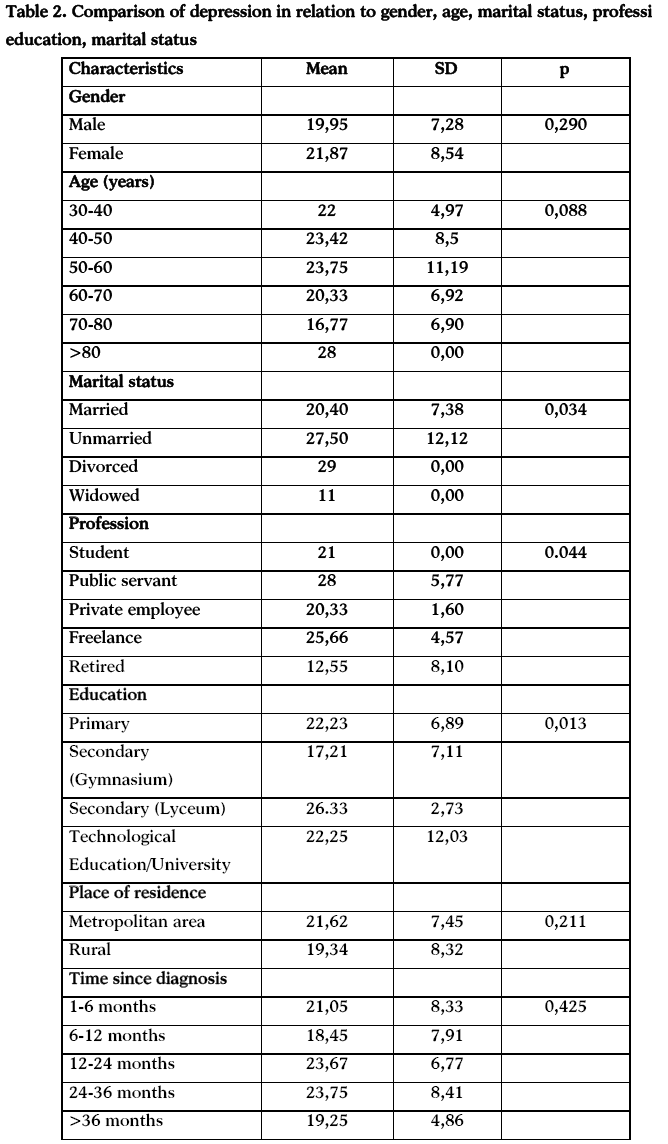
It was found that regarding patient’s gender, women and men experience the same level of depression (p=0,290) and also there was not statistically difference in depression between age groups (p=0,088). Higher levels of depression were observed for public servants patients (p=0,044) compared to patients who had other professions. Family status and depression also showed a significant difference (p=0,034) indicating that divorced patients experienced higher levels of depression compared to married and unmarried patients.
In addition, there was a statistically significant difference between educational status of patients and depression. The results indicated that those who had received secondary education had a significant higher level of depression (p=0,013) than others. Considering patients’ place residence and time since diagnosis, the findings showed that there were no statistically significant differences (p=0,211 and p=0,425 respectively). The results are shown in table 2.
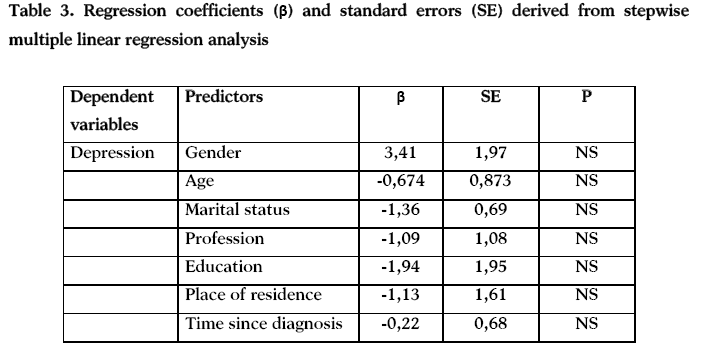
For determining what factors influence depression a multiple linear regression analysis was conducted. When multiple linear regression analysis was conducted (Table 3), with the score for depression as the dependent variable, it was not found statistically significant independent predictors.
Discussion
The present study assessed the symptom of depression in Greek patients with colon cancer. It contributes to the growing body of evidence regarding depression. It is anticipated that the findings of the study can be used by the Greek oncology nurses in order to ameliorate the nursing interventions in the clinical setting in the future.
The majority of the participants were men and this is a similar finding with other studies [18,27]. A percentage of 49,3% were between 50-69 years and this is an expected outcome because in Greece there is aged population according to National Statistical Agency.
The findings of our study indicated that 69,4% of colon cancer patients had depression while in other studies the prevalence of depression spectrum ranging from 23,6% -31,6% in colorectal cancer patients [13,17]. These differences could be attributed to different study design, sample characteristics and the different assessment methods used by the other studies.
An interesting finding of our study is that there was not statistically difference between depression and gender as well as between depression and age. This is consistent with the findings of other studies [17]. Depression is also believed that affects men and women with cancer equally and gender related differences in prevalence and severity have not been adequately evaluated [28]. In addition, there are conflicting results about depression and age and gender in other studies [11].
In regard to educational status, patients of secondary education experienced higher level of depression compared to those of primary education. This result is consisted with a finding of another Greek study in which it is supported that “the patients of low educational status are frequently unwilling to report their depressive symptom” [20].
Another interesting finding is about the marital status of patients. It is found that divorced patients experience higher level of depression in comparison with married ones. A possible explanation about this is that these people have no emotional support by their family, so it is easier to be depressive. This result is inconsistent with the results of other studies that found there was no statistical difference between depression and marital status [8]. Regarding the profession, there is a difference between our results and the results of other studies [8]. This difference may be explained by the fact that the other studies had different methodological design; larger population studied and had examined different types of cancer. Further research is needed in Greece in order to clarify the variables that affect the depression in colon cancer patients. In multiple regression analysis, our results have shown that the examined variable did not predict depression. This is not consistent with the study of Jadoon et al., [8] in which it was shown that the age (up to 40 years) has significantly influenced the prevalence of depression in cancer patients. A possible explanation for this difference is that the study of Jadoon examined all types of cancer and had a large number of participants. Culture may also had a significant role as it is reported that culture background affects the emotional expression of depression [29].
Another important factor that influenced the depression, but it wasn’t evaluated in the present study is the quality of life. There are some studies that have examined the relation between quality of life and depression [13,14,30] and it was shown that depression was strongly associated with poor quality of life13 and also with the symptom of distress for the malaise. Nutritional and gastrointestinal factors were independent predictors of depression [30]. Further studies on this topic would be needed in Greece.
Limitations of the study
This study has several limitations. First of all, our data provided limited clinical information and did not permit further description and correlation between depression and clinical characteristics of the sample. Secondly, our study includes a small number of cases thereby limiting the ability to generalize the findings to the entire Greek population.
Conclusions
This study shows that colon cancer patients have high prevalence rate of depression. More research is required to determine the patterns of depression during treatment and to correlate the clinical characteristics with the depression symptom in Greece. The findings are interesting for nurses, as they can detect cancer patients at high risk for depression. The results can also help them to the implementation of appropriate nursing interventions. Nurses should also cooperate with psychologists and this could lead to the improvement of the disease’s outcome and to the quality of patients’ life.
3129
References
- Mantzaris GJ. Clinical and epidemiological data on colorectal cancer, inflammatory bowel disease and helicobacter pylori in Greece. Annals of Gastroenterology. 2002; 15(4):374-380.
- Cancer Facts &Figures 2011. available at https://www.cancer.org. access in 8 August 2011.
- Classen M, Lambert R. International Digestive Cancer Alliance. Colorectal cancer screening in europe--a survey of the International Digestive Cancer Alliance. between November 2004 and March 2007.Z Gastroenterol. 2008;46( Suppl 1) :S23-4.
- National Cancer Institute. Depression available at https://www.cancer.gov access in 8 August 2011.
- O’Mahony S, Goulet J, Kornblith A, Abbatiello G, Clarke B, Kless-Siegel S, et al. Desire for hastened death, cancer pain and depression: report of a longitudinal observational study. J Pain Symptom Manage. 2005; 29: 446-57.
- Fillipovic BR, Fillipovic BF, kerkez M, Millnic N, Randelovic T. Depression and anxiety levels in therapy –nivepatientsith inflammatory bowel disease and cancer of the colon. World J Gastroenterol. 2007; 13(3): 438-443.
- Ashbury FD, Madlensky L, Raich P, Thompson M, Whitney G, Hotz K, et al. Antidepressant prescribing in community cancer cre. Support Care Cancer. 2003; 11: 278-285.
- Jadoon NA, Munir W, Shahzad MA, Choudhy ZS. Assessment of depression and anxiety in adult cancer outpatients : a cross-sectional study. BMC Cancer. 2010; 10:594.
- Pirl WF. Evidence report on the occurrence, assessment, and treatment of depression in cancer patients. J Natl Cancer InstMonogr. 2004, 32:32-9.
- Mystakidou K, Tsilika E, Parpa E, Katsouda E, Galanos A, Vlahos L. Assessment of anxiety and depression in advanced cancer patients and their relationship with quality of life. Qual Life Res. 2005, 14:1825-33.
- Massie MJ: Prevalence of depression in patients with cancer. J Natl Cancer InstMonogr. 2004, 32:57-71.
- Nordin K, Wasteson E, Hoffman K, Glimellius B, SjodenPO.Discrepancies between attainment and importance of life values and anxiety and depression in gastrointestinal cancer patients and their spouses. Psychooncology. 2001; 10(6):479-489.
- Alacacloglou A, Binicier O, Gugnor O, Oztop I, Dinoz M, Yilmaz U. Quality of life, anxiety, and depression in Turkish colorectal cancer patients. Support Care Cancer. 2010; 18(4):417-421.
- Tsunoda A, Nakao K, Hiratsuka K, Yasuda N, Shibusawa M, Kusano M. Anxiety, depression and quality of life in colorectal cancer patients. Int J Clin Oncology. 2005;10(6):411-417.
- Matsushita T, Matsushima E, Maruyama M. Psychological state, quality of life, and coping style in patients with digestive cancer. Gen Hosp Psychiatry. 2005; 27(2):125-132.
- Matsushita T, Matsushima E, Maruyama M. Anxiety and depression of patients with digestive cancer. Psychiatry ClinNeurosci. 2005; 59(5): 576-58.
- Medeiros M, Oshima CT, Forones NM. Depression and anxiety in colorectal cancer patients. J Gastrointest Cancer.2010;41(3):179-184.
- Tavoli A, Mohammad AM, Montazeri A, Roshan R, Tavoli Z, Omidvari S. Anxiety and depression in patients with gastrointestinal cancer: does knowledge of cancer diagnosis matter? BMC Gastroentelogy. 2007; 7:28.
- Mystakidou K, Parpa E, Tsilika E, Gogou P, Panagiotou I, Galanos A, et al. Self-efficacy, depression, and physical distress in males and females with cancer. Am J HospPalliat Care. 2010;27(8):518-525.
- Polikandroti M, Evaggelou E, Zerva S, Zerdila M, Koukoularis D, Kyritsi E. Evaluation of depression in patients undergoing chemotherapy. HSJ. 2008; 2(3):162-172.
- Fafouti M, Paparigopoulos T, Zervas Y, Rabavilas A, Malamos N, Liappas I, Tzavara C. Depression, anxiety and general psychopathology in breast cancer patients: a cross-sectional control study. In Vivo. 2010 ; 24(5):803-810.
- Kourkouta L. Ancient Greek psychotherapy for contemporary nurses. J PsychosocNursMent Health Serv. 2002; 40 (8):36-9.
- Radloff LS. The CES-D scale: A self report depression scale for research in the general population. Applied Psychological Measurement. 1977; 1:385-40.
- Fontoulakis K, Iacovides A, Kleanthous S, Samoli S, Kaprinis SG, Sitzoglou K, et al. Reliability, Validity and psychometric properties of the Greek Translation of the Center for epidemiological Studies. Depression (CES-D Scale). BMC Psychiatry. 2001;1:3.
- Bower JE, Ganz PA, Desmond KA, Bernaard C, Rowland JH, Meyerowitz BE, et al. Fatigue in long-term Breast Carcinoma Survivors. A longitudinal Investigation. Cancer. 2006; 106(4):751-758.
- Klemm P, Hardie T. Depression in internet and face-to face. Cancer Support Groups: A Pilot study. OncolNurs Forum. 2002;29(4):E45-E51.
- Smith-Gagen J, Cress RS, Drake CM, Romano PS, Yost MK, Ayanian JZ. Quality-of-Life and Surgical Treatments for Rectal Cancer-a Longitudinal Analysis Using the California Cancer Registry. Psychooncology. 2010; 19(8): 870–878.
- Miakowski C. Gender differences in pain, fatigue and depression in patients with cancer. J Natl Cancer InstMonogr. 2004; 32:139-143
- Bailey RK, Geyen DJ, Scott-Gurnell K, Hipolito MMS, Baley TA, Beal JM. Understanding and treating depression among cancer patients. Int Gynecol. Cancer. 2005;15:203-208.
- Breen SJ, Baravelli CM, Schofield PE, Jefford M, Yates PM, Aranda SK. Is symptom burden a predictor of anxiety and depression in patients with cancer about to commence chemotherapy? Med J Aust. 2009; 190(7 Suppl):S99-104.

