Keywords
Persian, Fatigue Severity Scale, fatigue, multiple sclerosis, stroke
Introduction
Fatigue can be defined as an extreme sense of tiredness, lack of energy, and decreased strength with exercise or as the day progresses [1]. It is a common complaint in a large medical conditions such as sleep disorders, [2] renal failure, [3,4] systemic lupus erythematosus (SLE), [5] liver disease, adrenal insufficiency, anemia, , thyrotoxicosis, , and any malignant disease [6,7]. Fatigue also represents one of the most common disabling symptoms in patients with multiple sclerosis (MS) and stroke [5,8-14]. It has a negative effect on occupational and social activities thus reducing patient's quality of life [15,16].
Different rating scales have been developed to subjectively assess fatigue [8,17]. Among these, Fatigue Severity Scale (FSS)5 is the most discriminating self report, simple and timesaving instrument which correlates strongly with other fatigue scales [5,18-20]. It is also closely associated with the Short Form-36 of the Medical Outcome (SF-36) [21] and assesses rapidly aspects of fatigue common to not only MS and stroke but other diseases as well [8,17].
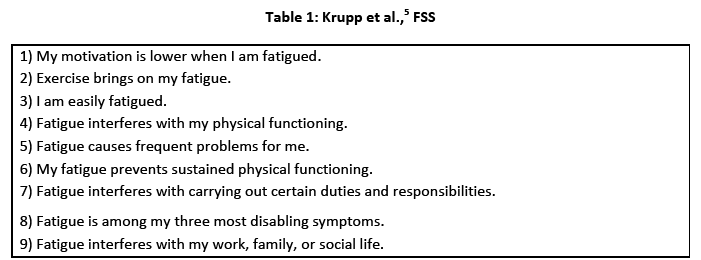
The FSS consists of nine items (table 1). For each items, the patient is asked to choose a number from 1 to 7 that indicates how much the patient agrees with each statement, where 1 indicates strong disagreement and 7 indicates strong agreement. As the original scale is in English language, the availability of a valid and reliable tool for quantification of fatigue in Iranian patients with neurological diseases such as stroke and MS, is important for clinical and research purposes. In the beginning of this study, there was not any publication about the translation and adaptation of the FSS. However, during the final stage of the present study, an article was published about the validation of Persian FSS in a small population of patients with a sub category of MS (relapsing remitting) [22]. Thus far, no research was conducted to determine the psychometric properties of the Persian FSS in neurological conditions of MS and stroke. Therefore, the aim of the present study was two fold:
(1) to compare the level of self-perceived fatigue between patients with MS and patients with stroke , and (2) to examine the validity and reliability of the Persian version of the FSS (P-FSS) in the study population.
Methodology
The study was conducted at the MS and stroke rehabilitation clinics. The methods and procedures used in this research were approved by the Research Council and Ethics Committee affiliated with Tehran University of Medical Sciences and all subjects signed an informed consent form.
Persian translation and adaptation of FSS
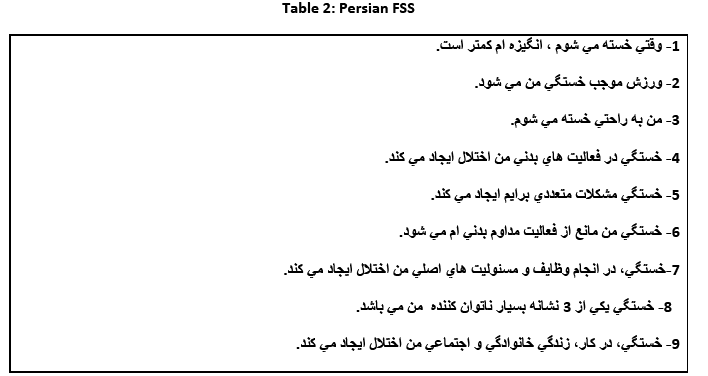
Initially, two independent specialists who were not familiar with the scale translated the original FSS from English to Persian. An expert committee experienced in neurological rehabilitation reviewed 2 forward translations, and synthesized one Persian version of FSS.Thereafter; two bilingual specialists blinded to the study, back translated the synthesized Persian FSS into English, and the prefinal version was produced after the committee reviewed all translations and original English FSS. Content validity of this prefinal version was tested on a group of patients (n = 30), and all items were understood by them. Finally, the Persian version of FSS was produced (table 2).
Subjects
Two different patient groups (MS and stroke: n= 30 and n=83, respectively) with two age-matched healthy groups [30 for MS (healthy group 1) and 60 for stroke patients (healthy group 2)] included in the study. All participants had the ability to read Persian. The exclusion criteria for this research were any other orthopedic, neurologic, and or rheumatologic diseases.
Outcome measures
The outcome measures were the Persian FSS and a Visual Analog Scale (VAS). All subjects were asked to fill up the Persian FSS and to quantify their fatigue in the previous week on a 0-10 cm fatigue VAS, where 0 indicates “no fatigue” and 10 “extremely fatigued.”
Statistical Analysis
Floor or ceiling effect were considered to be present if more than 15% of patients in each groups received the lowest or the highest possible Persian FSS scores. Test –retest reliability of the scale was measured using the Intraclass Correlation Coefficient (ICC) with 95% confidence interval (CI)23 and paired t-test. Values of 0.70–0.80 were accepted as evidence of good test-retest reliability and with those above 0.80 regarding excellent reliability [24].
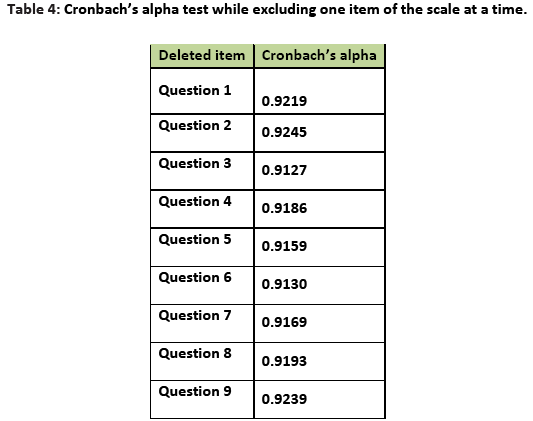
Internal consistency reliability or the degree of inter-item correlation within the scale was computed by Cronbach's alpha for 9 items (recommended value α≥ 0.70).23 The analysis was also conducted excluding one item each time to check the contribution to that particular item to the homogeneity of the scale.
Spearman correlation coefficient was used to assess concurrent validity. In addition, discriminative validity was assessed by comparing the FSS scores between patients and healthy persons. The validity coefficients were accepted as follows: 0.81–1.0 as excellent, 0.61–0.80 very good, 0.41–0.60 good, 0.21–0.40 fair, and 0–0.20 poor.25 SPSS version 16 for windows was used for statistical analysis.
Results
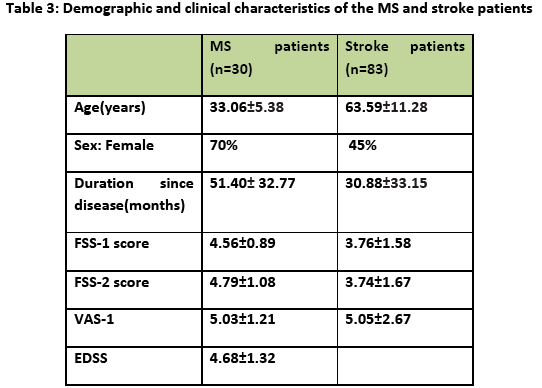
The mean ages of the two healthy groups were 31.4 SD 6.02 (range: 21-45) and 61.3 SD7.68 (range: 50-77) years for group 1 and 2, respectively. Patients with MS (aged 25 – 46 years) and stroke (aged 30–85 years) filled out the questionnaire and also quantify their fatigue by fatigue VAS. Demographic and clinical characteristics of the patients' groups have been shown in table 3. No floor or ceiling effect was found neither in patients with MS nor in patients with stroke.
FSS: Comparison between Groups
Mean Persian FSS scores were 4.56 SD 0.89 in MS patients (≥ 4.0 in 73.3%), 3.76 SD 1.58 in patients with previous stroke (≥ 4.0 in 45.8%), 3.11 SD 2.27 for healthy group1 (≥ 4.0 in 16.7%) and 2.85 SD 1.00 for healthy group 2 (≥ 4.0 in 16.7%). When FSS scores were dichotomized using 5.0 as cut-off point, [26] the prevalence of fatigue were 46.7% and 26.5% in MS and stroke patients, respectively.
The Cronbach's alpha for healthy subjects and patient groups were 0.79 and 0.93, respectively.Whenever one item was excluded alpha values did not reveal improved scale homogeneity (Table 4).
There was a significant positive correlation between Persian FSS and fatigue VAS (0.83: MS, 0.72: stroke; p<0.001). For the entire patients (n=113), a highly significant correlation was found (r=0.70, p<0.001). MS patients were younger than stroke patients (p<0.001). The mean FSS scores for patients with MS was significantly greater than those for stroke patients (p=0.001).On the VAS for fatigue, there was no significant differences between the patient groups (p>0.05). Discriminated validity was assessed to show the ability of FSS score to distinguish patients from control groups. The FSS scores in patient groups were significantly higher than those in control groups (p= 0.002 and p<0.001 for MS and stroke, respectively).
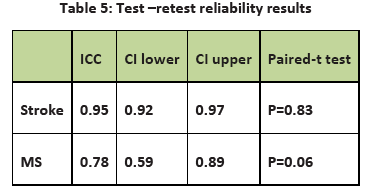
The test-retest reliability of FSS was examined in 113 patients. The patients were examined at two time points separated by one week. No significant changes were noted (p>0.05) (table 5).
Discussion
The results of this study demonstrate that test-retest reliability coefficients were very good to excellent in MS and stroke patients, respectively. Furthermore, there was no statistically significant difference between the FSS scores in the two evaluation sessions .These results indicate that the Persian FSS has high stability over time and is an appropriate tool for assessing fatigue in repeated measures. The FSS’s internal consistency values for both patients groups confirmed that Persian FSS had high internal consistency.
The reproducibility values have been reported 0.94 for fibromyalgia (FM) [27] and 0.81 for MS patients [28]. Furthermore, Krupp et al., [5] reported the Cronbach’s alpha coefficient of 0.81, 0.89 and 0.88 for patients (MS and SLE) and normal subjects. This value was reported 0.94 for chronic hepatitis C patients, [29] 0.94 for Parkinson disease, [30] 0.88 for Norwegian population [26] and 0.85 for FM patients [27]. Similar to our findings, Valko et al., [31] and Mattson et al., [32] reported satisfactory internal consistency for FSS scores (0.94: MS and SLE, 0.96: stroke).In another study, alpha coefficient was reported 0.89 for Turkish MS patients [28].
Our results showed high correlation between the Persian FSS and fatigue VAS scores in both patient groups providing support for validity in the groups. In the patients with spinal cord injury, Anton et al., [33] showed high correlation between two measurements (0.67) . Also, significant correlation were found for patients with hepatitis C (0.75), MS (0.79), stroke (0.70), FM (0.63), and in healthy subjects (0.94) [27,29,31].
In the present study, 16.7% of the healthy groups had a score of 4 or higher in comparison with 73.3% of patients with MS and 45.8% of patients with stroke. MS patients experienced high fatigue more than stroke patients. On the other hand, although MS patients were younger than stroke, but their mean FSS scores was significantly greater than that for stroke patients (p=0.001). On the VAS for fatigue, we found no significant differences between the patient groups. The FSS measures the impact of fatigue on daily functioning rather than the intensity of fatigue symptoms as VAS fatigue. It seems that multiple-item scale is more reliable than a single indicator [34,5]. Thus the Persian FSS items clearly distinguished not only between patients groups but also between healthy people and patient groups. In the study of Gencay-Can [27] the FSS scores of the FM patients were significantly higher than the scores of the healthy controls. Furthermore, the fatigue had been shown to be more pronounced in MS patients than patients with ischemic stroke [31,35] and most patients with sleep-wake disorders [31].
It has shown that the original FSS is sensitive to the effects of variety interventions, [36] so further research is suggested to evaluate the responsiveness of Persian FSS in order to assess the efficacy of medical or rehabilitation interventions. In addition, further validation of the Persian FSS in the other groups of patients (e.g. neuropathies, sleep disorders, renal failure, liver disease, etc.) is recommended.
In conclusion, our finding showed that self-perceived fatigue level was more pronounced in MS than stroke patients. The Persian FSS is a reliable and valid measure to detect presence and severity of fatigue in patients with MS and stroke. We recommend Persian FSS for measuring fatigue in clinical practice and research settings.
Acknowledgement
We would like to thank Dr.Kazemi, manager of Tabassom center, for his cooperation and assistance.
2811
References
- Krupp LB, Pollina DA. Mechanisms and management of fatigue in progressive neurological disorders. Curr Opin Neurol 1996; 9(6):456-460.
- Hossain JL, Ahmad P, Reinish LW,Kayumov L,Hossain NK,Shapiro CM. Subjective fatigue and subjective sleepiness: two independent consequences of sleep disorders? J Sleep Res 2005;14(3):245-253.
- Tel H. Determining quality of life and sleep in hemodialysis patients. Dial Transplant 2009;38(6):210-215.
- Lee B, Lin C, Chaboyer W, Chiang C, Hung C. The fatigue experience of hemodialysis patients in Taiwan. J Clin Nurs 2007;16(2):407-413.
- Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol 1989; 46(10):1121-1123.
- Hjollund NH, Andersen JH, Bech P. Assessment of fatigue in chronic disease: a bibliographic study of fatigue measurement scales. Health Qual Life Outcomes 2007;5:12.
- Campos MP, Hassan BJ, Riechelmann R, Del Giglio A. Cancer-related fatigue: a review. Rev Assoc Med Bras 2011 ;57(2):211-219.
- Krupp LB, Coyle PK, Doscher C, Miller A, Cross AH, Jandorf L, et al. Fatigue therapy in multiple sclerosis: results of a double-blind, randomized, parallel trial of amantadine, pemoline, and placebo. Neurology 1995;45(11):1956-1961.
- Brañas P, Jordan R, Fry-Smith A, Burls A, Hyde C. Treatments for fatigue in multiple sclerosis: a rapid and systematic review. Health Technol Assess 2000;4(27):1–61.
- Zifko UA. Management of fatigue in patients with multiple sclerosis. Drugs 2004;64(12):1295-1304.
- Krupp LB , Fatigue in Multiple Sclerosis ,Definition, Pathophysiology and Treatment . CNS Drugs 2003; 17(4): 225-234.
- Lerdal A, Kottorp A. Psychometric properties of the Fatigue Severity Scale-Rasch analyses of individual responses in a Norwegian stroke cohort. Int J Nurs Stud 2011;48(10):1258-1265.
- Choi-Kwon S, Han SW, Kwon SU, Kim JS. Poststroke fatigue: characteristics and related factors. Cerebrovasc Dis 2005;19(2):84-90.
- Staub F, Bogousslavsky J. Fatigue after stroke: a major but neglected issue. Cerebrovasc Dis 2001;12(2):75-81.
- H?user W, Stallmach A, Kocalevent RD, Rose M, Fliege H. Biopsychosocial predictors of fatigue in quiescent and mild ulcerative colitis: an explorative study. Psychosoc Med 2005; 2:Doc07.
- Henze T. Managing specific symptoms in people with multiple sclerosis. Int MS J 2005; 12(2):60-68.
- Flachenecker P, Ku?mpfel T, Kallmann B, Gottschalk M, Grauer O, Rieckmann P, et al. Fatigue in multiple sclerosis: a comparison of different rating scales and correlation to clinical parameters .Multiple Sclerosis 2002; 8(6):523-526.
- Iriarte J, Katsamakis G, de Castro P. The fatigue descriptive scale (FDS): a useful tool to evaluate fatigue in multiple sclerosis. Mult Scler 1999; 5(1): 10-16.
- Krupp LB, Soefer MH, Pollina DA, Smiroldo J, Coyle PK. Fatigue measures for clinical trials in multiple sclerosis. Neurology 1998;50:A126.
- Taylor RR, Jason LA, Torres A. Fatigue rating scales: an empirical comparison. Psychol Med 2000; 30(4): 849-56.
- Tang WK, Lu JY, Chen YK, Mok VC, Ungvari GS, Wong KS. Is fatigue associated with short-term health-related quality of life in stroke? Arch Phys Med Rehabil 2010; 91(10):1511-5.
- Azimian M,Shahvarughi Farahani A, Dadkhah A,Fallahpour M,Karimlu M. Fatigue severity scale: the psychometric properties of Persian- version in patients with multiple sclerosis , Research Journal of Biological Sciences, 2009,4(9):974-977.
- Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL, Dekker J, et al . Quality criteria were proposed for measurement properties of health status questionnaire .J Clin Epidemiol 2007,60(1):34-42.
- Shrout PE, Fleiss J . Intraclass correlations: uses in assessing rater reliability. Psychol Bull 1979;86(2):420-428.
- Feise RJ, Menke JM . Functional rating index: a new valid and reliable instrument to measure the magnitude of clinical change in spinal conditions. Spine 2001; 26(1):78-86;discussion 87.
- Lerdal A, Wahl A, Rustoen T, Hanestad BR, Moum T. Fatigue in the general population: a translation and test of the psychometric properties of the Norwegian version of the Fatigue Severity Scale. Scandinavian Journal of Public Health 2005;33(2): 123-130.
- Gencay-Can A, Can SS. Validation of the Turkish version of the fatigue severity scale in patients with fibromyalgia. Rheumatol Int 2012 ;32(1):27-31.
- Armutlu K, Korkmaz NC, Sumbuloglu V, Akbiyik DI, Guney Z, Karabudak R . The validity and reliability of the fatigue severity scale in Turkish multiple sclerosis patients. Int J Rehab Res 2007;30(1):81-85.
- Kleinman L, Zodet MW, Hakim Z, Aledort J, Barker C, Chan K, et al. Psychometric evaluation of the fatigue severity scale for use in chronic hepatitis C. Qual Life Res 2000;9(5):499-508.
- Hagell P, Höglund A, Reimer J, Eriksson B, Knutsson I, Widner H, et al. Measuring fatigue in Parkinson's disease: a psychometric study of two brief generic fatigue questionnaires. J Pain Symptom Manage 2006 ;32(5):420-432.
- Valko PO, Bassetti CL, Bloch KE, Held U, Baumann CR. Validation of the Fatigue Severity Scale in a Swiss cohort. Sleep 2008; 31(11): 1601-1607.
- Mattson M, Möller B, Lundberg IE, Gard G, Boström C. Reliability and validity of the Fatigue Severity Scale in Swedish for patients with systemic lupus erythematosus. Scand J Rheumatol 2008 ;37(4):269-277.
- Anton HA, Miller WC, Townson AF. Measuring fatigue in persons with spinal cord injury. Arch Phys Med Rehab 2008;89(3):538-542.
- Dittner AJ , Wesselyb SC, Brown RG .The assessment of fatigue: a practical guide for clinicians and researchers. J Psychosom Res 2004;56(2):157?170.
- Gramigna S, Schluep M, Staub F, Bruggimann L, Simioni S, Bogousslavsky J, et al. Fatigue in neurological disease: different patterns in stroke and multiple sclerosis ,Rev Neurol 2007,163(3):341-8.
- Krupp LB, Christodoulou C. Fatigue in multiple sclerosis. Curr Neurol Neurosci Rep 2001; 1(3):294-298

