Ridhaa Mohammed Hasan Al-Saadawi and Abeer Gatea*
Department of Epidemiology and Biostatistics, School of Public Health, Tehran University of Medical Sciences, Tehran, Iraq
*Corresponding Author:
Abeer Gatea
Department of Epidemiology and Biostatistics
School of Public Health, Tehran University of Medical Sciences
Tehran, Iraq
Tel: +0096 4772 3212 850
E-mail: abeergatea@hotmail.com
Received date: 01 September 2018; Accepted date: 05 February 2019; Published date: 12 February 2019
Citation: Al-Saadawi RMH, Gatea A (2019) Knowledge of People about the Tuberculosis Infection in the Health Center in Baghdad. Health Sci J Vol.13.No.1:623. DOI: 10.21767/1791-809X.1000623
Copyright: © 2019 Al-Saadawi RMH, et al. This is an open-access article distributed under the terms of the creative commons attribution license, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Keywords
TB; Knowledge; Program; Significant; Center
Introduction
Tuberculosis is the second-most common cause of death from infectious disease (after those due to HIV/AIDS) [1]. Roughly one-third of the world's population has been infected with M. tuberculosis [2]. With new infections occurring in about 1% of the population each year [3]. However, most infections with M. tuberculosis do not cause TB disease [4], and 90-95% of infections remain asymptomatic [5]. In 2012, an estimated 8.6 million chronic cases were active [6]. In 2010, 8.8 million new cases of TB were diagnosed and 1.20–1.45 million deaths occurred, most of these occurring in developing countries [7,8]. Of these 1.45 million deaths, about 0.35 million occur in those also infected with HIV [9]. China has achieved particularly dramatic progress, with about an 80% reduction in its TB mortality rate between 1990 and 2010 [9]. The number of new cases has declined by 17% between 2004– 2014 [10]. Tuberculosis is more common in developing countries; about 80% of the population in many Asian and African countries test positive in tuberculin tests, while only 5– 10% of the US population test positive [11]. Hopes of totally controlling the disease have been dramatically dampened because of a number of factors, including the difficulty of developing an effective vaccine, the expensive and timeconsuming diagnostic process, the necessity of many months of treatment, the increase in HIV-associated tuberculosis, and the emergence of drug-resistant cases in the 1980s [12]. The rates of TB vary with age. In Africa, it primarily affects adolescents and young adults [13]. However, in countries where incidence rates have declined dramatically (such as the United States), TB is mainly a disease of older people and the immune compromised (risk factors are listed above) [14]. Worldwide, 22 "high-burden" states or countries together experience 80% of cases as well as 83% of deaths [10]. The aim of this study to identify the knowledge of people about the TB disease in the health center and to find out any relationships between demographic characteristic and knowledge of people.
Methods
A cross-sectional study was conducted at one of the health centers of Baghdad Health Department in Al-Rusafa in the Sheikh Omar area for the period from January to 2018. The sample size was 150 people who reviewed the center for treatment and diagnosis. This health center is a public center that provides services for women, children and the elderly. It also has a special section for men. Samples were collected through a pre-prepared questionnaire containing demographic information and the interview was conducted directly with the auditor. The data analysis through descriptive (frequency, percent, p- value).
Results
Out of 150 participants, 107/150 (71.3%) still in the age groups 20-24 years, the female cases 79/150 (52.7%) were higher more than the male cases 71/150 (47.3%). Regarding the distribution of the visitors to the sections of the center, the highest percentage 42/150 (28%) of the vaccine room followed by the physician room 34/150 (22.7%). The table shows that the highly significant relationship have been found between the scientific department and overall knowledge assessments p=0.004 (Table 1).
Table 1 Relationship among socio-demographical characteristics variables and overall knowledge assessments.
| Var. |
Groups |
No. and Percent |
Overall Assessment |
C.S. |
| Under |
Upper |
CC=0.186
P=0.145
NS |
| Age Groups |
<20 |
No. |
13 |
6 |
| % Age Groups |
68.40% |
31.60% |
| % Overall Assessment |
17.10% |
8.10% |
| 20-24 |
No. |
55 |
52 |
| % Age Groups |
51.40% |
48.60% |
| % Overall Assessment |
72.40% |
70.30% |
| 25-29 |
No. |
6 |
11 |
| % Age Groups |
35.30% |
64.70% |
| % Overall Assessment |
7.90% |
14.90% |
| 30 ≥ |
No. |
2 |
5 |
| % Age Groups |
28.60% |
71.40% |
| % Overall Assessment |
2.60% |
6.80% |
| Gender |
Male |
No. |
35 |
36 |
CC=0.026
P=0.750
NS |
| % gender |
49.30% |
50.70% |
| % Overall Assessment |
46.10% |
48.60% |
| Female |
No. |
41 |
38 |
| % gender |
51.90% |
48.10% |
| % Overall Assessment |
53.90% |
51.40% |
| Department |
Physician room |
No. |
19 |
15 |
CC=0.338
P=0.004
HS |
| % Scientific Department |
55.90% |
44.10% |
| % Overall Assessment |
25.00% |
20.30% |
| Physical room |
No. |
8 |
8 |
| % Scientific Department |
50.00% |
50.00% |
| % Overall Assessment |
10.50% |
10.80% |
| Radiology |
No. |
7 |
8 |
| Room |
% Scientific Department |
46.70% |
53.30% |
| % Overall Assessment |
9.20% |
10.80% |
| Optic room |
No. |
12 |
3 |
| % Scientific Department |
80.00% |
20.00% |
| % Overall Assessment |
15.80% |
4.10% |
| Vaccine Room |
No. |
11 |
31 |
| % Scientific Department |
26.20% |
73.80% |
| % Overall Assessment |
14.50% |
41.90% |
| Dental room |
No. |
11 |
4 |
| % Scientific Department |
73.30% |
26.70% |
| % Overall Assessment |
14.50% |
5.40% |
| Lab. Room |
No. |
8 |
5 |
| % Scientific Department |
61.50% |
38.50% |
| % Overall Assessment |
10.50% |
6.80% |
CS: Cross Sectional Study, P: P-value, NS: Non-significant, HS: Highly Significant
Regarding of marital status, there is no any relation between the marital status and overall knowledge assessment at the value <0.05. For monthly income, the highest percentage was 48% for those with a moderate income. Also, in this the table shows that there is no relationship between the income and knowledge assessment at the value <0.05 (Table 2).
Table 2 Relationship among socio-demographical characteristics variables and overall knowledge assessments.
| Variable |
Groups |
No. and Percent's |
Overall Assessment |
CS |
| Under |
Upper |
| Marital Status |
Single |
No. |
65 |
56 |
CC=0.211
P=0.073
NS |
| % marital status |
53.70% |
46.30% |
| % Overall Assessment |
85.50% |
75.70% |
| Married |
No. |
7 |
16 |
| % marital status |
30.40% |
69.60% |
| % Overall Assessment |
9.20% |
21.60% |
| Divorcee |
No. |
4 |
1 |
| % marital status |
80.00% |
20.00% |
| % Overall Assessment |
5.30% |
1.40% |
| Widow |
No. |
0 |
1 |
| % marital status |
0.00% |
100.00% |
| % Overall Assessment |
0.00% |
1.40% |
| Monthly Income |
Good |
No. |
29 |
32 |
CC=0.888
P=0.777
NS |
| % Monthly Income |
47.50% |
52.50% |
| % Overall Assessment |
38.20% |
43.20% |
| Moderate |
No. |
36 |
36 |
| % Monthly Income |
50.00% |
50.00% |
| % Overall Assessment |
47.40% |
48.60% |
| Low |
No. |
11 |
6 |
| % Monthly Income |
64.70% |
35.30% |
| % Overall Assessment |
14.50% |
8.10% |
CS: Cross Sectional Study, P: P-value, NS: Non-significant, HS: Highly Significant
Discussion
Tuberculosis (TB) remains a major cause of morbidity and mortality and Viet Nam ranks 12 among the 22 high-TB burden countries [15]. In this study we found 71.3% of samples in the age groups 20-24 years with compared with results in Viet Nam 44.9% [15], in Bangladesh 61.7% [16], this refers to the deterioration of the health situation due to the wars, resulting lack of attention to the health aspect and the lack of medicines. Significant differences in TB organ manifestation in association with season, sex and age suggest different pathophysiological mechanisms of disease development [17]. In our study 52.7% of samples were female, other results found in Malaysia 27.7% [18], in Taiwan 54.4% [19] in India 66.8% [20], this indicate that the difference in lifestyle between countries and most countries suffer from poverty. In our study, 80.7% of samples were single compared with results found in Mexico 92.4% [21]; this refers to the different customs and traditions between the two countries. TB patients and their households are characterized by increasingly lower employment income, lower employment rate and higher dependency on public transfer, but the socio/economic deterioration is rather a risk factor for TB [22]. In this study 48% were moderate monthly income, other results found in Denmark 53% [23], in Sudan 14.9% [24], this is due to the difference in the standard of living between countries and most of limited income families as well as unemployment and lack of opportunities for work (Figure 1).
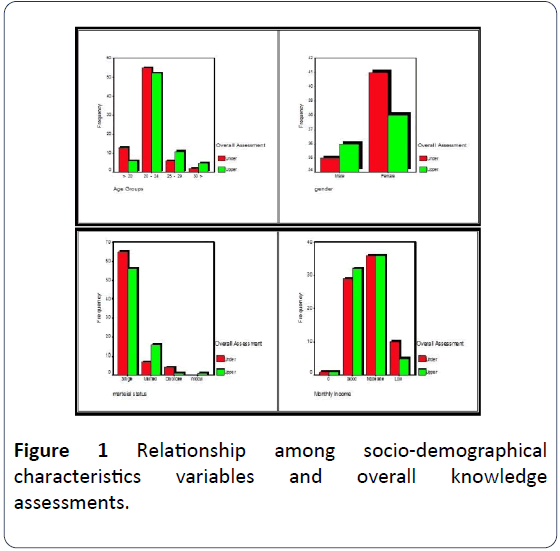
Figure 1: Relationship among socio-demographical characteristics variables and overall knowledge assessments.
Conclusion
We conclude that the half the number of participants are in the age groups 20-24 years; and mostly were females; single; had a moderate monthly income. Highly significant relationship have been found between the department and overall knowledge assessments at the p=0.004. No significant relationship have been found between the age groups, gender, marital status and monthly income with the overall knowledge assessments at the p-value=0.145, p=0.750, p=0.073, p=0.777.
Recommendation
We need to build the communication strategies like training, timely dissemination of information of policy changes and one-to-one dialogue with private practitioners to dispel misconceptions may enhance TB notification. Trust building strategies like providing feedback about referred cases from private sector, health personnel visit or a liaison private doctor may ensure compliance to public health activities. In addition, educational programs should be carried out to create awareness among the at-risk groups.
24081
References
- Golden MP, Vikram HR (2005) Extrapulmonary tuberculosis: an overview. Am Fam Physician 72: 1761-1768.
- World Health Organization (2009) Epidemiology (PDF). Global Tuberculosis Control: Epidemiology, Strategy, Financing 6-33.
- GBD (2013) Mortality and Causes of Death, Collaborators (17 December 2014). Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 385: 117-171.
- Bonah C (2005) The experimental stable of the BCG vaccine: safety, efficacy, proof and standards, 1921–1933. Stud Hist Philos Biol Biomed Sci 36: 696-721.
- Jacob JT, Mehta AK, Leonard MK (2009) Acute forms of tuberculosis in adults. Am J Med 122: 12-7.
- Comstock G (1994) The International tuberculosis campaign: a pioneering venture in mass vaccination and research. Clin Infect Dis 19: 528-540.
- Behera D (2010) Textbook of pulmonary medicine (2nd Edn.). New Delhi: Jaypee Brothers Medical Pub 457-460.
- Bloom ASM, Barry R (1994) Tuberculosis: pathogenesis, protection and control. Washington, D.C: ASM Press.
- Persson, Sheryl (2010) Smallpox, syphilis and salvation: medical breakthroughs that changed the world 141-145.
- Rothschild BM, Martin LD, Lev G, Bercovier H, Bar-Gal GK, et al. (2001) Mycobacterium tuberculosis complex DNA from an extinct bison dated 17,000 years before the present. Clin Infect Dis 33: 305-311.
- Kumar V, Abbas AK, Fausto N, Mitchell RN (2007) Robbins basic pathology (8th Edn.). Saunders Elsevier 516-522.
- Halezeroglu S, Okur E (2014) Thoracic surgery for haemoptysis in the context of tuberculosis: what is the best management approach? J Thoracic Dis 6: 182-185.
- Bhargava A, Pinto L, Pai M (2011) Mismanagement of tuberculosis in India: Causes, consequences, and the way forward. Hypothesis 9: e7.
- Amdekar Y (2009) Changes in the management of tuberculosis. Ind J Pediatrics 76: 739-742.
- Nhung NV, Hoa NB, Khanh PH, Hennig C (2015) Tuberculosis case notification data in Viet Nam, 2007 to 2012. Western Pac Surveill Response J 6: 7-14.
- Mondal MN, Nazrul HM, Chowdhury MR, Howard J (2014) Socio-demographic factors affecting knowledge level of Tuberculosis patients in Rajshahi City, Bangladesh. Health Sci 14: 855-65.
- Padberg I, Bätzing-Feigenbaum J, Sagebiel D (2015) Association of extra-pulmonary tuberculosis with age, sex and season differs depending on the affected organ. Int J Tuberc Lung Dis 19: 723-728.
- Shanmuganathan R, Subramaniam ID (2015) Clinical manifestation and risk factors of tuberculosis infection in Malaysia: case study of a community clinic. Glob J Health Sci 7: 42361.
- Hung CL, Chien JY, Ou CY (2015) Associated factors for tuberculosis recurrence in Taiwan: a nationwide nested case-control study from 1998 to 2010. PLoS One 10: e0124822.
- Sarpal SS, Goel NK, Kumar D, Janmeja AK (2015) Gender disparities in retreatment patients of tuberculosis: A north Indian study. Nat Sci Biol Med 6: 63-66.
- Young BN, Rendon A, Rosas-Taraco A, Baker J, Healy M, et al. (2014) The effects of socioeconomic status, clinical factors, and genetic ancestry on pulmonary tuberculosis disease in northeastern Mexico. PLoS One 9: e94303.
- Suleiman MM, Sahal N, Sodemann M, Elsony A, Aro AR (2014 ) Tuberculosis awareness in Gezira, Sudan: knowledge, attitude and practice case-control survey. East Mediterr Health J 20: 120-129.
- Floe A, Hilberg O, Wejse C, Lokke A, Ibsen R, et al. (2015) The economic burden of tuberculosis in Denmark 1998-2010. Cost analysis in patients and their spouses. Int J Infect Dis 32: 183-190.
- Eldin SGS, Fadl-Elmula I, Ali MS, Ali AB, Salih AL, et al. (2011) Tuberculosis in Sudan: a study of Mycobacterium tuberculosis strain genotype and susceptibility to anti-tuberculosis drugs. BMC Infect Dis 11: 219-230.

