Keywords
Staff nurses; Absenteeism; Rates; Hail; Factor
Introduction
Absenteeism has been one of the most common causes of staff shortage in healthcare setting which significantly affect the delivery of quality healthcare services. It falls into two categories, planned absenteeism and unplanned absenteeism [1]. Absenteeism is not only detrimental to an employee's career, but to the organizations bottom line as well. Absenteeism could be an indication of managerial issues, such as low employee morale or a toxic work environment. Absenteeism is undesirable for employees, their colleagues and employers. It is therefore important to enlarge insight into possible causes, especially work- related ones.
There are many causes of absenteeism. Stressors in the job environment, individual work ethic and characteristics, cohesiveness of the employees, organizational commitment, having a voice or not and leadership are the most known factors [2]. In Australia, five percent of the Australian workforce has absent of any given day [3-5]. In the King Khalid University Hospital in the KSA, the prevalence of sickness absence is higher among contract workers than non-contract workers (16% and 9%, respectively) [6-8].
At health-care setting, nursing is the largest workforce, with their activities recorded in task division. And so, absenteeism among nurses is of major concern since they occupy a wide area of responsibility. It was concluded in the study of “Absenteeism of nursing staff: decisions and actions of nurse managers” that absenteeism varies according to the month of the year and in different service units which was classified according to units and degree of problem. Factors affecting absenteeism were determined such as: employee illness, dissatisfaction with institutional conditions and inadequate interpersonal relationships. In addition, factors associated with absenteeism were no overtime payment (75.6%) and social reasons (77.8%) [1].
In Norway and Denmark, sickness absence was more prevalent in youngest age groups, while work attendance with children and caring for an elderly parent or sick relative or child noted to contribute to absence from work [9].
However, there is also a significant effect of age on the rate of absenteeism. Mature nurses (>30 years) were viewed to have a high commitment to duty while young nurses (<30 years) were deemed to lack commitment to work and this lack of commitment contributed to a higher rate for this age group. Aside from demographic factors and absenteeism trends, seasonal patterns - winter season, December as the second highest absenteeism rate; daily patterns - Monday and Friday; workload and nature of work- those who do double shifts or overtime and night rostering and change of rostering patterns were all discussed as contributory factors of staff absenteeism.
In addition, 42.5% of nurses use to absent from duty because of minor ailments and heavy workload, 31.3% of nurses cause of absenteeism is dissatisfaction due to lack of recognition and reward [6].
Model of Absenteeism
The Steers and Rhodes model of absenteeism is regarded as one of the most influential and often cited models in absenteeism literature. In the model, employee attendance is primarily determined by an employee’s ability and motivation to attend. These two variables are also theorized to interact in such a way that someone’s perceived ability to attend moderates his or her motivation to attend [10]. Motivation to attend is influenced by a person satisfaction with his or her job and various pressures to attend. The predictiveness of different components of the Steers and Rhodes model may depend on the type of situation causing an employee ’ s absence. For example, if someone in an employee’s family is ill, the employee may need to stay at home no matter how great the motivation for attendance. However if the absence is caused by someone’s low motivation to attend, the organization may be able to take steps to increase his or her attendance. Taken as a whole, absenteeism caused by family issues, say, a sick child should be attributed to one ’ s perceived ability to attend but not motivation to attend. The job situation is described in terms of job scope, job level, role stress, work group size, co-worker relations and opportunities for advancement. Values and expectations are determined by personal characteristics, such as, age, sex, education and tenure. Satisfaction combined with various other pressures to attend such as economic conditions, incentives, work group norms, personal work ethic and commitments to determine the attendance motivation situation. Attendance motivation is a primary determinant of actual attendance, provided that the employee has the ability to attend. The ability to attend is determined by variables such as illness, family responsibilities and transport problems, which can act as constraints on employee choice. Attendance motivation and the ability to attend interact to determine actual attendance. Although, not explicitly stated, the determinants of attendance motivation appear to relate to voluntary absenteeism, whereas the ability to attend variables appears to refer to an involuntary absenteeism situation (Figure 1).
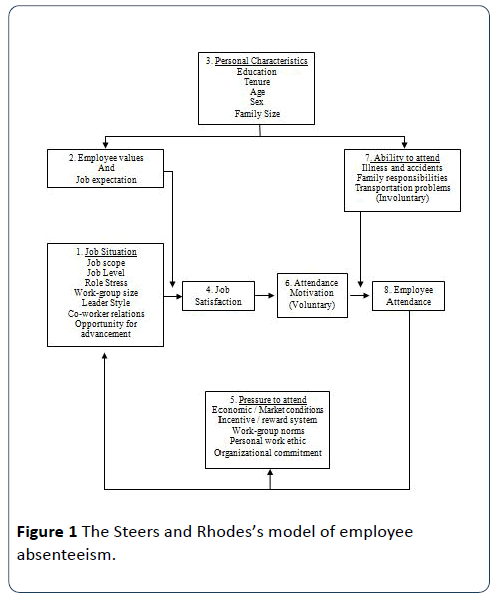
Figure 1: The Steers and Rhodes’s model of employee absenteeism.
Research design
The descriptive research design using a quantitative technique was included for the study to identify factors that impact on nursing staff absenteeism and factors that enhance staff commitment [11].
Research tool
The Researcher used a survey questionnaire in gathering the data needed in the specific problems of the study. The said instrument included eight (8) demographic profiles of the respondents, five (5) close-ended questions on level of staff satisfaction and twelve (12) close-ended questions on commitment scale using Likert Scale.
The respondents profile includes the following: age, marital status, gender and years of experience, no of working hours, frequency of absenteeism in a month and main reason of absenteeism.
The second part of the questionnaire is the response of the respondents regarding their level of satisfaction work in the PHCC which includes: clinical practice, general relationship in the unit, teamwork and leadership in the unit, process of resolving conflicts in the unit and work motivation in the unit.
The third requires the respondents to answer the level of disagreement and agreement in three categories of commitment scale: affective, continuance and normative commitment scale [12].
Targeted population
Data was collected from Saudi staff nurses in PHCC with the City of Hail.
Inclusion criteria: Saudi staff nurses of 32 PHCC within the City of Hail.
Exclusion criteria: Non-Saudi staff nurses.
Sampling technique
Stratified sampling was used.
Sample size
As cited by Sevilla et al. minimum acceptable size for descriptive research is 20% for a smaller population as small as 500 and below and 10% of the population for a larger population as large as 1,000. In this research sample size was determined by taking the 30% of the total population of nurses working in PHCC within the city. The total population was based on the Regional Nursing Administration PHCC statistics for the year 2019.
n=total population × 0.30%
=355 (0.30)
=106.5 or 107
Data Collection Procedure
Initially the questionnaire was sent electronically to each PHCC Directors with guidelines to assure nurses received the same directions and information and PHCC Directors were also instructed to forward for each staff. This included an explanation of the study objectives, participants' rights, and data confidentiality. The information provided by the participants was completely treated anonymously [13].
Statistical tool
Both descriptive and inferential statistics were used through the SPSS software program. Descriptive measurement included frequency, percent, mean and standard deviation. To evaluate the respondents’ perception of their commitment, Saudi nurses were required to respond to each item using the seven point Likert Scale, ranging from 1 strongly disagree to 7 strongly agree.
Inferential statistics included identifying variation of commitment scale between different demographical variables and identifying relationships between these with the commitment scores [14,15].
Ethical Consideration
Ethical approval was obtained from the ethical committee for human research in Hail. The study was conducted through online survey in coordination with the Primary Health Care Directors where rules and regulations of the PHCC were considered. Identity and responses of the participants were kept confidential. The results of this study were sent to all involved organizations to help them understanding these factors affecting absenteeism.
Results
A total of 110 participants joined the study. Table 1 presents the demographics of respondents whereas, majority of the respondents belong to the age bracket of 35-39 (37.3%) most of them are male 59 with 53.6%, 84 or 76.4% are married. Most of the respondents 69 (72.9%) served PHCC for more than 7 years, working for 8 hours, 105 (95.5%) and never been absent for a month 73 (66.4%) [16-18].
| Age |
No. |
Percentage (%) |
| 20-24 |
4 |
3.60% |
| 25-29 |
7 |
6.40% |
| 30-34 |
26 |
23.60% |
| 35-39 |
41 |
37.30% |
| 40-44 |
27 |
24.50% |
| 45 and above |
5 |
4.50% |
| Gender |
| Male |
59 |
53.60% |
| Female |
51 |
46.40% |
| Marital status |
| Single |
17 |
15.50% |
| Married |
84 |
76.40% |
| Widow |
3 |
2.70% |
| Separated/Divorce |
6 |
5.50% |
| Years of experience in PHC |
| 0-2 |
6 |
5.50% |
| 03-Apr |
13 |
11.80% |
| 05-Jun |
22 |
20% |
| >7 |
69 |
62.70% |
| No. of working hours |
| 6 hours |
4 |
3.60% |
| 8 hours |
105 |
95.50% |
| 10 hours |
1 |
0.90% |
| 12 hours |
0 |
0% |
| Frequency of absenteeism in a month |
| Never |
73 |
66.40% |
| Ones |
22 |
20% |
| Twice |
6 |
5.50% |
| >Two |
9 |
8.20% |
Table 1 Demographic profile of respondents.
Table 2 shows the factors influencing absenteeism. Among < the respondents ’ reasons of absenteeism, majority is having health problem 44 (40%), while working environment, personal and family problem 27 (24.5%) and due to stress 12 (10.9).
| Factors |
No. |
Percentage (%) |
| Health problem |
44 |
40% |
| Working environment |
27 |
24.50% |
| Personal/Family problem |
27 |
24.50% |
| Stress |
12 |
10.90% |
Table 2 Factors influencing absenteeism.
Table 3 presents the level of satisfaction of respondents. In terms of clinical practice, respondents were extremely dissatisfied 39 (35.5%) moderately dissatisfied 20 (18.2%), respondents feels good in their clinical practice 17 (15.5%) and slightly dissatisfied 14 (12.7%). 8 out of 110 respondents feels neutral 8 (7.3%), slightly satisfied 7 (6.4%), moderately satisfied 3 (2.7%) and 2 (1.8%) were extremely satisfied.
| Clinical Practice |
No. |
Percentage (%) |
| Extremely dissatisfied |
39 |
35.50% |
| Moderately dissatisfied |
20 |
18.20% |
| Good |
17 |
15.50% |
| Slightly dissatisfied |
14 |
12.70% |
| Neutral |
8 |
7.30% |
| Slightly satisfied |
7 |
6.40% |
| Moderately satisfied |
3 |
2.70% |
| Extremely satisfied |
2 |
1.80% |
| General relationship of their unit |
| Extremely dissatisfied |
41 |
37.30% |
| Moderately dissatisfied |
14 |
12.70% |
| Good |
25 |
22.70% |
| Slightly dissatisfied |
16 |
14.50% |
| Neutral |
5 |
4.50% |
| Slightly satisfied |
6 |
5.50% |
| Moderately satisfied |
1 |
0.90% |
| Extremely satisfied |
2 |
1.80% |
| Teamwork and leadership of their unit |
| Extremely dissatisfied |
29 |
26.40% |
| Moderately dissatisfied |
26 |
23.60% |
| Good |
34 |
30.90% |
| Slightly dissatisfied |
5 |
4.50% |
| Neutral |
11 |
10% |
| Slightly satisfied |
2 |
1.80% |
| Moderately satisfied |
0 |
0% |
| Extremely satisfied |
3 |
2.70% |
| Resolving disagreements/conflicts in the unit |
| Extremely dissatisfied |
31 |
28.20% |
| Moderately dissatisfied |
18 |
16.40% |
| Good |
25 |
22.70% |
| Slightly dissatisfied |
9 |
8.20% |
| Neutral |
15 |
13.60% |
| Slightly satisfied |
3 |
2.70% |
| Moderately satisfied |
3 |
2.70% |
| Extremely satisfied |
6 |
5.50% |
| Work motivation |
| Extremely dissatisfied |
29 |
26.40% |
| Moderately dissatisfied |
19 |
17.30% |
| Good |
28 |
25.50% |
| Slightly dissatisfied |
12 |
10.90% |
| Neutral |
15 |
13.60% |
| Slightly satisfied |
3 |
2.70% |
| Moderately satisfied |
3 |
2.70% |
| Extremely satisfied |
1 |
0.90% |
Table 3 Level of satisfaction of respondents.
According to general relationship of respondents’ to their unit majority were extremely dissatisfied 39 (35.5%) 20 feels moderately dissatisfied (18.2%) and 17 perceives good relationship 15.5%. 14 out of 110 respondents were slightly dissatisfied and remain neutral at 8 (7.3%). While 6.4% were slightly satisfied, 2.7% moderately satisfied and 1.8% extremely satisfied.
Base on teamwork and leadership in the unit, most of the respondents were extremely dissatisfied 29 (26.34%) 26 (23.6%) moderately dissatisfied while 34 (30.9% feels good about the leadership and teamwork in their unit. Only 5 (4.5%) were slightly dissatisfied and 11 (10%) remains neutral. There were only 2 (1.8%) were slightly satisfied, 0% moderately satisfied, 3 (2.7%) extremely satisfied 3 (2.7%).
As shown base on resolving conflict/disagreement, majority of the respondents were extremely dissatisfied 31 (28.2%), moderately dissatisfied 18 (16.4%) and sensed good at 25 (22.7%). There were 9 (8.2%), remains neutral at 15 (13.6%). On the contrary, respondents who feel both slightly satisfied and moderately satisfied were 6 (5.4%) and 6 (2.5%) were extremely satisfied.
As seen according to work motivation, most of the respondents 29 (26.4%) were extremely dissatisfied, moderately dissatisfied 19 (17.3%) good 28 (25.5%), 15 (13.6%) remains neutral. On the other hand, only 3 (2.7%) were slightly satisfied, 3 (2.7%) the same with those who feels moderately satisfied and only one answered extremely satisfied at 0.9%. As seen according to work motivation, most of the respondents 29 (26.4%) were extremely dissatisfied, moderately dissatisfied 19 (17.3%) good 28 (25.5%), 15 (13.6%) remains neutral. On the other hand, only 3 (2.7%) were slightly satisfied, 3 (2.7%) the same with those who feels moderately satisfied and only one answered extremely satisfied at 0.9%.
As shown in Table 4, affective commitment scale of the respondents are affected by their feelings toward their organization, including the people they are working with and their feeling of sense of belongingness as a family (3), and their views regarding their sense of oneness in the organization (4). With a mean of 3, the affective commitment scale has slightly disagreement to the respondents.
| Affective Commitment Scale |
Mean |
Interpretative |
| I would be very happy to spend the rest of my career with this organization. |
3 |
Slightly disagree |
| I enjoy discussing my organization with people outside it |
3 |
Slightly disagree |
| I do not feel a strong sense of "belonging" to my organization. (R) |
4 |
Undecided |
| I do not feel like "part of the family" at my organization. (R) |
3 |
Slightly disagree |
| Continuance Commitment Scale |
Mean |
Interpretative |
| Right now, staying with my organization is a matter of necessity as much as desire. |
3 |
Slightly disagree |
| I feel that I have too few options to consider leaving this organization. |
2 |
Disagree |
| Too much of my life would be disrupted if I decided I wanted to leave my organization now. |
3 |
Slightly disagree |
| It would be very hard for me to leave my organization right now, even if I wanted to. |
3 |
Slightly disagree |
| Normative Commitment Scale |
Mean |
Interpretative |
| Even if it were to my advantage, I do not feel it would be right to leave my organization now. |
3 |
Slightly Disagree |
| This organization deserves my loyalty. |
3 |
Disagree |
| I would feel guilty if I left my organization now. |
3 |
Slightly disagree |
| I would not leave my organization right now because I have a sense of obligation to the people in it. |
4 |
Undecided |
Table 4 Organizational commitment of respondents.
While, in terms of continuance commitment scale of the respondents which is affected by their feelings towards their own feelings or belief: staying in the organization is a matter of necessity as much as they desire (3), their feelings toward the effect of disruption in his/her life if they decide to leave the organization (3) the respondents’ feelings ton how hard it is to leave the organization for the present time (3) and their views regarding little options to consider leaving the organization (2). With a mean of 3, the continuance commitment scale has slightly disagreement to the respondents.
As manifested base on normative commitment scale when ask about the respondents feelings toward leaving the organization at this time (3), the belief of the respondent ’s fairness to be loyal in the organization (3), respondent’s feeling of guilt as end result if he/she will leave the organization (3) and the belief of the respondents of not leaving the organization because they have a sense of obligation to the organization and to people (4). With a mean of 3, the normative commitment scale has slightly disagreement to the respondents.
Discussion
There are different factors influencing absenteeism among nursing staff in the primary health care centers presented in this study, majority of them is the presence health problems. While base on recent study of 42.5% of nurses use to be absent from duty because of minor ailments and in Norway and Denmark work attendance with children and caring for an elderly parent or sick relative or child noted to contribute to absence from work [6,7].
It was also identified in the previous study by FL et al. Factors affecting absenteeism were determined such as: employee illness, dissatisfaction with institutional conditions and inadequate interpersonal relationships which was also clearly showed in this study.
Majority of the respondents were extremely dissatisfied on the following criteria: Clinical practice in the unit, general relationship in the unit, resolving disagreements/conflicts, and work motivation. Steers and Rhodes model of absenteeism employee attendance is determined by an employee’s ability and motivation to attend.
Respondents affective, continuance and normative perceptions/feeling of respondents were very low on a scale of 3 - slightly disagreement which means respondents were not emotionally attach to the organization, has a weak continuance commitment and they do not feel that they are part of the organization.
This study has a strong point as it presented the frequency of absenteeism and its factors, the level of satisfaction of nurses which is strongly correlated to the commitment scale of nurses.
It is necessary that the organization should develop strategies to combat absenteeism in the workplace and improving staff commitment as evidenced by an improvement in staff performance. The characteristics of nurses, the nurse manager, the work and the organization should be taken into account toward achieving these goals. Develop ways involve nurses awareness and involvement of the staff towards achieving on the specific goals of their center. To promote camaraderie between staff nurses, fairness, equality and provide constructive feedback to achieve a stronger affective commitment [12].
Conclusion
Nurses were found to have lack of commitment to their present job/work and are extremely dissatisfied in the administrative section. Since majority of the respondents answered they have never been absent for a month, thus considering their level of satisfaction and commitment scale, developing a motivation strategy, to make employees feel that their work is valued and creating flexibility by providing a flextime because now a days employees value personal time specially for family needs (Cliffs Notes, Motivation Strategies). Developing an in-service training program on ethicalprofessional behavior in practice and practice of giving intangible rewards, such as posting names of nurses with good attendance on the bulletin board and giving credit to nurses who are showing some improvements regarding their attendance by doing these it would enhance continuance commitment because individual's association with the organization is based on an assessment of economic benefits gained are factors that could alleviate or enhance staff commitment.
24505
References
- Alharbi FL, Almuzini TB, Aljohani AA, Aljohani KA, Albowini AR, et al. (2018) Causes of absenteeism rate among staff nurses at medina maternity and child hospital. Egypt J Hosp Med 70: 1784-1788.
- Al-Hussami M (2009) Predictors of nurses’ commitment to health care organizations. Aust J Adv Nurs 26: 36-48.
- Al Shammari (1994) Sickness absenteeism among employees of a teaching hospital in Saudi Arabia. J R Soc Health 114: 6-10.
- Andrew A (2017) Employees’ commitment and its impact on organizational performance. Asian J Econ Bus Account 5: 1-13.
- Evans J (2011) Absenteeism-a complex problem. A study on absenteeism in Trondheim’s nursing homes. Master’s thesis in cultural, social and community psychology.
- Kanwal N, Riaz G, Riaz MS, Safdar S (2013) Identify the causes of absenteeism in nurses Mayo Hospital Lahore Pakistan. J Sci Manage 4: 110-114.
- Gangai KN (2014) Absenteeism at workplace: what are the factors influencing to it? Int J Organ Behav Manage Perspect 3: 1258-1260.
- Kottwittz MU (2018) Time pressure, time autonomy, and sickness absenteeism in hospital employees: a longitudinal study on organizational absenteeism records. Saf Health Work 9: 109-114.
- Kurcgant P, Passos AR, Oliveira JM, Pereira IM, Costa TF (2015) Absenteeism of nursing staff: decisions and actions of nurse managers Rev Esc Enferm USP 49: 35-41.
- Madlinger G (2018) The 6-step process for dealing with employee absenteeism. Small business blog.
- Mafini C, Pooe D (2012) The relationship between employee satisfaction and organizational performance: evidence from a South African government department. SA J Ind Psychol 39: 1-10.
- Meyer JP, Allen NJ (2004) TCM employee commitment survey academic users guide. The University of Western Ontario pp: 1-16.
- Pilkington FB (2005) The concept of intentionality in human science nursing theories. Sage J Nursing Sci Quarterly 18: 98-104.
- Losina E, Yang HY, Deshpande BR, Katz JN, Collins JE (2017) Physical activity and unplanned illness-related work absenteeism. PLoS One 12: e0176872.

