Ancia Manwere1, Tirivanhu Chipfuwa2*, Maceline Mutsa Mukwamba3 and Geldine Chironda4
1Lecturer, Department of Health Sciences, Faculty of Science, Bindura University of Science Education, Bindura, Zimbabwe
2Lecturer, Department of Health Sciences, Faculty of Science, Bindura University of Science Education, Bindura. Zimbabwe
3Tutor, School of Nursing and Midwifery, United Bulawayo Hospitals, Bulawayo, Zimbabwe
4Lecturer, School of Nursing and Public Health, University of Kwazulu Natal, Kwazulu Natal, South Africa
*Corresponding Author:
Tirivanhu Chipfuwa
Bindura University of Science Education
Department of Health Sciences
Private Bag 1020, Bindura, Zimbabwe
Tel: +263 773 295 150
E-mail: chipfuwat@yahoo.co.uk
Introduction
Nurses play a pivotal role in pain management [1]. Untreated and undertreated pain has debilitating effects and significantly interferes with the patient’s physical, emotional and spiritual well being, thus can alter the patient’s quality of life [2-5]. Lui, So and Fong reported that pain is a common symptom in patients in medical units and effective pain management strategies can relieve it effectively [6]. Basic principles of pain management recommends that pain should be assessed regularly i.e. together with other vital signs [7]. However, self-report is considered by health care providers as the best tool for the assessment of pain, rather than focusing on the patients’ behaviour [8,9].
The most common reasons for not acting on a patient’s report of pain especially intramuscular administration of morphine are the belief that the patient is or will be addicted to the narcotics , respiratory depression and masking the patient’s symptoms [10-13]. Nurses knowledge of pain management is weak with incorrect answers being highest on pharmacology and assessment of pain although research shows that if health care providers assess and treat pain before it becomes severe, sensitization is avoided and less medication is needed [1,5,11,14]. Nurses also have the key responsibility of providing non-pharmacological therapies to patients as adjuvant to pharmacological interventions to maximise relief of pain. The non-pharmacological interventions are grouped as cognitive and physical. Cognitive techniques focus on mental functions and these include music and relaxation. Physical techniques focus on altering physiological processes to reduce pain and these include massage and application of heat and cold [15].
The criterion for minimally acceptable percentage score on the Nurses Knowledge and Attitudes Survey Regarding Pain Tool (NKAS) is 80%. Both knowledge and attitudes affect the nurses’ ability to effectively manage pain [5,16]. Studies done in different countries with nurses in adult medical wards revealed that a deficit in knowledge relating to pain management was prominent i.e. percentage of total scores were ranging from 39.65 to 72,3 with knowledge scores on pharmacology rarely exceeding 65% [1,3,5,6,9,11-13,16-18]. Although the nurses in these studies had appropriate attitudes towards pain management, there were discrepancies between practice and attitude. This means that nurses may have positive attitude towards pain management but without sufficient knowledge to effectively relieve the pain. However, Kassa and Kassa had different findings which showed that nurses had poor knowledge and 53.7% had negative attitude towards pain management which was attributed to low salaries, lack knowledge and role confusion in pain management [13].
Other studies concluded that clinical experience is the most influential factor that promotes nurses knowledge and confidence in managing patient’s pain. Nurses with longer clinical working experience applied knowledge of pain to their daily practice [6,19]. However, a study done in Malaysia revealed that registered nurses’ personal experience with pain had influenced their practice in pain management. Age groups of more than 40 years had better knowledge (p=0.046) in this study [2]. However Yava et al had different findings in Turkey. There were no statistically significant relationships between knowledge on pain management and demographic variables such as age, years of experience and rank (p>0.05) [3].
A study to explore knowledge and attitudes of pain management among nursing faculty revealed that nurses incorrectly reported that measuring vital signs such as blood pressure and pulse was an accurate way to assess the level of pain a patient was experiencing. They also indicated facial expression as a way of assessing pain levels. Nurses also incorrectly reported that patients did not give reliable reports of pain and that nurses could be fostering patients’ addiction to opioids. Kasa and Kassa agrees with these findings and added that respondents reported that they would focus on patients’ behaviour to measure pain intensity [13,20].
A review of literature revealed there are no studies that examined Zimbabwean nurses’ knowledge and attitudes regarding pain management among adult medical patients. The purpose of this study therefore was to assess the knowledge and attitudes of registered nurses towards pain management of adult medical patients. This line of inquiry is important because absence of pain is part of the basic human rights to health. Findings from this study add important information to the literature regarding nurses’ knowledge and attitudes towards pain management of adult medical patients in Bindura, Zimbabwe and can be used to inform future interventions that improve pain assessment and treatment.
Purpose
The purpose of this study was to assess the knowledge and attitudes of registered nurses towards pain management of adult medical patients in Zimbabwe.
Material-Method
A descriptive study to assess the knowledge and attitudes of registered nurses towards pain management of adult medical patients was carried out at Bindura Provincial Hospital. A sample of 50 consenting registered nurses was drawn using a systematic random sampling method. A self-administered, questionnaire was used to collect data. A questionnaire was developed from relevant literature specifically for this study to obtain data for the quantitative approach design. The questionnaire consisted of 30 questions specifically designed to highlight the: Demographics (Section A), Knowledge (Section B) and Attitudes (Section C) of the registered nurses towards pain management of adult medical patients. The questionnaire was given to experts i.e. Medical Surgical Nurses in the Health Sciences Department to assess content validity. A pilot study was carried out at Shamva Hospital with 10 registered nurses to ensure reliability of the instrument. No changes were made to the questionnaire after expert review and pilot study. The reliability of the instrument was 0.76 (Cronbach's α=0.76). Permission to carry out the study was sought from the Bindura University Research Ethics Board, Bindura Hospital Medical Superintendent and the Senior Nursing Officer. Data analysis was performed using the Statistical Package for Social Sciences (SPSS) version 16, 2012.
Results
Demographic data
The majority of the respondents 22(44%) were in the age category of 20-30 years. The mean age was 33.5 years with a standard deviation of 7.6 years. The majority of the respondents 39 (78%) had 1 to 10 years of experience. There were 49 (98%) diploma holders (Table 1).
Table 1: Demographic Data (n=50).
| Variable |
Frequency (n) |
Percentage (%) |
Age (years)
20 – 30 |
22 |
44.0 |
| 31 – 40 |
16 |
32.0 |
| 41 – 50 |
11 |
22.0 |
| 51 – 60 |
1 |
2.0 |
Sex
Female |
40 |
80.0 |
| Male |
10 |
20.0 |
Level in Nursing profession
Junior Nurse |
20 |
40.0 |
| Senior Nurse |
24 |
48.0 |
| Charge Nurse |
6 |
12.0 |
Highest academic qualification
Diploma in Nursing |
49 |
98.0 |
| BSc Nursing Science |
1 |
2.0 |
Years of Experience
1 – 10 |
39 |
78.0 |
| 11 – 20 |
9 |
18.0 |
| 21 – 30 |
2 |
4.0 |
| Total |
50 |
100.0 |
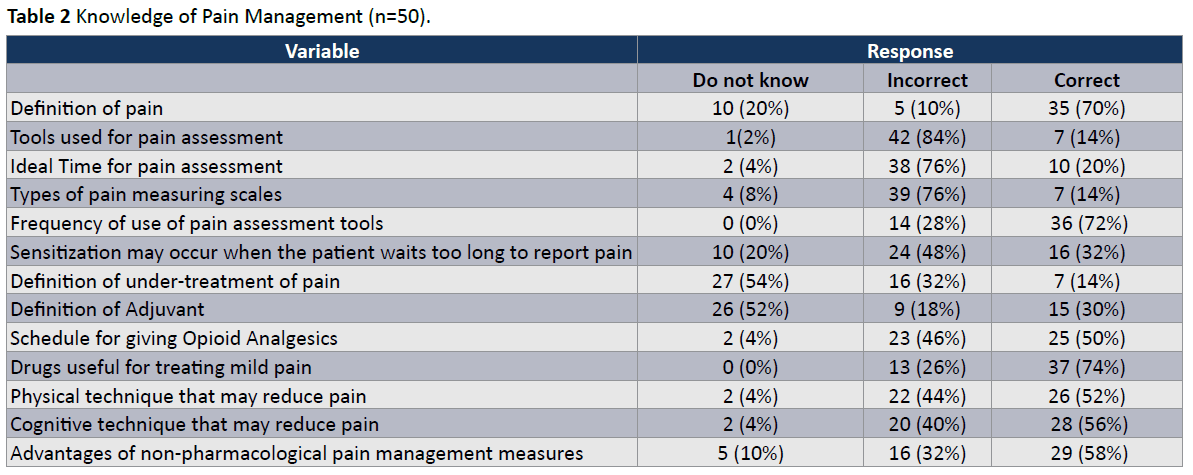
Knowledge of pain management
Ten (20%) of the respondents did not know the definition of pain whilst 5(10%) failed to define pain. Forty-two (84%) of the respondents failed to give correct tools used for pain assessment, 38 (76%) gave incorrect ideal time for pain assessment and 39 (76%) failed to identify types of pain measuring scales (Table 2). The majority of the respondents 36 (72%) correctly identified the frequency of use of pain assessment tools, 37 (74%) drugs useful for treating mild pain and 28 (56%) cognitive technique that may reduce pain. Furthermore, 27 (54%) of the respondent did not know the definition of under-treatment of pain and 26 (52%) did not know how to define an adjuvant. Twenty-nine (58%) of the respondents correctly identified the advantages of nonpharmacological pain management measures. Knowledge of pain management was associated with the age of the respondents (p=.001; p ≤ .005) with those of older (40 years and above) scoring high on the knowledge scores scale. There was also association between knowledge of pain management and one’s years of experience in the nursing profession (p=.003; p ≤ .005). However, knowledge of pain management was not associated with one’s level in the nursing profession (p=.325; p ≤ .005) and highest academic qualification attained (p=.467; p ≤ .005).
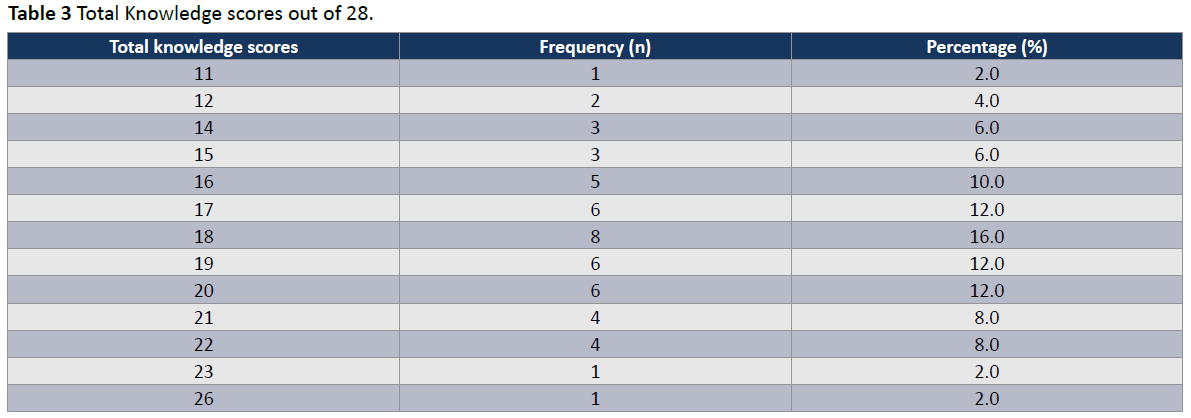
Knowledge scores
The total mean knowledge score was 64.5% with a range of 39.3- 92.9%. The majority of the respondents 29 (58%) had scores of 15 to 19, 14(28%) had scores of 20 to 23 and 6 (12%) had scores below 14 (Table 3). Only 2 (4%) had scores of 23 and 26 out the possible 28 which is above 80% of the total score while the majority 48 (86%) had scores below 80% of the maximum score. A score of 21 out of 28 (75%) was regarded as adequate knowledge and desirable score for this study according to the knowledge measuring instrument.
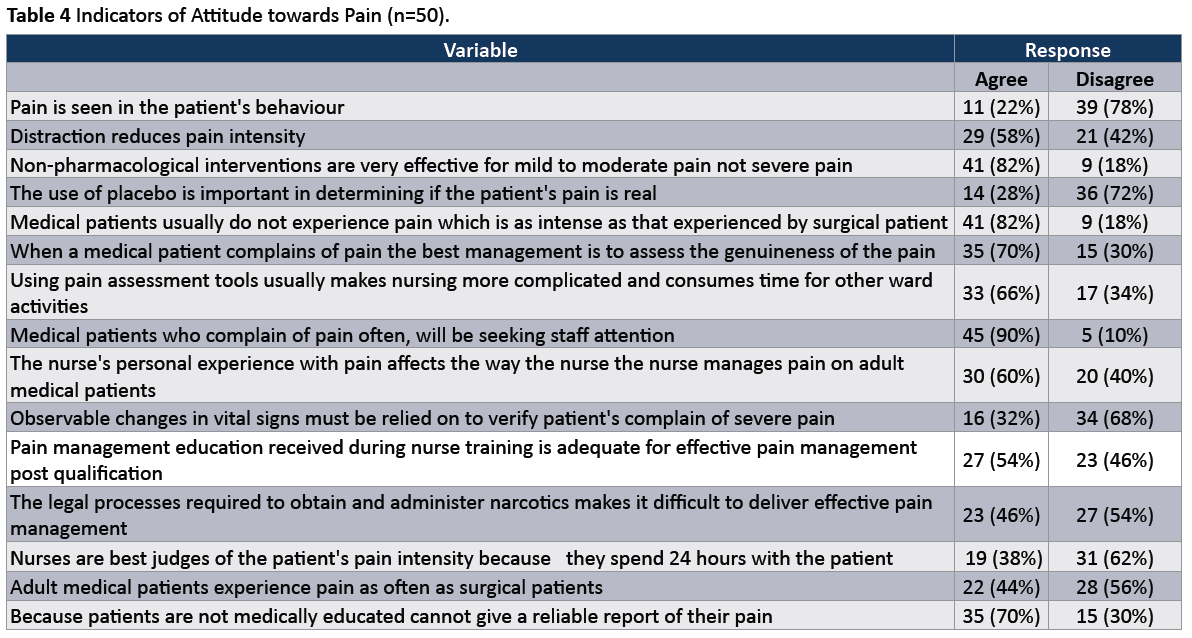
Attitude towards of pain
The majority of the respondents 29 (58%) agreed that distraction reduces pain intensity, 41 (82%) agreed that non-pharmacological interventions are very effective for mild to moderate pain not severe pain and 41 (82%) agreed that medical patients usually do not experience pain which is as intense as that experienced by surgical patients (Table 4). Thirty five(70%) of the respondents concurred with the idea that when a medical patient complains of pain the best management is to assess the genuineness of the pain and 45 (90%) agreed that medical patients who complain of pain often, will be seeking staff attention. Twenty-eight (56%) of the respondents disagreed with the idea that adult medical patients experience pain as often as surgical patients. The majority of the respondents 35 (70%) concurred with the fact that patients are not medically educated therefore they cannot give reliable report of their pain whilst 15 (30%) disagreed (Table 4).
Attitude scores
The total mean attitude score was 56% with a range score of 20-80%. Fifteen (30%) of the respondents had a score of 47% and below which is below the mean score of 50%. However, the majority of the respondents 35 (70%) had a score of 8 and above as shown in Table 5. Knowledge of pain management was highly associated with the nurses’ attitude towards pain management with a significant p-value (p=.000; p ≤ .005). A score of 12 out of the possible 15 (80%) was regarded as high and satisfactory for this study on the designed attitude measuring instrument.
Table 5: Total Attitude Scores out of a possible score of 15.
| Total Attitude Scores |
Frequency (n) |
Percentage (%) |
| 3 |
3 |
6.0 |
| 4 |
1 |
2.0 |
| 5 |
4 |
8.0 |
| 6 |
2 |
4.0 |
| 7 |
5 |
10.0 |
| 8 |
8 |
16.0 |
| 9 |
10 |
20.0 |
| 10 |
6 |
12.0 |
| 11 |
6 |
12.0 |
| 12 |
5 |
10.0 |
Discussion
This study provides important information about the level of knowledge and attitudes regarding pain management of registered nurses in Bindura, Zimbabwe. Nurses in this study had a mean total knowledge score of 64.5% (range=39.2-92.9%) and this is supported by findings in other studies that showed that nurses’ knowledge of pain management was poor ranging from 39.7 to 72.3 with knowledge score of pharmacology rarely exceeding 65% although criterion for minimally acceptable percentage score on the Nurses Knowledge and Attitude Survey Scale regarding pain management (NKAS) is 80% [1,3,5-7,9,11-13,16-18]. The mean total attitude score was 56% (range=20-80%) which is below what was found in other studies (range=66-82.34%).2’16 This means that the attitude of the studied nurses towards pain management of adult medical patients was very low. This is supported by a study done in Ethiopia [13].
The majority (84%) of the respondents failed to identify pain assessment tools and 76% failed to give the ideal time for pain assessment. This shows a gap in pain management because experts in pain management recommend that pain should be assessed as the fifth vital sign after blood pressure, pulse, respirations and temperature [5,7]. Contrary to other studies that showed that nurses scored lowest marks that rarely exceeded 65% particularly in pharmacological interventions of pain management, 74% of nurses in this study correctly identified drugs for treating mild pain [11,13,14].
Older respondents of 40 years and above scored high marks on the knowledge score scale indicating an association (p=.003; p ≤ .005). This is supported by a study done in Malaysia that also showed that age groups of more than 40 years had better knowledge on pain management (p=0.046) [2]. There was also an association between ye1ars of experience and knowledge on pain management (p=.003; p ≤ .005). This is supported by a study done in Hong Kong that showed that nurses with longer clinical working experience applied knowledge of pain to their daily practice [6,19]. However, other researchers found contradicting results which showed a negative correlation between knowledge score and demographic variables such as age and working experience [7]. This means as nurses grow older and their knowledge on pain management decreases. Other studies revealed that there was no significant difference in nurses’ pain knowledge among subgroups for variables such as nurses’ age groups, nursing experience years and ranks [5].
Only 50% of the nurses reported that opioids should be given around the clock on fixed schedules as prescribed. The other 50% of nurses either did not know how frequently opioids should be given or they gave wrong answers which included the administration of opioids when patient complains of pain. This could be supported by a study done in Central Africa in which 66% of the nurses admitted that they had some fears about administering morphine to patients. These nurses might not give the opioids as prescribed because they could be afraid of fostering patients’ addiction to opioids, respiratory distress and masking the patient’s symptoms [1,5,10,11,13].
The study also revealed knowledge deficit on non-pharmacological interventions to reduce pain as only 52% and 56% could identify physical and cognitive techniques respectively that may reduce pain. This is quite disturbing as nurses are said to have the key responsibility of providing non-pharmacological therapies to patients as adjuvant to pharmacological interventions to maximise relief of pain [15].
Eighty-two percent (82%) of the respondents agreed that medical patients usually do not experience pain which is as intense as that experienced by surgical patients, 90% concurred that when medical patients complain of pain they will be seeking staff attention. This in contradiction with Lui, So and Fong who reported that pain is a common symptom for patients in medical units and effective pain management strategies can relieve it effectively. Seventy percent (70%) of the nurses incorrectly agreed that patients are not medically trained hence cannot give reliable report of their pain. These findings are in line with findings in a study done by Voshall, Dunn and Shelestak in which nurses incorrectly reported that patients did not give reliable reports of their pain [5,9,20]. Such negativity or knowledge deficit can be a barrier to effective pain management.
Knowledge of pain management was highly associated with nurses’ attitudes towards pain management with a significant p-value (p=.000; p ≤ .005). These results show a positive correlation between knowledge and attitudes towards pain management that is, as the knowledge scores increases the attitudes towards pain management improves. Findings in a study done in Malaysia showed that attitude towards pain management was not significant (p ≤ 0.05) [2,17]. Miller found that nurses may have very positive attitudes towards pain management without sufficient knowledge to effectively manage pain. Nurses in the study done by Miller had higher mean attitude score of 82.34% and mean knowledge score of 72.3% [16].
Conclusion
Nurses’ knowledge and attitudes towards pain management was very low. This is a cause for concern since nurses play a pivotal role in pain management. Absence of pain is a basic human right therefore nurses need to be equipped with the necessary information so that they are able to effectively manage pain in adult medical patients. Continuing education organized by hospitals will have a significant impact on nurses’ knowledge and attitudes towards pain management.
6882
References
- Suha O, Mohammad Q, Nahla ALA, Mohammed FAH (2014) Knowledge and Attitudes about Pain Management: A Comparison of Oncology and Non-Oncology Jordanian Nurses. Nurs and Health 2: 73-80
- Ho SE, Ho CC, Pang Yuen H, Lexshimi R, Choy YC, et al. (2013) A study of knowledge and attitudes of registered nurses towards pain management in an urban hospital. ClinTer 164: 215-219.
- Yava A, Cizek H, Ozcan C, Yildiz D, Dizer B (2013) Knowledge and Attitudes of Nurses about Pain Management in Turkey. Int J of Car Sci6: 494-505
- Broekmans S, Vanderschueren S, Morlion B, Kumar A, Evers G (2004) Nurses' attitudes toward pain treatment with opioids: a survey in a Belgian university hospital. Int J Nurs Stud 41: 183-189.
- Alexandrina de Jesus SL, Jacinta PM (2013) Pain: Knowledge and attitudes of nursing students, 1 year follow-up. Text Context Nurs22: 311-317
- Lui LY, So WK, Fong DY (2008) Knowledge and attitudes regarding pain management among nurses in Hong Kong medical units. J ClinNurs 17: 2014-2021.
- Ekim A, Ocakc A (2012) Knowledge and attitudes regarding pain management of paediatric nurses in Turkey. Pain ManagNurs16: 14-18
- Clarke KA, Iphofen R (2008) The effects of failing to believe patients’ experience of chronic pain. Nursing Times 104: 30-31
- Bernardi M, Catania G, Lambert A, Tridello G, Luzzani M (2007) Knowledge and attitudes about cancer pain management: a national survey of Italian oncology nurses. Eur J OncolNurs 11: 272-279.
- Bernhofer E (2011) Ethics and Pain Management in Hospitalized Patients" OJIN: Online JIssues Nurs 17
- Jho HJ, Kim Y, Kong KA, Kim DH, Choi JY, et al. (2014) Knowledge, practices, and perceived barriers regarding cancer pain management among physicians and nurses in Korea: a nationwide multicenter survey. PLoS One 9: e105900.
- Deandrea S, Montanari M, Moja L, Apolone G (2008) Prevalence of undertreatment in cancer pain. A review of published literature. Ann Oncol 19: 1985-1991.
- Kassa RN, Kassa GM (2014) Nurses’ Attitude, Practice and Barriers toward Cancer Pain Management, Addis Ababa, Ethiopia. J Cancer SciTher 6: 483-487
- Samuels JG, Fetzer SJ (2009) Evidence-based pain management: analyzing the practice environment and clinical expertise. Clin Nurse Spec 23: 245-251.
- Bicek E (2004) Nurses' Attitudes, Knowledge, and Use of Nonpharmalogical Pain Management Techniques and Therapies. Honors Projects, Paper 12
- Miller A (2012) Hospice Nurses - Attitudes and Knowledge about Pain Management. A thesis submitted in partial fulfilment of the requirements for the degree of Masters of Science in Nursing College of Nursing. University of South Florida, USA
- Rampanjato RM, Florence M, Patrick NC, Finucane BT (2007) Factors influencing pain management by nurses in emergency departments in Central Africa. Emerg Med J 24: 475-476.
- Kaki AM (2011) Medical students’ knowledge and attitude towards cancer management in Saudi Arabia. Saudi Med J 32: 628-632
- Tse MM, Ho SS2 (2014) Enhancing knowledge and attitudes in pain management: a pain management education program for nursing home staff. Pain ManagNurs 15: 2-11.
- Voshall B, Dunn KS, Shelestak D (2013) Knowledge and attitudes of pain management among nursing faculty. Pain ManagNurs 14: e226-235.

