Key words
Cardiopulmonary resuscitation, automatic external defibrillator, nurse attitudes, cardiac arrest.
Introduction
Myocardial ischemia is the leading cause of death worldwide. Whereas sudden cardiac arrest (SCA), arising from coronary artery disease, is responsible for over 60 % of deaths. In Europe sudden cardiac arrest is the leading cause of death and is responsible for 700,000 casualties per annum. Early initiation of CPR drastically increases the probability of a victim‘s survival from a heart attack. [1]
The impact of sudden death in the world is extremely difficult to measure, and varies with the prevalence of coronary artery disease in different countries. It is particularly difficult to measure the death rate of sudden cardiac arrests worldwide. Although there are no combined figures in Greece, the incidence rate appears to be more than 6000 deaths annually. [2]
The most common sudden deaths that are caused by heart attacks occur outside of a hospital. Furthermore the survival rate in such cases is very low. It is estimated that only 1-5 % of these patients survive and are discharged from the hospital. The first person who promptly arrives to provide medical care after the heart attack has begun will encounter that the victim is experiencing ventricular fibrillation and ventricular tachycardia. These heart rhythms must be confronted quickly. In an effort to improve pre hospital care, the American Heart Association has promoted the "Chain of Survival" which is a sequence of four steps that should be taken in order to help a victim of cardiac arrest. If applied, this Chain of Survival improves a person‘s chances of continued existence. It has been proven that early defibrillation, which is one step in the chain of survival, is the only significant intervention used. [3]
The European Resuscitation Council (ERC) offers guidelines for providing CPR that are revised and published every five years. Traditionally cardiopulmonary resuscitation was only performed by a physician. With the creation of these guidelines and instructions however, nursing staff has actively and directly become involved in the chain of survival in and out of the hospital. It has been scientifically proven that involving them in this process has decreased the delay in resuscitation. [4,5] Each member of the medical and paramedical community needs to know how to apply CPR and defibrillation not only in hospital but out of hospital as well.
The use of automated external defibrillators outside of the hospital can offer effective CPR for victims of cardiac arrest and this would save a significant amount of lives each year. Furthermore it would reduce the rate of severe disability caused by hypoxia of the brain for those who survive. [6,7]
Purpose
The purpose of this study was to explore the factors that influence the attitude of nursing staff in initiating CPR and in using the automated external defibrillator on victims of cardiac arrest out of the hospital.
Material and methods
The sample population of this study consisted of 310 nurses from various regions of Greece, from Athens and rural settings. A questionnaire based on a previous study was used. [8] It consisted of four parts. The first was concerned with the demographic characteristics of the respondents. The second consisted of questions inquiring about their educational experience as well as their practical experience in resuscitation. The third part explored the attitudes of the participants in the study towards initiating CPR in hypothetical situations. Lastly, the fourth part, explored the factors that influenced the attitudes towards initiating CPR.
The questionnaire was anonymous and purely voluntary. The respondents were given an explanation as to the goal of this study, that their involvement is purely voluntary, that their anonymity would be secured, that confidentiality would be maintained, and lastly that their information would not be used for other research or goals.
Statistical analysis
To find the correlation between the sample‘s level of education on resuscitation and their demographic characteristics, both the Pearson x2 and the Spearman r were used. The statistical package SPSS ver.17 was used for the analysis of the results from this study. (SPSS Inc., 2003, Chicago, USA).
Results
Study population
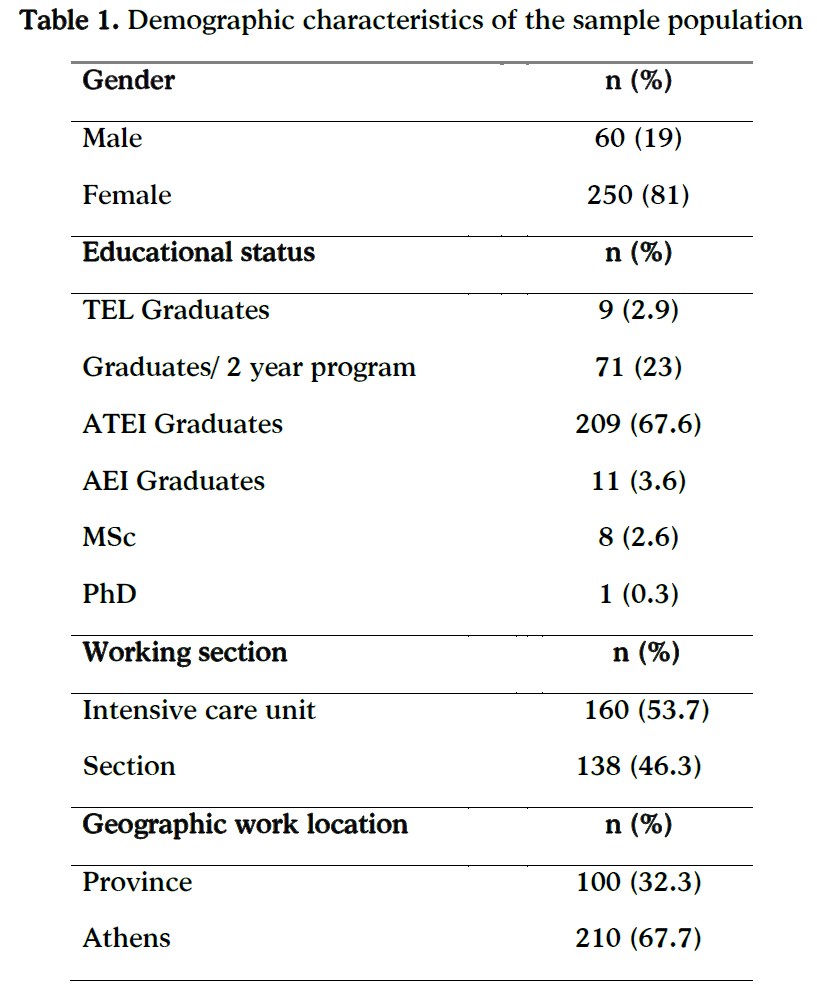
The demographic characteristics of study population are reported in Table 1. The mean age of study participants was 35±7.85 (range 20-61) years; 81% were female and 19% were male. Regarding the educational level of participants, 2.9% had completed secondary technological education lyceum (TEL), 23% had graduated from an additional 2- year program, 67.6% were graduates from Higher Technological Education Institute (ATEI) and 3.6% from University (AEI). Further, 2.6% held a master‘s degree (Msc) and 0.3% a doctoral degree (PhD), (Table 1). 53.7% of the respondents worked in intensive care units, while 46.3% worked in hospital wards. In terms of location, 32.3% of the study subjects worked in rural areas and 67.7% worked in Athens (Table 1).
Questionnaires on CPR-AED training
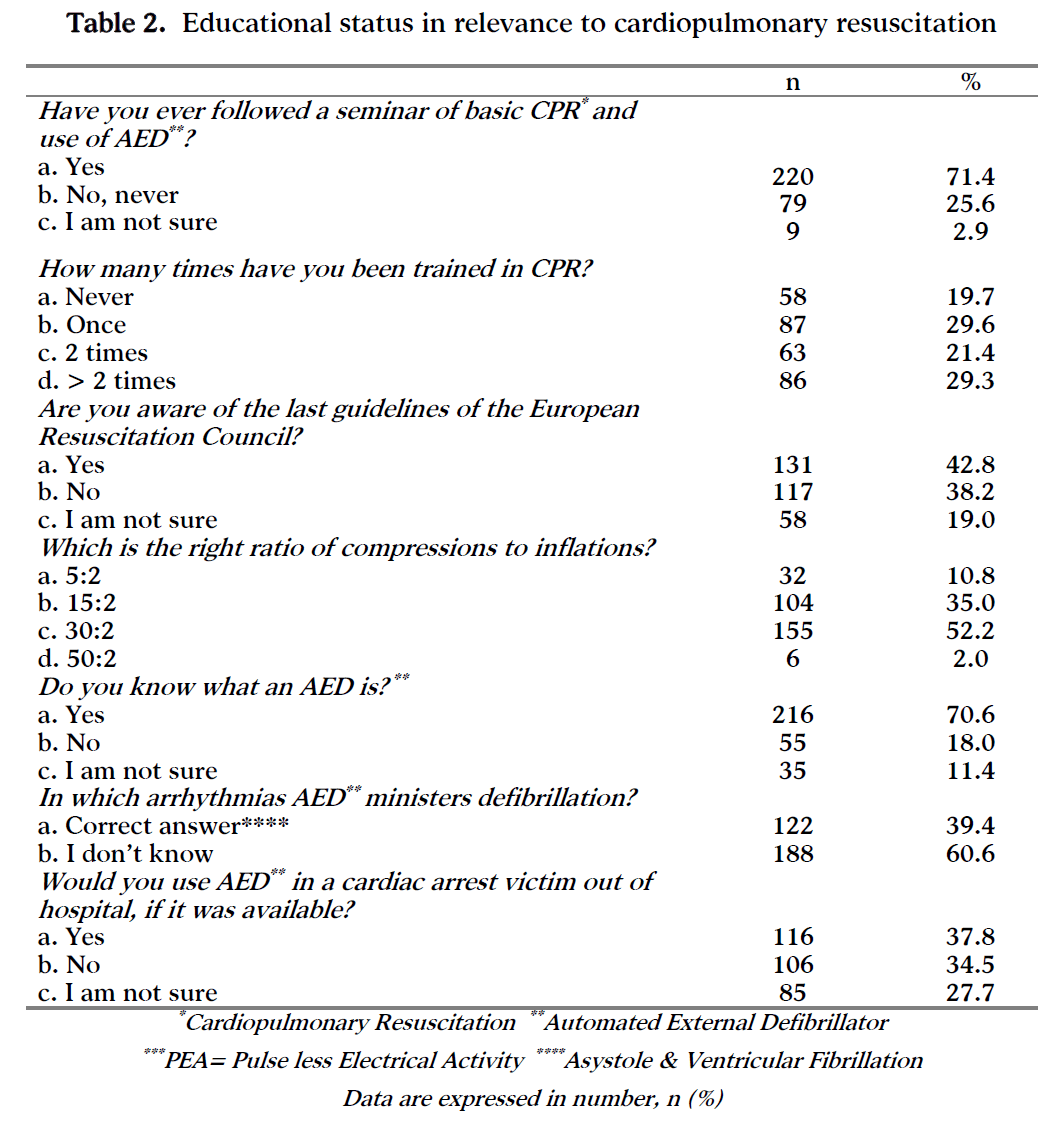
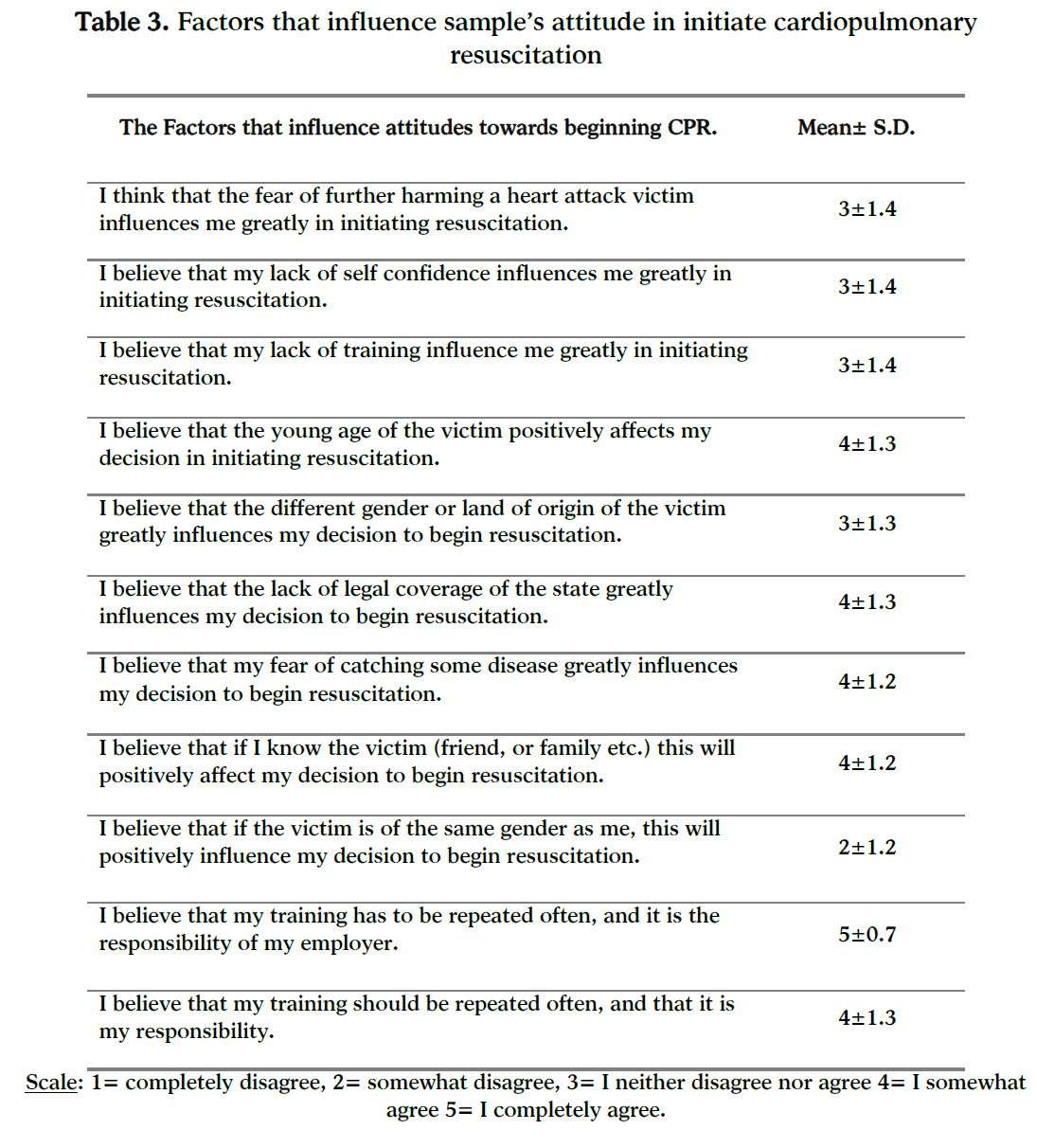
CPR training data are listed in Table 2. 71.4% of the sample had attended a basic CPR-AED course; of this sample, 29.6% had attended the course once, 21.4% had attended twice and 29.3% had taken a refresher course in CPR more than 2 times (Table 2). The answers of the nursing staff regarding the factors that may influence its attitude in initiating CPR or on operating an AED are shown in Table 3. Of interest, it is neither the lack of confidence or training that affects their attitude in helping others. Study participants neither agree nor disagree with the statement that they may be negatively influenced by a fear that they may do more harm to a victim of cardiac arrest and somewhat agree that young victim, the lack of legal coverage from the state and the fear of contracting some illness may negatively influence their decision to begin CPR (Table 3).
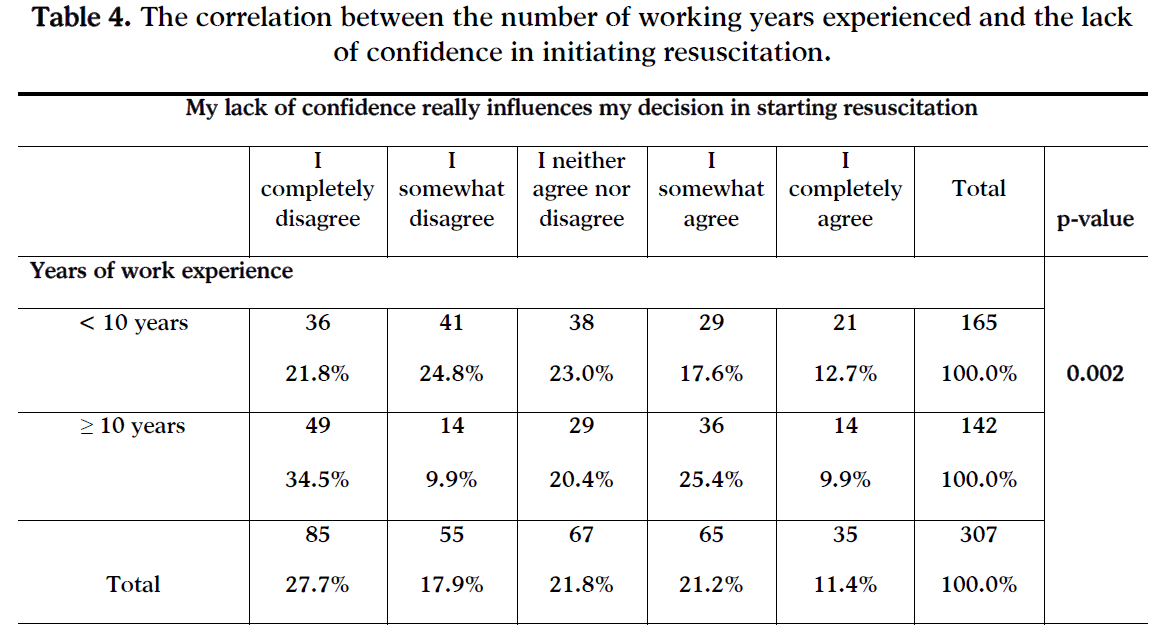
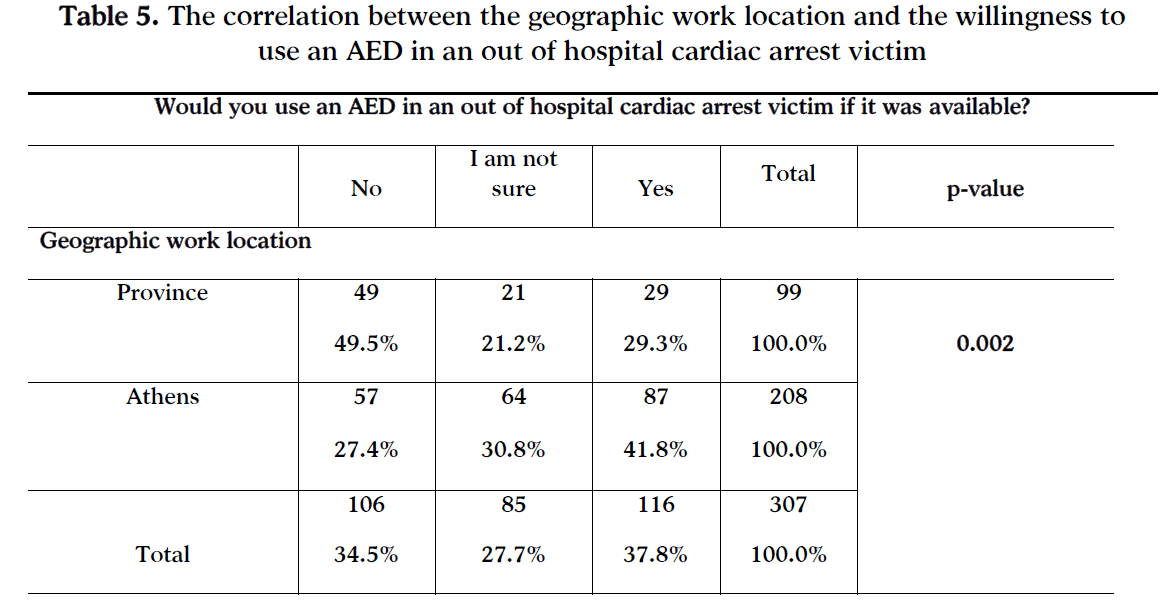
There is a statistically significant correlation between the years of working experience and with the level of confidence (p=0.002), (Table 4). So is a statistically significant correlation between geographic work location and the willingness to use AED if it was available. (Table 5).
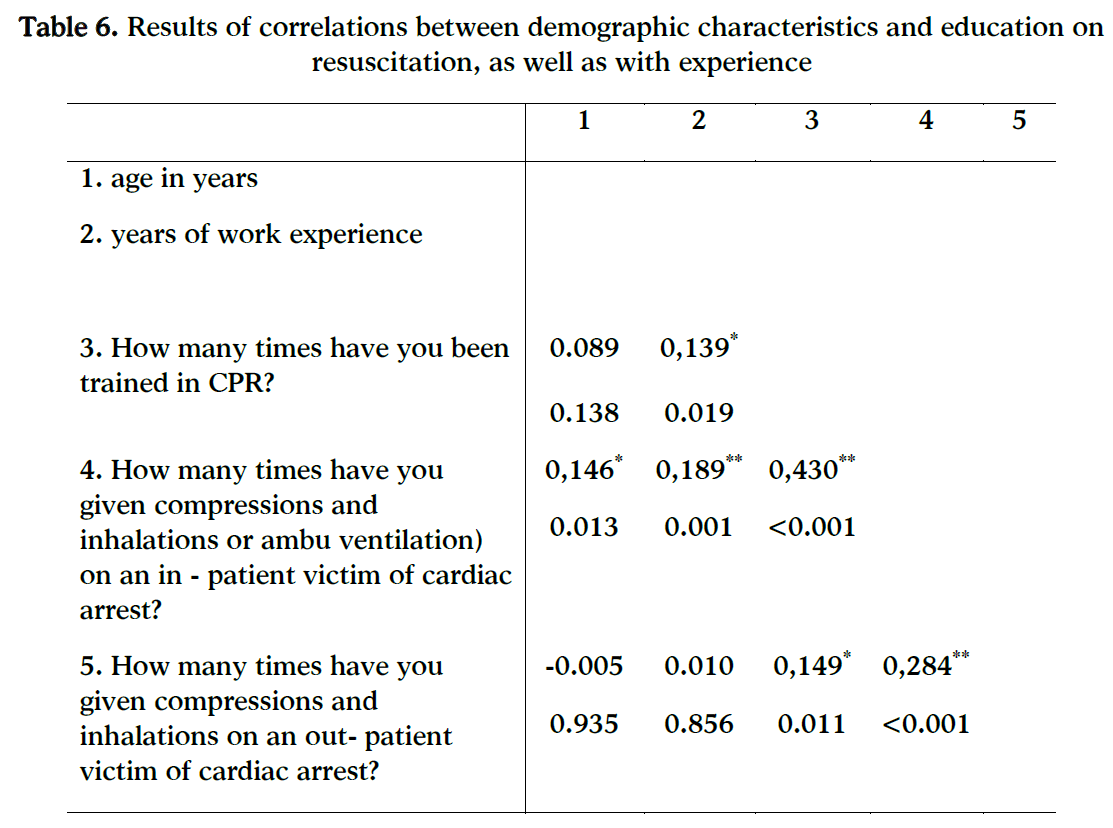
By implementing the control of 2 continuous variables using the Spearman r criterion, the following statistically significant correlations were discovered:
1) There was a statistically significant positive correlation between the age and the number of times that one has applied thoracic compressions or ventilations to a patient (r=0.146, p=0.013).
2) There was a statistically significant positive correlation between the years of work experience and the number of times the person has been trained in CPR (r=0.139, p=0.019). Therefore as work experience increases it seems that they have also been trained more times in CPR.
3) There was a statistically significant positive correlation between the years of work and the number of times that one has implemented compressions or ventilations on a patient (r=0.189, p-value<0.001). Therefore as the work experience increases so does the number of times that they have applied CPR in the hospital, (Table 6).
Discussion
The results of this study showed that the sample population has not received enough satisfactory training, as they were not able to retain information relevant to applying CPR. This conclusion stems from the fact that a great percentage of the respondents did not answer correctly to the questions on the last guidelines of the European Resuscitation Council (ERC) that were relevant to the appropriate ratio of thoracic compressions to ventilations, as well as the defibrillator rhythms. In another similar study conducted by Govender et al., [9] 20 professional health care workers had a decrease in their skills and their knowledge of CPR, even though they had been trained in CPR 3 months prior to the study.
Another similar study that was undertaken by a university clinical team in London showed that the retention of knowledge and skills during and after training in CPR is difficult and requires a more systematic training, as well as methods that will ensure better retention of skills and information. [10] In a study conducted by Soo-Il Oh et al., [11] 47 professional nurses were tested on their skill of CPR 3 times at an interval of 4 months. From the results, it was confirmed that re-education clearly affects nurse‘s knowledge and skills by maintaining their knowledge and enhancing their skills. A good example of this is represented by the results of the study done by Preusch et al., [12] which stressed the importance of training even experienced staff with the goal of adopting the guidelines for resuscitation and applying them properly in times where it becomes necessary. The factors that influence the attitudes of nursing staff in beginning CPR include the following: The fear of catching a contagious illness, and the number of times that they have been trained by their employers thus increasing their confidence in applying CPR.
As far as the first factor is concerned, similar studies done by Giammaria et al., [13] and Boucek et al., [14] report the reluctance of professional health care workers in providing mouth to mouth without the appropriate means. Their reluctance is due to their anxiety over catching an illness from the victim.
As for the second factor, which is training, the respondents in this study have expressed their wish for training that is more systematic. Repeating training helps staff retain knowledge in CPR and in using the automatic external defibrillator. Anthonypillai [15], Berden et al., [16] and Kuhnigk et al., [17] have come to the same conclusion through their studies.
Through the comparative analysis done in this study we have come across some interesting conclusions about what factors influence nurse staff‘s knowledge in CPR and in using the automatic external defibrillators. Working experience is a significant factor which reinforce nurse attitude to initiate CPR and use the AED. Nurses feel more confident of their knowledge and skills. According to the results of the study the years of work experience are closely related to the number of times the person has been trained in CPR. Training and availability of equipment help nurses use AED in resuscitation situations. There is often a gap between what is taught and what is practical in reality. Nurses need more encouragement and more information to reduce anxiety concerning defibrillation. Taniguchi et al., [18] a study on 3328 individuals, amongst them were doctors, student doctors and teachers, suggests that a large proportion of the respondents would use the AED with great confidence regardless of the fact that they lack training and knowledge on this device.
Another study done by Makinen et al., [19] that had a sample of 496 nurses, and lasted 4 years suggests that 27% of nurses are reluctant to use the AED in fear that they might cause trauma to the victim, and 64% would be reluctant out of anxiety of whether or not the machine would work. The above mentioned study concludes that there is a great need for intensive courses/training with the goal of boosting the confidence of nurses.
The results of our study also demonstrate that nurses who work in hospitals of Athens are more willing to use the AED. A possible explanation of this result is that nurses working in Athens have more opportunities of CPR training, a fact which encourage them to initiate CPR. Educational programmes increase nurse‘s confidence in their own CPR-AED skills and create a positive atmosphere towards defibrillation. [20,21] Previous studies also, as mentioned above, have demonstrated that repeated educational programmes can improve skill retention and the likelihood of using an AED. [22,23]
Conclusions
The factor that shapes nurses‘ attitudes towards beginning CPR and in using the AED is mainly work experience. The more years of experience nurses have all the more willing they will be in applying CPR. The fear of transmitting an illness during resuscitation is also another important factor that influences nurse‘s attitudes.
Having systematic and recurring training in CPR is important. It is both the responsibility of health care organizations and of individual nurses to take the initiative in following such courses. Doing so will undoubtedly increase the staff‘s confidence in beginning CPR when it becomes vital in saving a life.
5301
References
- American Heart Association, =Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care‘, 2005
- Xanthos Th, Papadimitriou D. Vasoconstrictors during cardiopulmonary resuscitation. Archives of Greek Medicine 2008;25(5):559-565
- Marenco J, Wang P, Link M, Homoud M. Improving Survival from Sudden Cardiac Arrest. The Role of the Automated External Defibrillator. JAMA 2001; 285 (9) 1193
- Makinen M, Murola-Niemi L, Kaila M, Castren M. Nurse‘s attitudes towards resuscitation and national resuscitation guidelines- Nurses hesitate to start CPR-D. Resuscitation 2009; 1399-1404
- Murola-Niemi L, Makinen M, Castren M. Medical and nursing students‘ attitudes toward cardiopulmonary resuscitation and current practice guidelines Resuscitation, 2007; 72:257-263
- Malami D, Papamichail M. Cardiac arrest: Automated external defibrillator in public places save life. Hospital Chronicles 2006, supplement: 142-145
- Parnell M, Pearson J, Galletly D, Larsen P. Knowledge of and attitudes towards resuscitation in New Zealand high-school students. Emerg Med J 2006;23:899–902
- Kapadochos Th, Karamali V, Polikandrioti M, Meidani M. Nurse‘s attitude in out of hospital cardiopulmonary resuscitation. Vima Asklipiou 2008; 7(4): 360-371
- Govender K, Ross A, Campbell L. Retention of knowledge of and skills in cardiopulmonary resuscitation among healthcare providers after training SA Fam Pract 2010;52(5):459-462
- Hamilton R. Nurses' knowledge and skill retention following cardiopulmonary resuscitation training: a review of the literature. J Adv Nurs. 2005;51(3):288-97
- Soo-Il O., Sang-Sook H. A study on the sustainable effects of reeducation on cardiopulmonary resuscitation on nurses‘ knowledge and skills. J Korean Acad Nurs. 2008; 38(3):383-392
- Preusch MR, Bea F, Roggenbach J, Katus HA, Jünger J, Nikendei C. Resuscitation Guidelines 2005: does experienced nursing staff need training and how effective is it? Am J Emerg Med. 2010;28(4):477-84
- Giammaria M, Frittelli W, Belli R, Chinaglia A, De Michelis B, Ierna S, et al. Does reluctance to perform mouth-to-mouth ventilation exist among emergency healthcare providers as first responders. Ital Heart J Suppl. 2005;6(2):90-10
- Boucek CD, Phrampus P, Lutz J, Dongilli T, Bircher NG. Willingness to perform mouth-to-mouth ventilation by health care providers: a survey. Resuscitation. 2009; 80(8): 849-53
- Fiona Anthonypillai, Retention of advanced cardiopulmonary resuscitation knowledge by intensive care trained nurses. Intensive Crit Care Nurs. 1992;8(3):180-4
- Berden HJ, Willems FF, Hendrick JM, Pijls NH, Knape JT. How frequently should basic cardiopulmonary resuscitation training be repeated to maintain adequate skills? BMJ. 1993;306(6892):1576-7
- Kuhnigk H, Sefrin P, Paulus T. Skills and self-assessment in cardio-pulmonary resuscitation of the hospital nursing staff. Eur J Emerg Med. 1994;1(4):193-8
- Taniguchi T, Omi W, Inaba H. Attitudes toward automated external defibrillator use in Japan. Resuscitation. 2008; 79(2):288-91
- Mäkinen M, Murola N, Kaila M, Castrén M. Nurses‘ attitudes towards resuscitation and national resuscitation guidelines—Nurses hesitate to start CPR-D. Resuscitation.2009; 80(12):1399-1404
- Buck-Barrett I, Squire I. The use of basic life support skills by hospital staff; what skills should be taught? Resuscitation. 2004;60(1):39-44
- Lima S, Macedo L, Vidal M, Sa M. Permanent education in BLS and ACLS: impact on the knowledge of nursing professionals. Arg Bras Cardiol 2009; 93(6):582-8,630-6
- Woollard M, Whitfeild R, Smith A, Colquhoun M, Newcombe RG, Vetteer N, Chamberlain D. Skill acquisition and retention in automated external defibrillator (AED) use and CPR by lay responders: a prospective study. Resuscitation. 2004;60(1):17-28
- Woollard M, Whitfield R, Newcombe RG, Colquhoun M, Vetter N, Chamberlain D. Optimal refresher training intervals for AED and CPR skills: a randomised controlled trial. Resuscitation. 2006;71(2):237-47

