Keywords
Romantic relationships, Sexual minority couples, Recruitment exclusion, Health
The Systematic Exclusion of Sexual Minority Couples from Research on Relationships and Health
Humans are hardwired for social connection, and romantic relationships are particularly important for maintaining health and positive psychological wellbeing [1]. In the last decade alone, advancements in equipment and methodology have propelled the science of romance into an even more refined examination of the link between romantic attachments and health. For example, in a magnetic resonance imaging study, Eisenberger and colleagues (2011) found that gazing at a picture of a romantic partner during an experimental pain task was associated with neurobiological processes implicated in pain reduction [2]. While the frontiers of relationship science continue to advance, there is a question as to whether same-sex relationships are represented in these discoveries.
Substantial research has been conducted highlighting the health disparities between heterosexual and LGB individuals. Early work in the area of health disparities outlined the discrimination and harassment that LGB individuals experienced in medical setting [3]. Researchers outline specific mental health outcomes associated with the denial of rights that are granted to the majority population, such banning same sex marriage [4]. Reviews and meta-analytic studies outline the negative mental and physical health implications that effect LGBs as a result of experiencing systematic exclusion and discrimination at the societal, organizational and individual level [5,6]. Recently, developments have brought increased public awareness of significant health disparities experienced by sexual minorities in North America and are likely associated with the rise in research on LGB health. The first being the Institute of Medicine report published in 2011 and the second was the recent acknowledgment by the National Institutes of Health [5] that LGB individuals comprise a population with significant health disparities and set aside research funding opportunities in hopes of understanding and reducing these disparities. While this trend is promising, empirical studies have focused primarily on LGB disease specific disparities (e.g., HIV/ AIDS) and lack of access to healthcare due to institutional biases and exclusionary policies [7]. The NIH and IOM reports do not answer the question as to whether LGBs are excluded from participating in research on relationships and health that do not have a specific LGB focus.
In 2010, Egleston et al. conducted a review of the ClinicalTrials. gov database and found that LGB couples were excluded from 15% of the clinical trials on ‘couples,’ erectile dysfunction,’ and ‘hypoactive, related to hypoactive sexual disorder’ due only to their sexual orientation. Interestingly, they also found a clinical trial on asthma that excluded lesbian and gay men from participating, without justification [8]. In an informal study by Blair (2014) in which posters from a recent conference on romantic relationships were reviewed, it was found that out of the 45 posters that examined topics concerning romantic relationships, only 15.5% of the studies stated that LGB participants were included [9]. It is yet to be examined if LGB couples are excluded from participating in research on romantic relationships or if researchers are just not mentioning that they included LGB couples in their recruitment strategies.
Exclusionary practices in research pose a threat to both the advancement of science and the particular portion of the population that is excluded from scientific inquiry. Jacklin reminded the scientific community that decades of research collected to that date had based their research findings on white, heterosexual males and yet drew misleading conclusions from this research about females, as well as sexual and racial minorities [10]. The minority stress model was proposed as a theoretical framework from which to explain the impact of routine discrimination and differential treatment that LGBs experienced on a daily basis [11]. Building on this model, researchers have demonstrated that the systematic exclusion of minority individuals from advances in science, along with stigmatizing institutional practices and polices, have negative consequences for these individuals, including increased stress burden and decrements in mental and physical wellbeing [6,12]. Lewis discuses the multiple ways in which the mental health of LGBs is affected by discriminatory policies and health practices related to the area in which they live and the limited support resources available in some regions of North America and Europe [13]. These findings, among others, support the conclusion that the exclusion of LGBs from research negatively impacts their health and wellbeing, and importantly, does not serve to instill positive change in discriminatory policies and public opinion.
There are a number of ways in which researchers may exclude LGB individuals from research. For example, LGBs may be excluded at the recruitment stage of studies, not allowing them to participate at all, or excluded from the statistical analysis, due to small numbers of LGB participants. Both of these exclusions are concerning; the former reason contributes directly to practices that perpetuate discrimination that sexual minority individuals face in daily life [9]. The latter, is a statistical concern of small samples within a larger study. However, the impact of excluding LGBs from analysis contributes to the problem that these individuals are then not represented in the advancement of scientific knowledge about the impact of relationships on health. Inclusionary recruitment is addressed in the current article and recommendations for increasing the numbers of LGBs in samples for the purpose of statistical analyses are reviewed in the discussion section.
Current paper
For the current paper, we focused our review on romantic relationships. Recognizing that the field of research on relationships is longstanding and vast, we simplified our review of the inclusivity of LGB couples in research by focusing on ‘couples’ research in the domain of physical health. The central reason for this select focus is because there have been no substantiated physiological differences discovered between LGB and heterosexual individuals that would justify their exclusion from health research [14]. Thus, we would expect exclusion rates to be lower then other domains of research within the field of romantic relationships, such as sex or reproduction, where there are characteristic differences between the experiences of LGBs and heterosexual couples. However, based on the literature reviewed above, specifically the evidence that LGB couples may be excluded from some clinical trials and recent studies that involve couples, we hypothesize that there will be significant exclusion of LGB couples from participation in research focused on romantic relationships and health. However, given the upswing in research on LGB individuals and health, we hypothesize that the rate of exclusion of LGB couples will be lower at the end of the decade (2011 & 2012) than at the beginning (2002 & 2003).
Evaluating the Current Literature
We conducted a thorough search of both the Medline and PsychINFO Ovid databases between November 2011 and January 2013. The search was limited to research on romantic relationships and health published in the decade (2002-2012). Search terms included “romantic relationships,” “couples,” “physiology,” and “health,” as well as synonyms of these words (Table 1). The PsychINFO search returned 995 articles and Medline returned 1146 for a total of 2141. We removed duplicate publications. We limited our search to include English language, original research reports conducted with human couples involved in romantic relationships (other types of nonromantic partnership or supportive relationships were excluded). Couples in dyads were recruited, even if the study focused on one member of the dyad, both members needed to be aware that they were enrolled in a study. Articles that did not examine a physical health or wellbeing outcome were excluded (e.g., relationship termination). Two researchers were trained to analyze and rate the studies. Training included the review team (two research assistants and the lead author) independently reviewing and rating 25 articles and then comparing ratings to make sure everyone was applying the review criteria according to the protocol. The review protocol was as follows: The participant recruitment and inclusion/exclusion criteria were reviewed in each article, as well as any additional supplemental material. If the article clearly stated that they recruited or excluded from recruitment non-heterosexual couples from participation in their project, the article was sorted into the appropriate category (included/excluded from recruitment). Some researchers did recruit LGB couples but later excluded them from the statistical analyses. Because we were interested in recruitment inclusion of LGB couples, any research that included recruitment of LGB couples were rated as inclusive, non-biased articles, regardless of whether they later excluded them from analyses. Some articles did not state their inclusion/exclusion criteria or give an example of the recruitment advertisement anywhere in the article. In this case, the entire article was reviewed. If exclusion criteria was still unclear, such as when sexuality was not mentioned in the participant demographics or analyses, the article was placed in a ‘questionable (n=173) category.
Table 1: Search Terms
| Medline |
PsycINFO |
| Relationship Terms |
Health/Physiology Terms |
Relationship Terms |
Health/Physiology Terms |
| Social dating |
Health |
Interpersonal Relations combined with romance |
Outcome Assessment (Health care) |
| Romance |
Well Being |
Spouses |
Primary Health Care |
| Couples |
Behavioural Medicine |
Sexual Partners |
Health Status |
| Relationship termination |
Psychosomatic Medicine |
Marriage |
Minority Health |
| Marital relations |
Disorders |
Marital Status |
Health Status Indicators |
| Marital satisfaction |
Symptoms |
Family Relations |
Behavioural Medicine |
| Relationship quality |
Health Impairments |
|
Social Medicine |
| Marriage |
Physical Health |
|
Holistic Health |
| Cohabitation |
Back Pain |
|
Cardiovascular Physiological Phenomena |
| Dyads |
Chronic Pain |
|
Physiology, comparative |
| Spouses |
Physical Disorders |
|
Digestive System Physiological Phenomena |
| Interpersonal attraction |
Myofascial Pain |
|
Down-Regulation |
| Interpersonal interaction combined with romance |
Chronic Stress |
|
Immune Tolerance |
| Relationship satisfaction |
Somatoform Pain Disorder |
|
Psychophysiology |
| Interpersonal relationships |
Syndromes |
|
Musculoskeletal Physiological Phenomena |
| Affection |
Somatoform Disorders |
|
Nervous System Physiological Phenomena |
| Intimacy |
Bruxism |
|
Respiratory Physiological Phenomena |
| |
Neuropathic Pain |
|
Skin Physiological Phenomena |
| |
Pregabalin |
|
Up-Regulation |
| |
Spinal Nerves |
|
Neurosecretory Systems |
| |
Peripheral Neuropathy |
|
Abdominal Pain |
| |
Pain |
|
Colic |
| |
Pain Thresholds |
|
Acute Pain |
| |
Pain Perception |
|
Chronic Pain |
| |
Spasms |
|
Agnosia |
| |
Pain Measurement |
|
Pain Measurement |
| |
Fibromyalgia |
|
Neck Pain |
| |
Pain Management |
|
Patellofemoral Pain Syndrome |
| |
Perceptual Measures |
|
Back Pain |
| |
Nociceptors |
|
Low Back Pain |
| |
Somatization |
|
Breakthrough Pain |
| |
Hypochondriasis |
|
Mastodynia |
| |
Physiology |
|
Pain |
| |
Morphology |
|
Chest Pain |
| |
Molecular Neuroscience |
|
Angina Pectoris |
| |
Metabolic Rates |
|
Relfex Sympathetic Dystrophy |
| |
Biochemistry |
|
Causalgia |
| |
Histology |
|
Complex Regional Pain Syndromes |
| |
Body Fluids |
|
Pain Insensivity, Congenital |
| |
Apoptosis |
|
Headache |
| |
Anatomy |
|
Facial Pain |
| |
Physiological Arousal |
|
Facial Neuralgia |
| |
Physiological Correlates |
|
Fibromyalgia |
| |
Physiological Stress |
|
Somatosensory Disorders |
| |
|
|
Eye Pain |
| |
|
|
Trigeminal Neuralgia |
| |
|
|
Temporomandibular Joint Dysfunction Syndrome |
| |
|
|
Pain, Referred |
| |
|
|
Flank Pain |
| |
|
|
Pelvic Girdle Pain |
| |
|
|
Pain, Intractable |
| |
|
|
Arthralgia |
| |
|
|
Phantom Limb |
| |
|
|
Sciatica |
| |
|
|
Pain Management |
| |
|
|
Myofascial Pain Syndromes |
| |
|
|
Nociceptive Pain |
| |
|
|
Hyperalgisia |
| |
|
|
Analgesia |
| |
|
|
Sensory Thresholds |
| |
|
|
Pain Threshold |
| |
|
|
Shoulder Pain |
| |
|
|
Neuralgia |
| |
|
|
Pain Perception |
| |
|
|
Pain, Postoperative |
| |
|
|
Visceral Pain |
All questionable articles were subjected to a third review by the first author and if necessary, consensus discussions by the team of reviewers in order to determine if other information in the paper indicated recruitment criteria. For example, one recruitment ad invited female students in love with a partner to participate in a study. They were also required to bring an opposite sex friend or acquaintance with them that was the same attractiveness of their partner, and the same sex as their partner. This recruitment strategy excludes same-sex couples from participating. After the third review (n=46) articles remained that could not be rated due to the absence of, or ambiguous recruitment information. In this case, the authors of those papers were emailed and asked to clarify their recruitment inclusion and exclusion criteria. Specifically, they were asked if they included or excluded samesex couples from participation in their study. Some authors who were emailed did not respond (n=34). We excluded these articles from the final analysis leaving a total of 591 articles that were rated for exclusion/inclusion criteria. Overall, there was agreement between raters on 97.1% of the articles extracted. The Kappa statistic between the two raters was 0.76 (p < .001), which suggests substantial agreement between the raters [15].
Of the total articles reviewed, 88.7% excluded sexual minority couples from participating in their research study. Further, a Chi Square test was performed comparing exclusion rates during the early part of the decade (2002 & 2003, n=52) and last two years of the decade (2011 & 2012, n=52). There was no significant difference in exclusion rates for the two time periods χ2 (1, N = 104) = .71, p = .678. In order to examine if exclusion rates differed across the entire decade, exclusion rates were plotted for each year (Figure 1). The results reveal that the inclusion of LGB couples in relationship research on health did not improve across the decade.
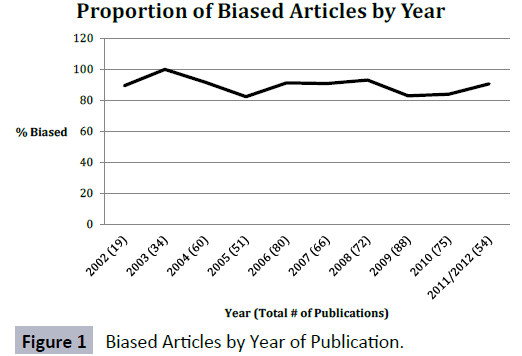
Figure 1: Biased Articles by Year of Publication.
As predicted, we found that LGB couples were systematically excluded from participating in research studies on romantic relationships and health in the decade between 2002 and 2012. Surprisingly, we did not find support for our hypothesis that the exclusion rates for the most recent years in the past decade (2011 & 2012) were lower than exclusion rates at the beginning of the decade. Our findings support previous reviews of relationship research that indicate that LGB couples are generally excluded from studies, although the findings from each study are generalized as if pertaining to all relationships [16,17]. Although the exclusion rates of LGB couples has not improved in the past decade, there seems to have been a shift in the language used to describe romantic relationships. By pulling a random sample of articles from this review (n=25) a trend noted was the increased use of inclusionary terms such as ‘partner,’ ‘significant other,’ or ‘lover’ rather than boyfriend/girlfriend or husband/wife, male/ female couple. Of the 25 articles, 14 (56%) used the term ‘partner’ and 11 (44%) used the terms ‘marital, spouse, husband/wife.’ This is a positive indication that researchers seek to be more inclusive in their language, respecting all types of coupling. However, as demonstrated by the results of this review, there is a disconnect between the use of inclusionary language and actual research practice. Moving to new terminology without actually including same-sex couples now hides the fact that they are excluded, rendering generalizations made from papers concerning couples or romantic partners misleading. This returns us to the conclusion that researchers do not set out to be biased [18] and may even adopt new language in order to reflect their good intentions. However, the scientific study of implicit associations [19] and a recent meta-analysis on the topic outlines that it is common to hold attitudes formed early in life that we are not consciously aware of as a result of societal attitudes and practice, such as stereotypes of about race, gender, age and sexual orientation. It is also understood that these negative associations may predict or shape behavior without the particular overt knowledge by the individual because these associations are likely to diverge from self-reported beliefs and behaviors [20]. Thus, researchers may be unconsciously biased in their recruitment practices without their conscious awareness.
As reviewed above, social exclusion at the community level can have detrimental relationship and health consequences for marginalized individuals [10,12,21]. The Tri-Council Policy Statement [22] that governs ethical conduct for research involving humans recognizes this. In Article 4.1 it states, “Taking into account the scope and objectives of their research, researchers should be inclusive in selecting participants. Researchers shall not exclude individuals from the opportunity to participate in research on the basis of attributes such as culture, language, religion, race, disability, sexual orientation, ethnicity, linguistic proficiency, gender or age, unless there is a valid reason for the exclusion.” This suggests that researchers should not exclude LGB couples and if they do, they should at least be explicit about their reasons for doing so.
Why might LGB populations be excluded from research on relationships?
Sampling: Research on biological markers, brain imaging and dyadic daily diary methodology can be time consuming and expensive research to conduct, often necessitating small samples. It may be the case that researchers seek to confirm if a significant phenomenon is present in a homogeneous sample before expanding research recruitment to include diverse couples. Expectations may exist that future scientists who specialize in LGB research will replicate the specific studies conducted that are limited to heterosexual couples in order to explore similarities and differences. However, given the years required to gain expertise in these research areas and the small number of researchers who conduct research on LGB relationships, it is unlikely that these same studies will be replicated with LGB couples for some time (or that LGB researchers will choose to focus on these exact same questions). Additionally, while one study may not be able to recruit a large enough sample size of LGB couples, participants from multiple studies may be combined to conduct a meta-analysis [9]. Thus, allowing LGB couples to participate broadly in research may open the door to further insights about the application of research on romantic relationships for sexual minority individuals. It is also possible that LGB individuals may hesitate to participate in research because they believe researchers are not looking to recruit them.
The question of biology. If the reasoning for excluding samesex partnered individuals is that some underlying biological difference relevant to relationships science exists, then we would expect some evidence upon which to predicate this assumption. However, almost no studies have actually been conducted on the question, and the ones that have [23] found that samesex and other-sex couples showed no significant differences in romantic love. Zeki and Romaya conducted a neuroimaging study on correlates of romantic love and found no differences in the activation of brain areas when comparing same-sex couples with heterosexual couples. Further, studies of sex hormones and relationship status among sexually diverse individuals has not yielded differences based on sexual orientation. For example, van Anders and Goldey (2010) studied levels of testosterone associated with relationship and partnering status and found that patterns of testosterone in various relationship couplings differed based on sex/gender and not sexual orientation [24]. That’s not to say we might not expect some minor or even major differences – after all, same-sex partnered individuals are subject to social stressors, such as stigma, that may impact biological processes throughout the lifespan. But we have no empirical reason to a priori exclude same-sex partnered individuals from general research on relationships, especially when the only available evidence points to similarities in biology.
Minority stress. Growing evidence exists that sexual minorities experience highly elevated rates of familial, peer and societal victimization [25-27]. This additional stress has been conceptualized as the minority stress model and researchers demonstrate that this contributes to health disparities evident between sexual minority and heterosexual individuals [28,29]. It is possible that some researchers may exclude same-sex couples out of concern that same-sex couplings are fundamentally different as a result of experiencing such marginalization. While this may be true, little research has been conducted on this topic. Further, same-sex couples are not the only minority couples that experience the burden of minority stress. Deskins and Bettinger point out the bitter bigotry that still exists in particular geographical regions of the United States for mixed race couples (particularly couples composed of Black and White individuals) [30].
Lehmiller and Agnew examined the impact of social disapproval on romantic relationship commitment among three types of couples with physically observable characteristics that draw social disapproval [31]. Specifically, individuals engaged in interracial, same-sex, and age-gap (greater than a 10 year difference in age) relationships. They found that there were no differences in perceived marginalization between the groups of marginalized couples but that all marginalized couples experienced significantly more social disapproval than traditional couples [31]. Interestingly, they found that the relationships of marginalized couples did indeed differ from traditional couples. While marginalization predicted less relationship investment, marginalized couples were more likely to be committed than non-marginalized couples. This research supports the idea that marginalized couples may experience their relationships in a different way than non-marginalized couples. However, not one article in the current review explicitly denied interracial or agegap couples from participating in their research study. In fact, the suggestion of such systematic exclusion based on race or age would likely garner strong disapproval from the scientific community
Examining gender differences. Health risks often differ by sex. For example, the prevalence of heart disease in the United States in 2010 was 7.8% among men and 4.6% among women [32]. Research examining the impact of relationship support on disease outcomes may be focused on how hormonal factors or societal roles, or gender stereotypes, may impact the responses of males and females. Including same-sex couples allows a disentangling of one’s gender from one’s gendered relationships. Questions of this nature provide researchers with the unique opportunity to include same-sex couples and conduct comparative analyses to discover if membership in a same-sex partnership impact study findings. Due to the high prevalence of heterosexual couples, there should be no concern that by including same sex couples there will not be enough opposite sex couples to run cross-sex analyses.
Another reason for the exclusion of same-sex couples is related to the current trends in dyadic data analyses. It is common for researchers who collect dyadic data to treat each members of the dyad as indistinguishable dyads by gender in an Actor-Partner Interdependence Model (APIM) [33]. Two conditions need to be satisfied before treating dyadic data as indistinguishable [33]. First, there needs to be a dichotomous variable that allows for the differentiation of each member of the dyad. If the dichotomous variable is gender, then it is only possible to run the analysis with heterosexual couples, because one cannot distinguish each member of the same-sex couple by gender. Second, the dichotomous variable needs to make some sort of an empirical difference. There is a method to test for whether a dyad is indistinguishable [34], and researchers are encouraged to conduct this test in order to preserve the more parsimonious model. Oftentimes, gender differences are minimal and dyads can usually be analyzed as indistinguishable dyads, which would allow for the inclusion of same-sex couples into the analyses [35,36]. Additionally, it is also possible to test for moderation by gender even if the data is treated as indistinguishable [37].
Furthermore, in order to properly assess gender differences within romantic couples, it is important to include male-male and female-female couples along with heterosexual couples to distinguish between gender effects due to the gender of the respondent, gender of the partner, and gender of the respondent and gender of the partner interaction [38]. For instance, consider the finding that women are more likely to experience a larger burden when caring for their partners than men [39]. If only data from heterosexual couples were used to reach this finding, then it is unclear whether the findings arose because females are more sensitive to the effects of caregiving, or because males induce greater stress on their partners when needing care. In order to disentangle these two possible explanations, researchers need to not only recruit heterosexual couples, but also male-male and female-female couples. Thus, not only are there reasons to not exclude LGB couples from the analyses, but there are also reasons to encourage the recruitment for LGB couples for statistical purposes.
Recommendations for future research
In opening relationship research to LGB couples, a distinction can be made between recruitment procedures and statistical analysis. Allowing same-sex couples to participate in research is an inclusive practice. Once recruited however, not having enough same-sex couples to conduct statistical analyses on this subgroup does not indicate a biased or exclusionary practice. However, researchers are encouraged to enhance strategies for the recruitment of same sex couples so that statistical comparisons can be completed. Researchers provide concrete strategies for recruiting diverse couples into research including List, Multipurpose, Screening and Network or Snowball sampling [28]. Other researchers have used a technique of placing two types of ads for couples research – one targeting the general population of couples (including sexual minorities) by the use of the terms “significant other,” “romantic partner,” etc, and another advertisement specifically recruiting sexual minority couples to indicate that researchers are indeed interested in recruiting LGB couples into their studies. Inclusive language on recruitment advertisements is important because many same sex couples will not respond to general research ads because of having been turned away in the past, only to face embarrassment or rejection. If only a small number of sexual minority couples respond, there is always the option to conduct statistical analyses with and without these couples to examine differences and similarities in outcomes.
Not only should researchers be more inclusive in their recruitment of LGB couples, it is recommended that peer reviewers should also be more vigilant when reviewing papers about relationships. In the informal review of conference presentations on inclusion of LGB couples in romantic relationships research, Blair included several suggestions that we echo here [9].
1. Check to ensure that the researchers have information about the sexual orientation of their participants either through a self-report scale, or by indicating the gender of their partner. If researchers do not have any information about the sexual orientation of their participants, then it would be incorrect to assume that they are all heterosexual. Researchers should be asked to provide this information in their inclusion criteria within their manuscript.
2. Examine the recruitment methods used by the researchers to ensure that they are not exclusionary. Closely check for the wording used when recruiting couples. If a researcher has omitted sexual minority couples from the analysis, make sure that the omission is valid. Heterosexual and sexual minority couples share many similarities [40], so the omission of sexual minority couples from the analysis requires a valid theoretical or a statistical validation. If there is no information available about the differences across sexual orientation, then the analysis should be conducted with and without sexual minority couples to see if results differ. While we do not suggest that a paper should be rejected solely for omitting a sexual orientation item, if the reviewers identify this potential issue to the researchers, it will encourage researchers to begin making note of sexual orientation in future studies.
It is important for researchers to understand that the exclusion of sexual minorities from their studies contributes to the dayto- day discrimination that already exists for sexual minority groups [9,41]. This exclusionary practice also goes against many of the federal, institutional, and funding agency guidelines on conducting ethical practices in research [9,22]. As scientists, whose opinions are valued in the eyes of society [42], we need to be more careful in ensuring that the way we conduct research does not negatively impact persons in society.
Conclusion
Science is arguably best served by transparency in methods, including the description of recruitment and exclusion criteria. Often it is left to activist groups to push change within a field. For example [43], Epstein highlights how the Woman’s Health Movement worked tirelessly against resistance to change the policies of federal granting agencies to require researchers to include women in medication efficacy trials [44]. However, leaving the work of changing exclusionary practices up to LGB activists places the burden of change on the very individuals who are excluded in the first place. Working together, relationship scientists can change exclusionary practices by aligning the language of inclusion with the practice of inclusion. This effort holds the rich reward of being able to truly generalize results and open doors for all types couples to reap the rewards of research on the science of relationships and health.
7377
References
- Baumeister RF, Leary MR (1995) The need to belong: desire for interpersonal attachments as a fundamental human motivation.Psychol Bull 117: 497-529.
- Eisenberg M, Shmuelof L, Vaadia E, Zohary E (2011) The representation of visual and motor aspects of reaching movements in the human motor cortex.J Neurosci 31: 12377-12384.
- D'Augelli AR (1989) Lesbians' and gay men's experiences of discrimination and harassment in a university community.Am J Community Psychol 17: 317-321.
- Herdt G, Kertzner R (2006) "I Do, but I Can't: The Impact of Marriage Denial on the Mental Health and Sexual Citizenship of Lesbians and Gay Men in the United States" Sex Res Social Policy 3: 33-49.
- Carabez R, Pellegrini M, Mankovitz A, Eliason M, Scott M (2015) Does your organization use gender inclusive forms? Nurses' confusion about trans* terminology.J ClinNurs .
- Lick DJ, Durso LE, Johnson KL (2013) Minority Stress and Physical Health Among Sexual Minorities.PerspectPsycholSci 8: 521-548.
- The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Understanding (2011) The National Academies Press.
- Egleston BL, Dunbrack RL Jr, Hall MJ (2010) Clinical trials that explicitly exclude gay and lesbian patients.N Engl J Med 362: 1054-1055.
- Blair K (2014) The state of LGBTQ-inclusive research methods in relationship science and how we can do better. Relations Res News 13: 7-12
- Jacklin CN (1981) Methodological issues in the study of sex-related differences. Developmental Review 1: 266-273.
- Meyer IH (1995) Minority stress and mental health in gay men.J Health SocBehav 36: 38-56.
- Frost DM (2011) Social stigma and its consequences for the socially stigmatized. Soc Personal Psychol Compass 5: 824-839.
- Lewis NM (2009) Mental health in sexual minorities: recent indicators, trends, and their relationships to place in North America and Europe.Health Place 15: 1029-1045.
- Zastrow C, Kirst-Ashman K (2006) Understanding human behavior and the social environment (9 eds)Cengage Learning, United States.
- Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data.Biometrics 33: 159-174.
- Graham JM (2010). Measuring love in romantic relationships: A meta-analysis. J SocPersRelat 28: 748-771.
- Peterson RA (2001)On the use of college students in social science research: Insights from a second-order meta-analysis. J Consum Res 28: 450-461.
- Fausto-Sterling (2000) Sexing the body: Gender politics and the construction of sexuality, Basic Books: University of Michigan Press, Michigan.
- Greenwald AG, Poehlman TA, Uhlmann EL, Banaji MR (2009) Understanding and using the Implicit Association Test: III. Meta-analysis of predictive validity.J PersSocPsychol 97: 17-41.
- Peplau LA, Fingerhut AW (2007) The close relationships of Lesbians and gay men.Annu Rev Psychol 58: 405-424.
- Han CS (2007)They don't want to cruise your type: Gay men of color and the racial politics of exclusion. Social Identities 13: 51-67.
- Canadian Institutes of Health Research (2010). Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans. Natural Sciences and Engineering Research Council of Canada, and Social Sciences and Humanities Research Council of Canada.
- Zeki S, Romaya JP (2010) The brain reaction to viewing faces of opposite- and same-sex romantic partners.PLoS One 5: e15802.
- Van Anders SM, Goldey KL (2010) Testosterone and partnering are linked via relationship status for women and 'relationship orientation' for men.HormBehav 58: 820-826.
- Andersen JP,Blosnich J (2013) Disparities in adverse childhood experiences among sexual minority and heterosexual adults: Results from a multi-state probability-based sample. PLoS ONE 8: e54691.
- Zou C, Andersen JP, Blosnich JR (2013) The association between bullying and physical health among gay, lesbian, and bisexual individuals.J Am Psychiatr Nurses Assoc 19: 356-365.
- Friedman MS, Marshal MP, Guadamuz TE, Wei C, Wong CF, et al. (2011) A meta-analysis of disparities in childhood sexual abuse, parental physical abuse, and peer victimization among sexual minority and sexual nonminority individuals. Am J Public Health 101: 1481-1494.
- Dean L, Meyer IH, Robinson K, Sell RL, Sember R, et al. (2000). Lesbian, gay, bisexual, and transgender health: Findings and concerns. J Gay Lesbian Med Assoc 4: 102-151.
- Roberts AL, Rosario M, Corliss HL, Koenen KC, Austin SB (2012) Elevated risk of posttraumatic stress in sexual minority youths: mediation by childhood abuse and gender nonconformity. Am J Public Health 102: 1587-1593.
- Deskins D,Bettinger C (2002) Black and White spaces in selected metropolitan areas. In Berry K, Henderson M (Eds) Geographical identities of ethnic America: Race, space, and place Reno, NV: University of Nevada Press, United States.
- Lehmiller JJ, Agnew CR (2006) Marginalized relationships: the impact of social disapproval on romantic relationship commitment.PersSocPsychol Bull 32: 40-51.
- Morbidity and Mortality Weekly Report (2011). Prevalence of Coronary Centers for Disease Control and Prevention (CDC) (2011) Prevalence of coronary heart disease--United States, 2006-2010.MMWR Morb Mortal Wkly Rep 60: 1377-1381.
- Kenny DA, Kashy DA, Cook WL (2006) Dyadic data analysis Guilford Press, United Kingdom.
- Kenny DA, Cook W (1999) Partner effects in relationship research: Conceptual issues, analytic difficulties, and illustrations. Personal Relationships 6: 433-448.
- Assad KK, Donnellan MB, Conger RD (2007) Optimism: an enduring resource for romantic relationships.J PersSocPsychol 93: 285-297.
- Debrot A, Schoebi D, Perrez M, Horn AB (2013) Touch as an Interpersonal Emotion Regulation Process in Couples’ Daily Lives: The Mediating Role of Psychological Intimacy. J PersSocPsychol 39: 1373-1385.
- Olsen JA1, Kenny DA (2006) Structural equation modeling with interchangeable dyads.Psychol Methods 11: 127-141.
- West TV, Popp D, Kenny DA (2008)A guide for the estimation of gender and sexual orientation effects in dyadic data: An actor-partner interdependence model approach. J PersSocPsychol34: 321-336.
- Yee JL, Schulz R (2000) Gender differences in psychiatric morbidity among family caregivers: a review and analysis.Gerontologist 40: 147-164.
- Kurdek LA (2005)What do we know about gay and lesbian couples? CurrDirPsycholSci 14: 251-254.
- Pizer JC, Sears B, Mallory C, Hunter ND (2011) Evidence of Persistent and Pervasive Workplace Discrimination Against LGBT People: The Need for Federal Legislation Prohibiting Discrimination and Providing for Equal Employment Benefits. Loy.L.A.L.Rev 45: 715-780.
- National Science Foundation (2012) Science and technology: Public attitudes and understanding. In Science and Engineering 2012.
- Epstein S (2008) Inclusion: The politics of difference in medical research. University of Chicago Press.
- Kenny DA, Ledermann T (2010) Detecting, measuring, and testing dyadic patterns in the actor–partner interdependence model. J FamPsychol 24: 359-366.

