Keywords
HIV/AIDS, Cyprus, nursing care code of ethics, human rights, immigrants
Introduction
Cultural, social policy and legal factors contribute to HIV vulnerability among migrant populations. Limited knowledge on HIV increases vulnerability as well as negative social attitudes and services that are not culturally sensitive and lack of culturally competent health professionals [1]. Migrants worldwide has increased over the last 10 years from an estimated 150 million in 2000 to 214 million persons today [2]. In 2010 about 10765 foreign students were studying in Cyprus, coming mainly from Third countries [3,4].
Migration into and within Europe has implications for public health including provision of HIV services for migrant populations [1]. The key factors that prevent migrants for accessing HIV services in relation to prevention are amongst others: a) lack of information about existing services and fear of stigma and discrimination, b) lack of culturally sensitive interventions, c) linguistic problems, c) marginalization and exclusion, d) legal obstacles, e) cultural and religious factors and e) migration policies [1].
Among the 66,000 third country nationals residing legally in Cyprus, more than 20,000 are domestic workers and a significant number of them is undocumented [5,6].
In Cyprus, only emergency care is available free of charge. female migrant domestic workers, have to contribute 50% of the cost of their private medical insurance, which does not cover gynecological and delivery care. Thus, their health is at risk and access to antenatal and postnatal care is limited [5].
A study on migrant domestic workers, [7] on utilization and access to private and public health care services in Cyprus showed that the employer had the role of gate-keeper and some of the women were facing lack of autonomy and were dependent on their employer. Lack of information on health care services were a factor stressed leading to risky sexual behaviors [7]. Another local study on sexual and reproductive needs of female migrant domestic workers, found that when contraception used by domestic workers, this was based on previous experience such as coitus interruptus, meaning that most of the participants were involved in risky sexual behavior. Although that participants showed familiarity with methods of contraception they did not show awareness of their causes of prevention [6]. In another relevant study in India on HIV/AIDS prevention differences were found amongst gender and place of resident (urban or rural), with women and participants of rural areas having lower knowledge of transmission and prevention of HIV [8].
The implication of nursing ethics to healthcare
Nurses, as care providers can contribute to resolve health problems and help immigrants to adjust in a new way of life [9] by: a) dispel myths and misinformation, b) advocating for access to prevention, c) safeguarding human rights, d) organize information campaigns, e) mobilizing community resources, f) targeting vulnerable populations at high risk of infection and g) promoting a continuum of care [10-12]. The Swedish Society of Nursing [13] encourages nurses to defend the right to healthcare of migrants without legal status and takes active part in lobbying for new legislation that does not discriminate against these migrants. The Nursing and Midwifery Council code of conduct [14-16] implies that nurses should treat people as individuals and respect their dignity (act as an advocate, helping people to access relevant health and social care, information and support), respect people’s confidentiality (ensure people are informed about how and why information is shared by those who will be providing their care) and share information in an understandable manner [14-16].
Methods and Material
The current study explored the: knowledge, perceptions and behavior of immigrants and foreign students living in Cyprus on HIV/AIDS and sexual reproductive health.
Study Design
The current study is a quantitative study using a self-completed questionnaire with the use of a closed-ended questionnaire based on literature review.
Sample and Sampling
Data were collected from 600 immigrants using a snowball sample, a non probability method of sampling. Participants were collected from two common gathering places in the two biggest cities of Cyprus (Nicosia and Limassol). The inclusion criteria were: a) 18 years of age and older, b) able to read and comprehend English language, c) legal domestic worker that were employed in Cypriot households or foreign student that came to Cyprus with a student permit for studying in tertiary education and registered in the relevant register of the Cypriot Ministry of Education and Culture or e) immigrants from third countries that reside and live in Cyprus. f) Participant’s willingness to participate. Both men and women were included in the study sample. Exclusion criteria were applied for refugees and illegal migrants. The response rate was 80%. Tool
The closed questionnaire was based on literature review [6,9,17-18] and included four parts: a) General Information (Demographics), b) Knowledge (modes of HIV transmission), c) Attitudes (transmission myths, how they perceive the HIV/AIDS and their consequences) and d) behavior (risky sexual behaviour, HIV related behaviours and condom use). It was self administered. Knowledge was assessed through 12 items on modes of transmission and 9 items on ways of reducing or preventing transmission. Attitudes was assessed using an 11-item on attitudes toward HIV/.AIDS and people having HIV/AIDS whereas Behavior was assessed through 28 items and exemplified questions related to unprotected sex and other risky sexual behaviours. The questionnaire was examined for validity by a group of experts and had proved that it had content validity. Cronbach’s coefficient alpha was found to be a=0.74.
A pilot study was applied in 3 migrant student and 3 domestic workers noting no major problems. The time of completing the questionnaire was 30 to 45 minutes.
In regards to scoring; For Knowledge, each right response was given a score of 1 while a not true or unsure was scored 2 and 3. Attitudes/Perceptions towards HIV/AIDS were assessed through a 6 level Likert scale. Risky sexual behaviours were assessed through 17 questions related to risky sexual behaviours indicating yes or no questions or true or false.
Data collection and analysis
Collection of the data took four months (December 2009-March 2010). The questionnaires were distributed and collected on weekends (as these were the free days of the participants) from two common gathering areas of migrants in Cyprus. Two members of the research team personally distributed the questionnaire and remained and at a significant spot at the same area and participants returned the questionnaire thrown in a box within 30-45 minutes. The analysis was performed with the use of the SPSS version 16. Demographic distribution was described through frequency and percentage, whereas chi-square tests and pearson correlations were used.
Ethical Issues
Prior to data collection, all study participants were informed with a covering letter on the aims and scope of the current study and were assured of confidentiality and anonymity based on the Cyprus article 6 (h) of the Legislation of Personal Data (Protection of Individuals) Law 138 (1) 2001: indicating that processing of the data is performed solely for statistical and research purposes on condition that all necessary measures were taken for the protection of the data participants and to article 11 (1) of the same legislation participants were informed for the purpose of the study prior their participation [21]. Further, ethical principles drafted by Belmont Report (1979) were applied throughout the whole study [19].
Results
Demographics
Most of the participants were males (62.7%), whereas 37.3% were females. Participants were mainly coming from Philippines 21% and their ages ranged from 21-25 (43.2%) and from 26-30 (30.1%). Participants were mainly residing in Famagusta area (33.3%), as well as Nicosia area (22.2%). As far as their level of education is concerned, 72.7% of the participants had a college or university degree, whereas 24.5% reported to work as domestic workers. Participants’ family situation is described as single (74.4%) or married (21.6%). The question in relation to their sexual behavior revealed that 27.8% had occasional sexual partners during their stay in Cyprus, 27.6% had sex only with their partner when in their country whereas 25.6% had a stable sexual partner in Cyprus. Further, 18.3% of the participants reported having a child.
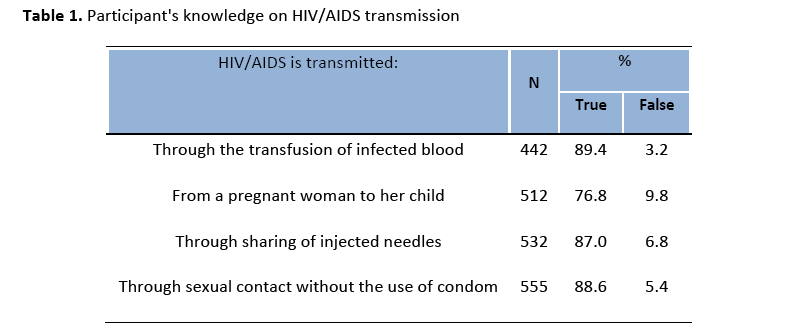
Knowledge
Regarding knowledge, 21.4% believed that HIV/AIDS is transmitted while eating with an HIV infected person. Knowledge in relation to transmission while eating with an HIV infected person was significantly higher amongst men than women (p=0.000). In relation to transmission through sexual contact without the use of condom was significantly higher in relation to men than women (p=0.03). As far as the current occupation is concerned, it was interesting to note that farmers and salespersons, gave a positive answer to the transmission of HIV while eating with an HIV infected person (p=0.000). A negative response was given by 70.0% of the participants in the question whether HIV is transmitted through the use of common households (Table 1). In relation to gender, more men (77.9%) than women (54.5%) found the statement not true (p=0.000). It is important to note that 48.5% of the participants answered that the risk of infection from HIV may be reduced or prevented by not having sex; and was significantly higher amongst men (p=0.000) whereas 83.9% of the participants stated that the risk of infection from HIV may be reduced or prevented by avoiding shared needles. As far as the knowledge in relation to current occupation, only students, gardeners and participants that were not working gave a correct answer in relation to the reduction or prevention of HIV by not having sex (p=.000).
At this point, is also significant to note that in relation to the statement concerning the reduction or prevention of HIV by avoiding the company of HIV infected people men responses were significantly higher than women (p=0.000) as well as students, waitresses gardeners and cooks.
Perceptions
As far as their perceptions on HIV/AIDS and sexual reproductive health, 27.8% of the participants strongly disagree with the statement ‘individuals with AIDS got what they deserved’. It is interesting that, students reported that they strongly agree with the above statement in relation to other occupations (p=.000), whereas 44% of the participants strongly disagree that ‘individuals with AIDS should be isolated away from the society’. It is important to note that 41.7% of the participants agree that they could be a friend with a person with AIDS. More women than men agree that they could be friends with a person with AIDS (p=.000). As far as the current occupation is concerned in relation to perceptions about being a friend with a person who has AIDS responses of farmers, gardeners and participants that are not working where significantly higher than other occupations (p=0.000). Further, 39.5% of the participants completely disagree with the statement that ‘the government shouldn’t provide HIV people free medical care’, 21.2% of the participants completely agree with this (Table 2).
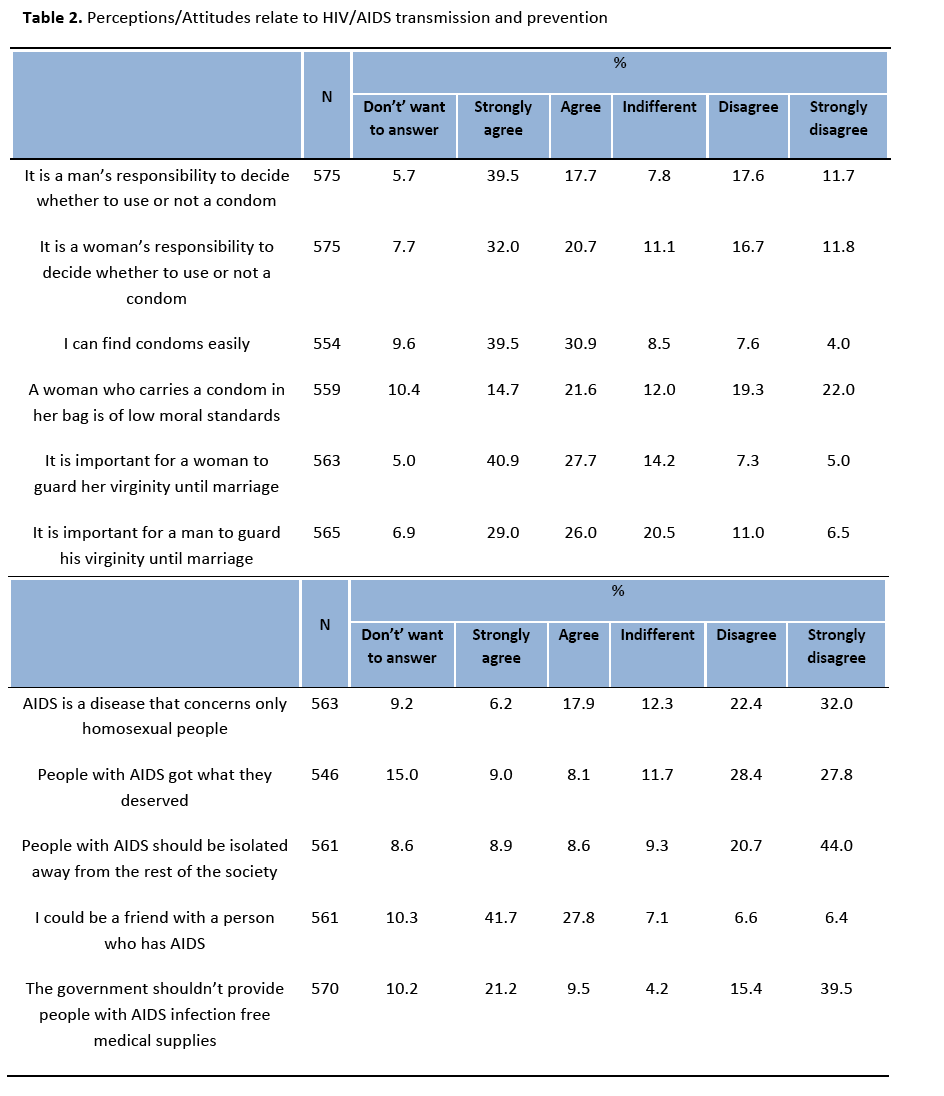
Farmers where found to strongly agree with the above statement (p=.000) and men found to respond higher than women in relation to above statement (p=.000). More men that women strongly disagree with the statement that HIV is a disease that concerns only homosexual people (p=.000). Men seem to respond significantly higher as well to the statement: people with AIDS got what they deserved (p=.041), the same occurred for the statement: people with AIDS should be isolated away from the rest of the society (p=.000). Statistically significance was also found between the country of origin and attitude of the participants (p=.000). Participants coming from Pakistan, China and South Africa either agree or strongly agree that AIDS is a disease that concerns only homosexual people whereas participants coming from Philippines, Vietnam, Lebanon, Kenya, Iran, Cameroun and Georgia disagree with the above statement. As far as the statement: people with AIDS got what they deserve participants from India, Pakistan, Bangladesh, China, Ukraine, Kenya, Iran, Cameroun, Japan, Georgia and Zimbabwe disagree or strongly disagree with the above statement (p=.000). Participants coming from Vietnam, S. Africa and Lebanon either strongly agree or agree with the statement: people with AIDS should be isolated away from the rest of the society, statistical significance amongst the country of origin and the above statement showed p=.000). Moreover, statistical significant correlations were found amongst country of origin and attitude concerning the statement: I could be a friend with a person who has AIDS (p=.000). Participants coming from India, Pakistan, Bangladesh, Nepal, Sri Lanka, S. Africa, Kenya, Russia, Nigeria, America, and Zimbabwe were either strongly agree or agree with the above statement. Further, the correlation between country of origin and the statement the government shouldn’t provide people with AIDS infection free medical supplies (such as medication) only participants coming from India, Sri-Lanka, South Africa and Kenya either agreed or strongly agreed with the above statement.
Behavior
Regarding sexual activity, 62.4% reported to be sexually active in Cyprus. Further, 10.0% of the participants had sex with a person of the same sex and 9.2% of the participants reported having sex against their will. The majority of the participants (86.0%) reported that they were not driven to risky sexual behavior because of alcohol drinking. However, 3.2% of the participants reported having a sexual partner that had used intravenous drugs. Also, 9.3% of the participants reported being engaged in group sexual activities.
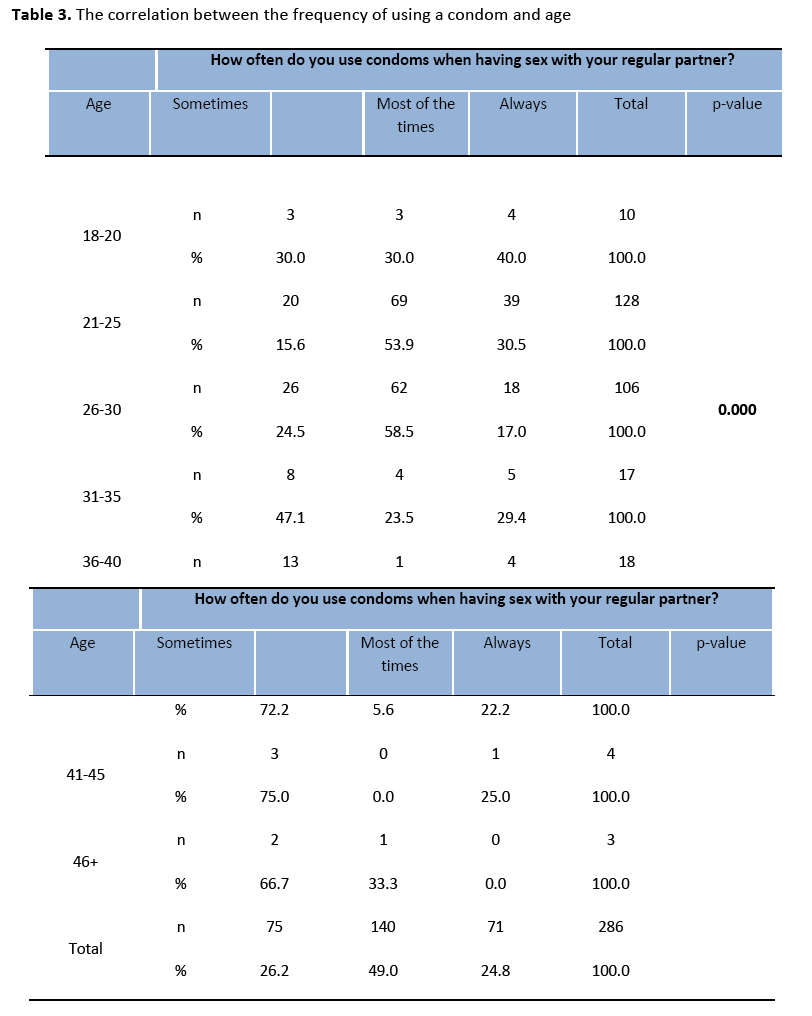
As far as the reasons of not using a condom during their last sexual intercourse with their regular partner 14.7% of the participants reported of not having thought of it; whereas 11% had used other methods of contraception’s. Further, 49% of the participants reported using condom most of the times; whereas 26.2% reported using a condom sometimes. It is important to note that 44% of the participants had sex with other person/s while being with their regular partner and 10.5% of them reported that they had not used condom since condom reduces pleasure. Further, more men than women found to be using condoms with their regular partner (p=.000). Men found responding higher that they have had sex with other persons than their regular partners (p=.000). As far as the level of education participants with a doctorate responded that they did not use a condom during the last sexual intercourse with their regular partner (p=.004). Statistical significance correlations were also found between the level of education and the reasons of not using a condom (p=.000). College/University students responded higher that condom decreases the pleasure (66.7%) whereas participants with primary education on their majority (100%) were not using a condom due to the fact that they didn’t know how to use it and master students (50%) indicated that they were using other methods of contraception’s. It was also interesting to found that a combination of reasons (didn’t think about it and we were under the influence of drugs) was an indication for not using condoms within College/University students. As far as the responses for behavior in relation to age of the respondents significant correlations were found in the statement of positive use of a condom during the last sexual intercourse with their regular partner (p=.000) between younger ages 18-20 (57.9%), 21-25(77.3%) and 26-30(68.8%) (Table 3). Significant correlation was also found between age and the frequency of using condoms when having sex with their regular partner (p=.000), where younger ages, 18-20 indicate that they were always using a condom (40.0%), 21-25(54.9%). Younger ages (18-20, 21-25 and 26-30) were also found to be using condoms during the last sexual intercourse with a person/s other than their regular partners in relation to older ages 31-35, 36-40, 41-45 and 46+ (p=.000). The same occurred as far as the frequency of using a condom with a person other than their regular partner with younger ages using a condom always and only participants 46+ using a condom most of the times (p=.000). Singles were found to be using a condom during their sexual intercourse with their regular partner than participants with other family situation (p=.000). The same occurred for family situation in relation to using a condom during their sexual intercourse with a person other than their regular partner (p=.000), singles were using a condom. In relation to country of origin and condom use during the last sexual intercourse with the regular partner statistically significant correlations found (p=.000). Participants coming from Philippines, Vietnam, Iran, Cameroun, Afganistan, Georgia, Nigeria and other were not using condoms while having sex with their regular partners. As far as the question concerning having sex with other person/s while being with their regular partner, participants coming from Zimbabwe, Bangladesh, Pakistan and India gave a positive answer, statistical significance was found (p=.000). Participants coming from those countries reported that they were using a condom. Furthermore, participants coming from Vietnam (100%), Philippines (79.3%) and Sri Lanka (71.4%) reported that they were not using a condom during the last sexual intercourse with a person/s other than their regular partner (p=.000). Only participants coming from Afghanistan (100%) and China (57.1%) were driven to risky sexual behavior because of alcohol drinking.
Discussion
In relation to modes of transmission, 21.4% of the participants believed that HIV/AIDS is transmitted while eating with an HIV infected person. A statistically significant finding in relation to the knowledge of men than women.
Overall, participants seem to practice risky sexual behaviors, such as having unprotected sex, this was found to be higher in men than women. Findings from the current study are in line with results of the two other local researches in relation to domestic workers conducted in Cyprus [6,7]. Further, abstinence from sex was suggested by 48.5% of the participants as a method for reducing or preventing the risk of infection and was significantly higher amongst men. The current study results seem to be in line with the results of the study of Tanaka et al., [20] where males 93.5% accredited the significance of abstinence for the reduction and prevention of HIV/AIDS.
Men found to be reporting higher that they had sex with other persons than their regular partners. However, in the study of Tanaka et al., [20] it was found that women having sex more regularly with other persons than their regular partners and were found to be less willing to use condoms in general. At this point authors suggest that cultural and religious factors play a significant role in practicing safe sex methods. In the He et al. study, although migrants seemed to have some knowledge on HIV, findings emphasized the need to promote safer sex and health services accessibility and use among migrants [21].
Despite the results of the current study and other studies mentioned in this paper, Thu et al study in Thailand showed that there were misconceptions on prevention of HIV/AIDS; however no statistically significant association between knowledge and condom use, but a positive attitude was associated with safe practice [22]. Moreover, participants and especially men and students reported to avoid the company of HIV infected people as a mean to prevent or reduce the infection. Participants strongly agree that “individuals with AIDS got what they deserved” in relation to other participants. Lack of knowledge contributes to isolation of people living with HIV and one might have been expected that young participants would have been more aware of the modes of transmission. Researchers postulate their knowledge, attitudes and perceptions is a combination of the cultural, religious and political factors, rather than epistemological knowledge itself. Similar findings reported in two other studies [23-24].
In the Fitzgerald et al., [24] study on migrant workers in the USA the majority of women had a good general knowledge of HIV transmission, however authors stated the need of further prevention education specifically on perinatal transmission. One of the major challenges currently facing western Europe is to prevent the relaxation of safer sex practices, to improve access to HIV testing and care for all, especially migrants coming from countries with generalized epidemics [26].
Limitations
The current study included only ethnic minorities such as foreign students and migrant domestic workers and one can imply that the recommendations made are only to be applied in this group of population only and not to be generalized to the broader migrant population.
Conclusion
Participants of the current study lack the substantial knowledge and hold misbelieves on issues related to HIV/AIDS or STI’s in general and this leads them to risky sexual behaviors. The results, suggest that health providers need to design effective policies for the health of foreign students and immigrants that live in Cyprus.
There is the need for provision of guidance on training and clinical practice for health professions in provision of culturally-sensitive prevention and care services and for development of culturally appropriate materials; as well as the development for good clinical practice in line with the nursing code of ethics that take into account of the specific needs of migrants and respect diversity.
The development of a Public Health Legislation, as well as the empowerment of public health authorities for providing prevention services that would be accessible to those ethnic minorities is strongly supported also by the guidelines prepared on HIV/AIDS on Human Rights, by UNAIDS and the Office of the High Commissioner for Human Rights.
Nurses should be trained for the provision of culturally sensitive care, prevention and protection of health. There is a need to incorporate migrant health protection and equitable access to care into mainstream health policies. Nursing organizations should act as advocates and health promoters in preventing HIV/AIDS and sexually transmitted infections in line with their codes of ethics.
Acknowledgments
We would like to deeply thank the Cyprus Ministry of Health that funded the current project as well as Mrs. Christiana Dipli for participating in the data collection phase as well as within the Statistical analysis of the current project. We would also like to thank Cyprus Family Planning Association and Research Unit in Behaviour and Social Issues that contributed in order for the project to be fulfilled.
2944
References
- European Centre for Disease Prevention and Control. ECDC Technical Report. Migrant health: Access to HIV prevention, treatment and care for migrant populations in EU/EEA countries. Stockholm, 2006. Available at website: https://ecdc.europa.eu/en/publications/Publications/0907_TER_Migrant_health_HIV_Access_to_treatment.pdf. June 26, 2012.
- United Nations Trends in Total Migrant Stock: The 2008 Revision. Available at: https://esa.un.org/migration/. Accessed April 9, 2012.
- Cyprus Ministry of Education and Culture. National Report. Cyprus, 2010. Available at website: https://www.moec.gov.cy/etisia-ekthesi/pdf/Annual_report_2010_GR.pdf. Accessed April 9, 2012
- Cyprus Civil Registry and Migration Department. Alien Students. Cyprus, 2011. Available at website: https://www.cyprus.gov.cy/moi/citizenscharter/citizenscha rter.nsf/dmlstudents_en/dmlstudents_en?OpenDocument Accessed 10/1/ 2013
- Health for Undocumented Migrants and Asylum Seekers .Access to Healthcare and Living Conditions of Asylum Seekers and Undocumented Migrants in Cyprus, Malta, Poland and Romania. 2009. Available at website: https://www.december18.net/article/new-huma-report-cyprus-malta-poland-romania Accessed April 9, 2012.
- Kouta C, Kaite C, Kalavana TH. Migrant domestic workers in Cyprus: An evaluation of their sexual and reproductive health needs. A pilot study. Hellenic Journal of Nursing Science 2011; 4(2): 19-31.
- Theodorou MH, Pithara C, Konstantinou A, Kantaris M. Utilization and access to private and public health care services by domestic workers in Cyprus: Mapping inequalities and discrimination. Paper presented during the Gender Equality and Women?s Empowerment Conference, Nicosia, Cyprus; October 23 2010.
- Hazarika I. Knowledge, attitude, beliefs and practices in HIV/AIDS in India: Identifying the gender and rural-urban differences. Asian Pacific Journal of Tropical Medicine 2010; 821-827.
- Tung WC, Hu J, Davis C, Tung WK, Lin YM. Knowledge, attitudes and behaviors related to HIV and AIDS among female college students in Taiwan. Journal of Human Behavior in the Social Environment 2008; 17(3/4): 361-375.
- General Assembly of the United Nations. The Universal Declaration of Human Rights (art.25). 1948.
- UNAIDS and Office of High Commissioner for Human Rights. International Guidelines on HIV/AIDS and Human Rights. 2006. Available at website: https://data.unaids.org/Publications/IRC-pub07/jc1252-internguidelines_en.pdf. Accessed April 9, 2012.
- International Council of Nurses Position Statement. Health Services for migrants, refugees and displaced persons. 2006. Available at: https://www.icn.ch/images/stories/documents/publications/position_statements/A06_Healh_Migrants_Refugees.pdf. Accessed December 9, 2012
- Swedish Society of Nursing. Foundation of Nursing Care Values. 2010. Available at website: https://www.swenurse.se/Global/SSF%20Bilder/Etik/Foundation.Of.Nursing.Care.Values.pdf. Accessed April 9, 2012.
- The International Council of Nurses Codes of Ethics. Geneva, Switzerland, 2000. Available
- International Council of Nurses Fact Sheet. Mobilizing Nurses for HIV/AIDS Prevention and Care. 2009.
- Nursing and Midwifery Council code of Conduct. 2008. Available at website: https://www.nmc-uk.org/Nurses-and-midwives/The-code/The-code-in-full/.Accessed 9/4/2012
- Maimaiti N, Shamsuddin A, Tohti A, Memet R. Knowledge, Attitude and Practice Regarding HIV/AIDS among University Students in Xinjiang. Global Journal of Health Science 2010; 2(2):51-60.
- Drummond PD, Mizan A, Wright B. HIV/AIDS knowledge and attitudes among West African immigrant women in Western Australia. Sexual Health 2008;5 (3) 251-259.
- The Belmont Report. Ethical Principles and Guidelines for the Protection of Human Subjects of Research. 1979 [Online] Available at: https://www.emerson.edu/graduate_studies/upload/belmontreport.pdf Accessed 16/06/2012
- Tanaka Y, Kunii O, Hatano T, Wakai S. Knowledge, attitude and practice (KAP) of HIV prevention and HIV infection risks among Congolese refugees in Tanzania. Health and Place 2008; 434-452.
- He N, Zhang J, Yao J, Tian X, Zhao G, Jiang Q, Detels R. Knowledge, attitudes, and practices of voluntary HIV counseling and testing among rural migrants in Shanghai, China. AIDS Education Prevention. 2009; 21(6):570-81.
- Thu M, Kyu H.H, Van der PuttenM.Assessing knowledge, attitudes and practices on HIV-AIDS prevention among Myanmar migrant workers: A case study in Mahachai, SamutSakhon province, Thailand. Journal of Technology 2005; 8(3):131-134.
- Gagnon AJ, Merry L, Bocking J, Rosenberg E,Martinez-Oxman J. Knowledge, attitudes and practices and the role of sexual power. Health and Place 2010;16(1) :10-15.
- Ferrer L, Clanelli R, Guzman E, Cableses B, Irrarazabal L, Bernales M, Araya A. Chilean University Students: Knowledge and Concern about HIV/AIDS. Journal of the Association of Nurses in Aids and Care 2007; 18(5):51-56.
- Fitzgerald K, Chakraborty J, Shah T, Khuder S, Duggan J. HIV/AIDS knowledge among female migrant farm workers in the Midwest. Journal of Immigrant Health. 2003; 5(1):29-36.
- WHO, HIV/AIDS in Europe. Moving from death sentence to chronic disease management 2010.

