Awajimijan Nathaniel Mbaba1, Michael Promise Ogolodom2*, Rufus Abam1, Beatrice Ukamaka Maduka3, Michael S. Okpaleke4, Osanaiye Abimbola Elizabeth5 and HenryTobenna Okafor6
1Department of Radiology, Rivers State University Teaching Hospital, Port Harcourt, Rivers State, Nigeria
2Rivers State Hospitals Management Board, Port Harcourt, Rivers State, Nigeria
3Department of Medical Radiography and Radiological Sciences, University of Nigeria, Enugu Campus, Nigeria
4Department of Radiography and Radiological Sciences, Nnamdi Azikiwe University Awka, Nigeria
5Olabisi Onabanjo University Teaching Hospital, Sagamu, Ogun State, Nigeria
6Benue State University, Markudi, Nigeria
- *Corresponding Author:
- Michael Promise Ogolodom
Rivers State Hospitals Management Board
Port Harcourt, Rivers State, Nigeria
Tel: +2348039697393
E-mail: mpos2007@yahoo.com
Received Date: September 30, 2020; Accepted Date: October 12, 2020; Published Date: October 16, 2020
Citation: Mbaba AN, Ogolodom MP, Abam R, Maduka BU, Okpaleke MS, Elizabeth OA, et al. (2020) Extra and Intraparenchymal Renal Artery Aneurysms Causing Hydronephrosis: a Case Report. Health Sci J. 14 No. 6: 764.
DOI: 10.36648/1791-809X.14.6.764
Keywords
Computed tomography urography; Hydronephrosis; Extra and intraparenchymal renal artery aneurysm
Introduction
Renal artery aneurysm is an infrequent pathologic entity occurring in 0.1% of the general population [1]. RAA is a form of visceral artery aneurysms (VAA) and constitute the second most common of VAA accounting for 15-22% [2], with splenic artery aneurysm as the most common, accounting for (60%) [3] of all cases. Although considered rare, RAAs in recent times are being diagnosed with increasing frequency due to increased use of cross-sectional imaging modalities such as ultrasonography, CT and MRI. RAA is intraparenchymal in less than 10% of patients detected with this disorder [4,5]. The first case of RAA was reported by Rouppe in 1970, which was the case of a sailor who died following a fall on his right flank and an autopsy revealed a large false aneurysm with rupture [6]. RAA are encountered more commonly in female population in the 4th-6th decades of life [1,7,8]. They are often asymptomatic [9] and commonly detected incidentally during abdominal investigations for unrelated pathology [1]. About 73% of patients with RAA commonly presents with hypertension [1] and a complication of spontaneous rupture, is rare but usually with a catastrophic outcome when it occurs. There is paucity of data on RAA causing hydronephrosis. To the best of our knowledge, this is the first report on this rare entity in our setting.
Case Report
We present the case of a 44-year old female patient who was referred to our facility for CT Urography to investigate the cause of left renal hydronephrosis. Patient was suspected of having a renal stone with associated hydronephrosis following abdominal ultrasound scan. The suspected stone was not echogenic and did not cast shadow. Consequently, patient was advised to do a CT urography for further assessment. The investigation was done using a GE 64 slice CT machine. Standard protocols of CT Urography were adopted. Pre and post IV contrast helical sections with coronal and sagittal reformations were obtained.
The scan revealed multiple contrast filled saccular aneurysms in the left renal artery with intra and extrarenal locations as well as dilatation of the calyceal system. There are four aneurysms distributed two each in the intra and extrarenal locations (Figures 1 and 2). The largest of the masses is intrarenal and measures 4.69 x 3.95cm. The second intrarenal aneurysm measures 1.86 x 1.79cm. Extrarenal aneurysms measures 2.56 x 2.78cm and 2.47 x 2.50cm. Delayed CT images showed clubbing of the renal calyces (Figure 3). Abdominal CT angiography was also done to confirm the lesions. A diagnosis of extra and intraparenchymal renal artery aneurysms was made. Patient was referred for surgical evaluation and we lost her to follow-up.
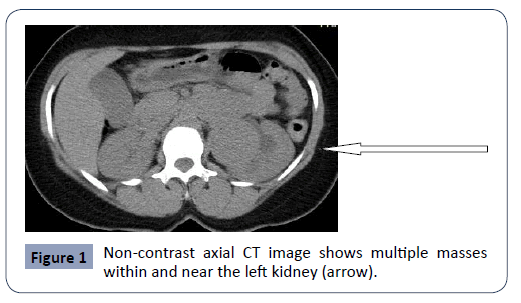
Figure 1: Non-contrast axial CT image shows multiple masses within and near the left kidney (arrow).
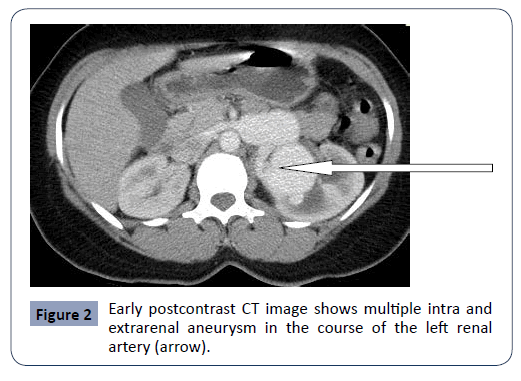
Figure 2: Early postcontrast CT image shows multiple intra and extrarenal aneurysm in the course of the left renal artery (arrow).
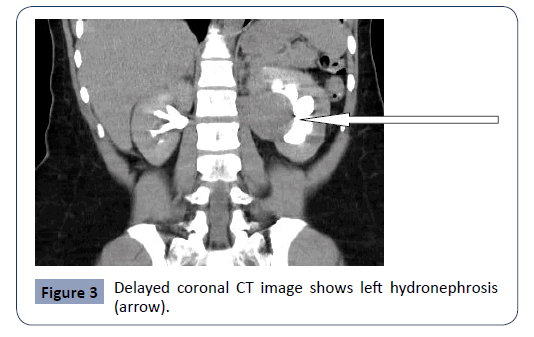
Figure 3: Delayed coronal CT image shows left hydronephrosis (arrow).
Discussion
Renal artery aneurysm is a type of visceral artery aneurysms (VAA), which affect the celiac, splenic, superior and inferior mesenteric arteries. Renal artery aneurysm is a localized dilatation of the renal artery greater than twofold the diameter of the normal renal artery [10]. Renal artery aneurysm are mostly saccular and non-calcified [9,11], more common on the right, unilateral in 80%, and multiple in 1-30% of cases [12]. In less than 10% of the patients with RAA, the lesion may be intraparenchymal in location [4,5]. RAA is common in female; likewise our patient is a female in her 4th decades, which is in agreement with previous reports [7].
In this patient under review, aneurysms are saccular and left sided. This is consistent with the report of the study conducted by Prevljak et al [13]. Nevertheless, renal artery aneurysm is known to be common on the right renal artery.
RAA can be symptomatic causing hypertension, pain, haematuria and renal infarction [14]. However, most aneurysms are asymptomatic and found incidentally during investigations for unrelated intra-abdominal disorder. Our patient did not present with any symptom that is related to renal pathology. The aneurysm in our patient was detected incidentally during routine abdominal ultrasound scan and confirmed with contrast CT scan. In this patient, the aneurysm is multiple with both extra and intraparenchymal (IPRAA) lesions causing obstruction of the calyceal system with resultant hydronephrosis. Porcaro [15] in a related article documented that although RAA is commonly asymptomatic, it may present with symptoms and signs related to complications. Similarly, it has been documented that RAA can rarely cause hydronephrosis as it is commonly located in the main renal artery and its primary branches without obstructing the pyelocalyceal system [16]. IPRAA normally occur secondary to disease or injuries of the renal vasculture and are grouped into true, false, saccular, fusiform, dissecting and microaneurysm [15]. Nevertheless, our patient denied any history of renal disease or surgery suggesting that the aneurysm may be inherited as documented in the literature [13,17].
Spontaneous rupture is the most devastating complication of RAA, which can lead to death in about 80% of cases [18]. Factors leading to rupture may include intraparenchymal location of aneurysm, hypertension, aneurysm greater than 2cm in size [12], and pregnancy with an increased risk in the third trimester [19]. Rupture in post partum period has also been reported [5,20]. The patient under review although in her late reproductive period, is at increased risk of rupture because her aneurysm is intraparenchymal and greater than 2cm in size.
Diagnosis of RAA is purely radiological and can be made with contrast CT or MRI of the abdomen. Non-contrast CT shows RAA as soft tissue mass in the region or course of the renal artery, which on post contrast CT is seen as contrast filled outpouching in the course of the renal artery. The role of Contrast CT in the diagnosis of RAA has been emphasized by many authors [13,16]. Similarly, the diagnosis of RAA in our patient was made possible by contrast CT of the abdomen.
RAA can present as an emergency with such complication as rupture. Nevertheless, most renal artery aneurysms are asymptomatic and management depends on various factors such as size and anatomic location of the aneurysm and whether or not symptoms are present. For aneurysm less than 2 cm, treatment is observational while that greater than 2 cm, treatment is surgical to avert life threatening complications.
Conclusion
Renal Artery Aneurysm is an uncommon pathology of the renal artery. It is mostly asymptomatic but can present with symptoms such as hypertension. Complications of RAA may include hydronephrosis and rupture, which could be life threatening. RAA should be remembered in the differential diagnosis when evaluating pararenal and intrarenal masses. Contrast CT is the mainstay of diagnosis and once diagnosis is confirmed, surgical assessment is required to avert unpleasant consequences. Conflict of Interest: None declared.
32214
References
- Henke PK, Cardneau JD, Welling TH, Upchurch GR, Wakefield TW, et al. (2001) Renal artery aneurysms: a 35-year clinical experience with 252 aneurysms in 168 patients. Ann Surg 234: 454-462.
- Klein GE, Szolar DH, Breinl E, Raith J, Schreyer HH (1997) Endovascular treatment of renal artery aneurysms with conventional non-detachable microcoils and Guglielmi detachable coils. Br J Urol 79: 852-860.
- Messina LM, Shanley CJ (1997) Visceral artery aneurysms. Surg Clin North Am 77: 425-442.
- Wason SE, Schwaab T (2011) Spontaneous rupture of a renal artery aneurysm presenting as gross hematuria. Rev Urol 12: e193–e196.
- Anastasiou I, Katafigiotis I, Pournaras C, Fragkiadis E, Leotsakos I, et al. (2013) A cough deteriorating gross hematuria: a clinical sign of a forthcoming life-threatening rupture of an intraparenchymal aneurysm of renal artery (Wunderlich’s Syndrome). Case Rep Vasc Med 2013: 452317.
- Rouppe DL (1770) Renal artery aneurysm. Nova Acta Phys Med Acad Nat Curios 76.
- Edwards BS, Stanson AW, Holley KE, Sheps SG (1982) Isolated spontaneous renal artery dissection presentation, evaluation, management and pathology. Mayo Clin Proc 57: 564-571.
- Yu ASL, Chertow GM, Luyckx V, Marsden PA, Skorecki K, et al. (2015) Brenner and Rector's The Kidney E-Book.
- Nosher JL, Chung J, Brevetti LS, Graham AM, Siegel RL (2006) Visceral and Renal Artery Aneurysms: A Pictorial Essay on Endovascular Therapy. RadioGraphics 26: 1687-1704.
- Chen S, Meng H, Cao M, Shen B (2013) Renal artery aneurysm mimicking renal calculus with hydronephrosis. American Journal of Kidney Diseases 61: 1036–1040.
- Zhang LJ, Yang GF, Qi J, Shen W (2007) Renal artery aneurysm: diagnosis and surveil-lance with multidetector-row computed tomography. Acta Radiol 48: 274-279.
- Tham G, Ekelund L, Herrlin K, Lindstedt EL, Olin T, et al. (1983) Renal artery aneurysms. Natural history and prognosis. Ann Surg 197: 348-352.
- Prevljak S, Carovac A, Jakirlic N (2012) Renal Artery Aneurysm. Med Arh 66: 355-356.
- Down LA, Papavassiliou DV, O'Rear EA (2013) Arterial deformation with renal artery aneurysm as a basis for secondary hypertension. Biorheology 50: 17-31.
- Porcaro AB, Migliorini F, Pianon R, Antoniolli SZ, Furlan F, et al. (2004) Intraparenchymal renal artery aneurysms. Case report with review and update of the literature. Int Urol Nephrol 6: 409-416.
- Rafailidis V, Gavriilidou A, Liouliakis C, Poultsaki M, Theodoridis T, et al. (2014) Imaging of a Renal Artery Aneurysm DetectedIncidentally on Ultrasonography. Case Reports in Radiology 2014: 375805.
- Abdel-Kerim A, Cassagnes L, Alfidja A, Gageanu C, Favrolt G, et al. (2012) Management of isolated non-traumatic renal artery dissection: report of four cases. Acta Radiol 53: 401-405.
- Henricksson C, Bjorkerud S, Nilson A, Pettersson S (1985) Natural history of renal artery aneurysm elucidated by repeated angiography and pathoanatomical studies. Eur Urol 11: 244-248.
- Cohen JR, Shamash FS (1987) Ruptured renal artery aneurysm during pregnancy. J Vasc Surg 6: 51-59.
- Nakamura R, Koyama S, Maeda M, Kobayashi M, Tanaka Y, et al. (2013) Rupture of renal artery aneurysm during the early post-partum period. Journal of Obstetrics and Gynaecology Research 39: 1476-1479.

