Amal Elbadri, Ibrahim Kheiri and Abdelmula Mohamed Abdalla*
Department of Clinical Chemistry, Faculty of Medical Laboratory Sciences, Alneelien University – Khartoum, Sudan
*Corresponding Author:
Abdelmula Mohamed Abdalla
Department of Clinical Chemistry
Faculty of Medical Laboratory Sciences
Alneelien University – Khartoum, Sudan
Tel: 00249912608616
E-mail: mula200099@yahoo.co.uk
Received date: 30 November 2018; Accepted date: 17 December 2018; Published date: 24 December 2018
Citation: Elbadri A, Kheiri I, Abdalla AM (2018) Evaluation of Serum Zinc Level Sudanese Patients of Erythropoietin Resistant In Hemodialysis. Health Sci J Vol.12.No.6:613. DOI: 10.21767/1791-809X.1000613
Copyright: © 2018 Elbadri A, et al. This is an open-access article distributed under the terms of the creative commons attribution license, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Keywords
Chronic renal failure; Hemodialysis erythropoietin resistant; Zinc; Hemoglobin
Introduction
Anemia is one of the most frequent early complications of chronic renal failure (CKF) [1]. The main cause is lack of erythropoietin due to reduced kidney function. The treatment of anemia in CKF patients is recombinant human erythropoietin (rHuEPO) [2,3]. The main cause of rHuEPO treatment failure is the loss or low iron availability. The prevalence of iron deficiency is very common in CKF, affecting as many as 50% of patients [3-5]. How-ever, despite rHuEPO and intravenous iron in the majority of patients, the prevalence of anemia exist in large numbers of hemolysis patients [4-6]. This rise the existence of other important factors related to rHuEPO resistance, including hyper and hypothyroidism, severe secondary hyperparathyroidism, malnutrition hypoprotienemia mal-absorption and exposure to large amount of dialysis solution which does not contain any trace elements might be related to zinc and other trace elements deficiency in hemodialysis patients [7]. Zinc is an essential trace element for human’s life, which is part of many enzymes [8]. Zinc plays essential biological functions, including gene expression, protein synthesis, immune responses, and other behavioral functions [9,10]. Serum zinc levels can be decreased by increased expression of intracellular metallothioneins or oxidative stress [8-10]. Zinc deficiency may be associated with some of the uremic symptoms such as anorexia decreased immunologic function hypogeusia and sexual dysfunction [10,11]. The dialysate concentration of other trace elements is not routinely manipulated. Substances that have lower concentrations in dialysate than in blood tend to be removed by dialysis [10-12]. This is true in the case of uremic toxins; it may lead to depletion of biologically essential substances. Besides the potential for ongoing removal of trace elements by dialysis, hemodialysis patients are at risk for low dietary intake of such substances due to uremia-related anorexia and dietary restrictions [11,13]. Nemours researches illustrated strong relationship between zinc deficiency and other disorders, such as inflammation, cardiovascular diseases, oxidative stress, and erythropoietin resistant anemia. Hence this study was conducted to explore the role of serum zinc level in erythropoietin resistant anemia in hemodialysis Sudanese patients.
Material and Methods
Study population: The current study was a case control hospital base study conducted at kidney disease (HD) clinic Khartoum Sudan, during the period from February to October 2018. 50 samples were collected from erythropoietin resistant Hemodialysis patients test group (26 male, 24 female with age of 20-80 years). In addition to other 50 from nonerythropoietin resistant hemodialysis patient’s sex and age matched control group.
Inclusion criteria: Any patients who have maintenance hemodialysis at least for six month having (rhEPO) with age more than 20 years and less than 80 years.
Exclusion criteria: Any patients of CRD (HD) with age less than 20 or more than 85 years patients with known malignancy infectious disease endocrine abnormalities gastric problems over drugs alcohol abuse and treatment with steroids or immune suppresser.
Data collection and clinical examination: Each site used a standardized questionnaire which collected the demographic and symptom information assessed in this study. Clinical examinations done by clinicians in above mentioned hospital.
Sample collection: Blood was taken from each participant by standard procedures. Serum zinc was estimated by atomic absorption spectrometry (AAS) method with Zeeman background correction (Z-2000 instrument, Hitachi, Japan), in the Laboratory of National Center for Research. EDTA container was used for hemoglobin estimation which was measured by standard colorimetric method.
Ethical consideration: Informed consent was taken from all participants and ethical approval was obtained from EL Neelain University research committee.
Quality control: Samples representing the normal and pathological level of zinc (Zn) hemoglobin were used for assessment of the quality control. Results ± 2 SD of the target values of the control sera were accepted.
Statistical analysis: Data was analyzed by computer software by using SPSS program manual master sheet (SPSS version 21), the results expressed as frequency percentage mean and SD. The independent t-test was used to compare the mean level of Hb and zinc in case and control. Correlation between measured variable was significant at p ≤ 0.05.
Result
The study comprised 100 participants divided into two groups. 50 erythropoietin resistant Hemodialysis patients test group, with age range 20–80 years (male 26, female 24) and 50 non erythropoietin resistant hemodialysis patients sex and age matched control group.
As presented in Table 1, the level zinc and Hb was significantly decreased in the study group when compared with control group (0.26 ± 0.08 mg/L versus 0.67 ± 0.09 mg/L, p=0.00 and 8.56 ± 0.56 gm/L versus 11.34 ± 0.59 gm/dl, p=0.000) respectively.
Table 1 Comparison of Zinc and Hb levels in the study group with the control group.
| Parameters |
Case (mean ± SD) |
Control (mean ±SD) |
P-value |
| Zinc (mg/L) |
0.26 ±0.08 |
0.67 ± 0.09 |
0 |
| Hb (gm/dl |
8.56 ± 0.56 |
11.34 ± 0.59 |
0 |
Across gender there is insignificant difference in the level of both zinc and Hb in male when compared with female in the study (0.28 ± 0.06 mg/L 0.24 ± 0.17 mg/L, p=0.08 and 8.64 ± 0.66 gm/dl versus 8.47 ± 0.42 gm/dl, p=0.75) respectively depicted in Table 2.
Table 2 Comparison of Zinc and Hb levels across gender in the study group.
| Parameters |
Male (mean ± SD) |
Female (mean ±SD) |
P-value |
| Zinc (mg/L) |
0.28 ± 0.06 |
0.24 ± 0.17 |
0.08 |
| Hb (gm/dl |
8.64 ± 0.66 |
8.47 ± 0.42 |
0.75 |
As shown in figure the level of serum zinc is significantly correlated with Hb and inversely with age in the study group (R=0.58, P=0.00, R=-43, P=0.01) Figures 1 and 2 respectively. Whereas Hb level is insignificantly correlated with patients age in the study group (R=0.24, p=0.16) Figure 3.
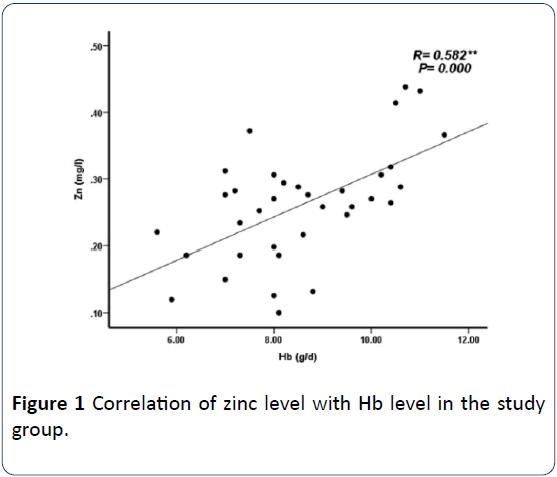
Figure 1: Correlation of zinc level with Hb level in the study group.
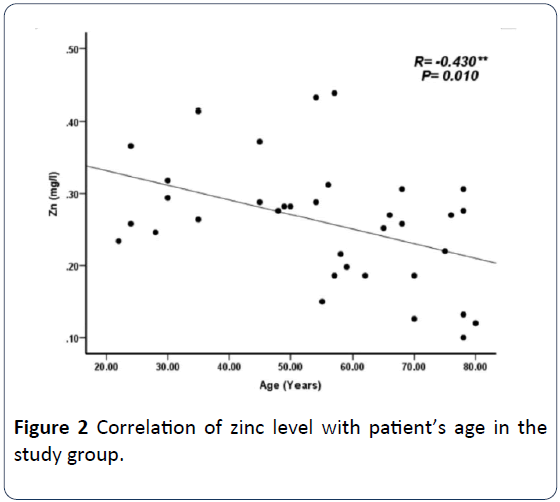
Figure 2: Correlation of zinc level with patient’s age in the study group.
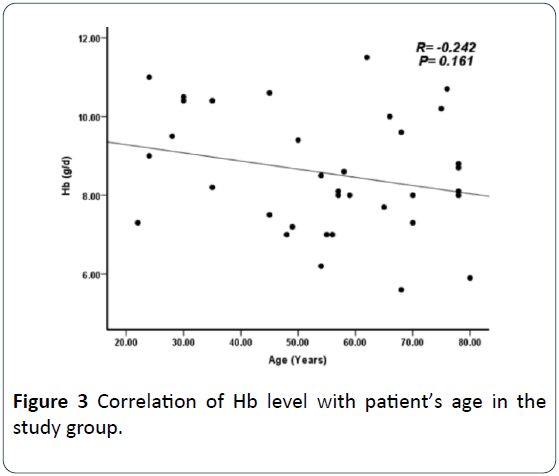
Figure 3: Correlation of Hb level with patient’s age in the study group.
Discussion
Erythropoietin resistant anemia is very series since cardiovascular mortality; morbidity and quality of life of patients are related to better control of anemia. Failure of rhEPO to correct anemia for many causes. Iron deficiency is the most important causes [14-16]. Prasad et al. [17] raised relationship between iron deficiency anemia and zinc deficiency. Great number of studies appeared in the literature in the recent years exploring the relationship between zinc deficiency and, general health, cardiovascular diseases, male infertility as well as erythropoietin resistant anemia in maintenance hemodialysis patients [5,6,17].
In the current study there was high statistically difference in the mean zinc and hemoglobin levels between the study group and the control group. The levels zinc and hemoglobin were significantly decreased in erythropoietin resistant group when compared with non-erythropoietin resistant group (P≤0.000) Which agree with the studies performed by Dashti et al. [18], Dvornik et al. [19] and Yegenaga et al. [20], whom reported that the mean serum Zn concentration in patients on maintenance HD was significantly lower than that of the control group. Serum Zn deficiency has been reported in CKD patients due to hypoproteinemia, proteinuria, tubular reabsorption impairment and calcitriol deficiency which has a role in the intestinal absorption of Zn. In addition HD patients are exposed to large amounts of highly purified dialysis solutions, which removed zinc and other essential trace elements that may lead to clinically relevant deficiency [21]. Tonelli et al. [22] performed systemic review and meta-analysis on trace elements in hemodialysis patients, and illustrated that average blood concentrations of biologically important trace elements (selenium, zinc,) were substantially different in hemodialysis patients, compared with healthy controls.
Across gender our study illustrated insignificant difference in the level of both zinc and Hb in male when compared with female in the study group. Although the level of both zinc and hemoglobin is slightly higher in male compared to female in the test group [23,24].
In the present study the level of serum zinc is significantly correlated with Hb and inversely with age in the study group. In accordance to Hiroki et al. who concluded that Zinc supplementation reduces ERI in patients undergoing HD and may be a novel therapeutic strategy for patients with renal anemia and low serum zinc levels. Although no previous studies illustrated an association between zinc concentrations and hemoglobin production, some studies observed that zinc play an essential role in erythroid differentiation and development [17,18]. Fukushima et al. [25] reported that zinc concentration and all anemia parameters showed significant positive correlation, indicating that anemia improves in patients with high serum zinc levels [19].
Conclusion
The study demonstrated that serum zinc level is significantly reduced in hemodialysis patients with erythropoietin resistant anemia.
Consent
As per international standard or university standard, patient’s written consent has been collected and preserved by the authors.
Ethical approval
As per international standard or university standard written approval of ethics committee has been collected and preserved by the authors.
Competing interests
Authors have declared that no competing interests exist.
Authors contribution
This work was carried out in collaboration between all authors. Author AEIK designed the study, performed the statistical analysis. Wrote the protocol and wrote the first draft of the manuscript. Authors (AEIK) and (AMA) managed the analysis of the study and the literature searches. All authors read and approved the final manuscript.
Acknowledgements
The authors gratefully acknowledge the HD patients at reproductive health care center and Omdurman hospital in Khartoum state Sudan for their assistance with obtaining the data used in this study.
23845
References
- Thomas R, Kanso A, Sedor JR (2008) Chronic Kidney disease and its complication. Prim Care 35: 329-344.
- Liuzzi JB, Lichten LA, Rivera S, Blanchard RK, Aydemir TB, et al. (2005) Interleukin-6 regulates the zinc transporter Zip 14 in liver and contributes to the hypozinncemia of the acute-phase response. Pro Natl Acad Sci USA 102: 6843-6848.
- Mahon A, Bennett L (2007) Renal anemia; recent development and rupture directions for improved management. J Renal Care 33: 108-114.
- Roger SD (2008) Extended administration of erythropoiesis-stimulating agents for optimizing the management of renal anemia: what is the evidence? Int J Cline Pract 62: 1413-1422.
- McClellan W, Aronoff SL, Bolton WK, Hood S, Lorber DL, et al. (2004) The prevalence of anemia in patients with chronic kidney disease. Curr Med Res Opin 20: 1501-1510.
- Lopez-Gomezv JM, Portoles JM, Aljama P (2008) Factors that conditon the response to erythropoietin on bemodialysis and their relaton to mortality. Kidney Int Suppt 111: S75-S81.
- Rucker D, Thadhani R, Tonelli M (2010) Trace element status in hemodialysis patients. Semin Dial 23: 389-395.
- Pdrasad AS, Miale A Jr, Farid Z, Sandstead HH, Schulert AR (1963) Zinc metabolism in patients with the syndrome of iron deficiency anemia, hepatosplenomegaly, dwarfism and hpypogonadism. J Lab Clin Med 61: 537.
- Kalantar-Zadeh K, Kopple JD (2003) Trace metals and vitamins in maintence dialysis patients. Adv Ren Replace Ther 10: 170-182.
- Cabral PC, Diniz AS, Arruda LK (2005) Vitamin A and zinc status in patients on maintenance haemodialysis. Nephrology 10: 459-463.
- Mahajan SK, Bowersox EM, Rye DL (1989) Factors undergoing abnormal zinc metabolism in uremia. Kidney Int 36: S269-273.
- Taylor A, Branch S, Halls D, Patriarca M, White M (2002) Atomic spectromety update. Clinical and biological materials, foods and beverages. J Anal Atom Spectrom 17: 414-455.
- Weiss G, Goodnough LT (2005) Anemia of chronic disease. New Engl J Med 352: 1011-1023.
- Arcasoy A, Cavdar AO, Babacan E (1978) Decreased iron and zinc absorpton in. Turkish children with iron deficiency and geophagia. Acta Haematol 60: 76-84.
- Lonnerdal B (2000) Dietary factors influencing zinc absorption. J Nutr 130: 1378S-1383S.
- Kilic I, Ozalp I, Coskun T, Tokatli A, Emre S, et al. (1998) The effect of zinc-supplemented bread consumption on school children with asymptomatic zinc deficiency. J Pediatr Gastroenterol Nutr 26: 167-171.
- Prasad AS, Halsted JA, Nadimi M (1961) Syndrome of iron deficiency anemia hepatosplenomegaly, hypogonadism, dwarfism and geoghagia. Am J Med 31: 532-546.
- Dashti-Khavidaki S, Khalili H, Seyedeh-Maryam V, Lessan-Pezeshki M (2010) Serum Zinc Concentrations in Patients on Maintenance Hemodialysis and its Relationship with Anemia, Parathyroid Hormone Concentrations and Pruritus Severity. Saudi J Kidney Dis Transpl 21: 641-645.
- Dvornik S, Cuk M, Racki S, Zaputovic L (2006) Serum zinc concentrations in maintenance hemodialysis patients. Coll Antropol 30: 125-129.
- Yegenaga I, Aydin Z (2014) Low Serum Zinc Level May be Related to Higher Doses of EPO in Hemodialysis Patients. BANTAO J 12: 40-44.
- Candan F, Gultekin F, Candan F (2002) Effect of vitamin C and zinc on osmotic fragility and lipid peroxidation in zinc-deficient haemodialysis patients. Cell Biochem Funct 20: 95-98.
- Tonelli M, Wiebe N, Hemmelgarn B, Klarenbach S, Field C, et al. (2009) Trace elements in hemodialysis patients: a systematic review and meta-analysis. BMC Medicine 7: 25.
- Randrianarison-Huetz V, Laurent B, Bardet V, Blobe GC, Huetz F, et al. (2010) Gfi-1B controls human erythroid and megakaryocytic differentiation by regulating TGF-beta signaling at the bipotent erythro-megakaryocytic progenitor stage. Blood 115: 2784-2795.
- Osawa M, Yamaguchi T, Nakamura Y, Kaneko S, Onodera M, et al. (2002) Erythroid expansion mediated by the Gfi-1B zinc finger protein: Role in normal hematopoiesis. Blood 100: 2769-2777.
- Fukushima T, Horike H, Fujiki S, Kitada S, Sasaki T, et al. (2009) Zinc deficiency anemia and effects of zinc therapy in maintenance hemodialysis patients. Ther Apher Dial 13: 213-219.

