Sarah El-Abbassi*, Asmae Touil, Tayeb Kebdani and Noureddine Benjaafar
Department of Radiation Oncology, National Institute of Oncology, Mohammed V University in Rabat, Morocco
*Corresponding Author:
Sarah El-Abbassi
Resident of Radiation Oncology, Department of Radiation oncology
National Institute of Oncology, Mohamed V University in Rabat, Morocco
Tel: +212661678389
E-mail: drsarahelabbassi@gmail.com
Received Date: March 14, 2017; Accepted Date: May 15, 2017; Published Date: May 18, 2017
Citation: El-Abbassi S, Touil A, Kebdani T, et al. Localized Kaposi Sarcoma. Arch Can Res. 2017, 5:2. DOI: 10.21767/2254-6081.1000140
Kaposi sarcoma (KS) is a lymphoangio-proliferative disease often caused by KS associated herpes virus, also known as human herpes virus 8. There are 4 known variants of KS: Epidemic or AIDS-associated KS, Endemic or African KS, iatrogenic post transplantation KS and Mediterranean or classic KS (CKS). We report a case of CKS treated successfully by radiation therapy.
Case Blog
Kaposi sarcoma (KS) is a lymphoangio-proliferative disease often caused by KS associated herpes virus, also known as human herpes virus 8. There are 4 known variants of KS: Epidemic or AIDS-associated KS, Endemic or African KS, iatrogenic post transplantation KS and Mediterranean or classic KS (CKS). We report a case of CKS treated successfully by radiation therapy.
A-78-year-old Moroccan man presented in our department with 11 months history of chronic lymphedema and painless lesions of lower right extremity. It began as discrete purples patches in the right foot. Patches become elevated, involving into nodules and plaques. His previous medical history revealed hypertension since 15 years for that he was taking antihypertensive drugs, diabetes type 2, and ischemic cerebrovascular accident treated since 1 year. He was not homosexual. On physical assessment, the lesions appear as violaceous patches, plaques and nodules with different sizes in lower right extremity. The nodules tend to enlarge into dome shaped tumors (Figure 1). It was localized only in lower right extremity. No other lesions were found in the body. It should be noted that the patient reports a lymphedema of the lower limbs more severe on the right for 11 months. Walking was limited after the onset of cerebrovascular accident. Skin biopsies were performed. The histo-pathological examination showed formation of intersecting fascicles and sheets of proliferating spindled cells with blood filled vascular spaces. An inceased inflammatory infiltrate consisting of lymphocytes, plasma cells, macrophages and dendritic cells was noted (Figure 2). Immunohistochemistry samples showed prBcl2 antibodies negativity; HHV8 antibodies positivity with overexpression of CD31 and CD34 antibodies (Figure 3). Which characterizes the classical form of nodular KS. A nuclear staining of proliferation index Ki67 of 6% of tumor cells was noted. The HIV, hepatitis B and C serologies were negatives. The case was discussed in multidisciplinary oncological team and radiotherapy was planned. External beam radiotherapy by photons with water bolus at a radiation dose of 8 Grays in one fraction was given. After one and six months of treatment, the clinical revaluation showed a good response (Figures 4 and 5).
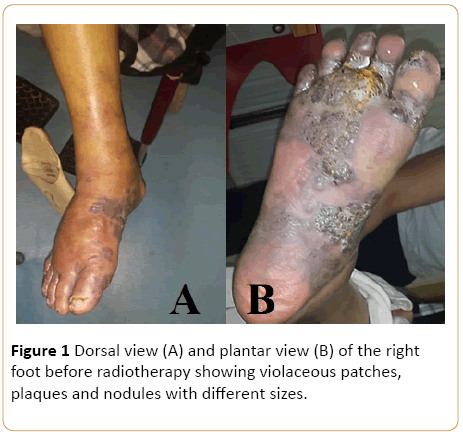
Figure 1: Dorsal view (A) and plantar view (B) of the right foot before radiotherapy showing violaceous patches, plaques and nodules with different sizes.
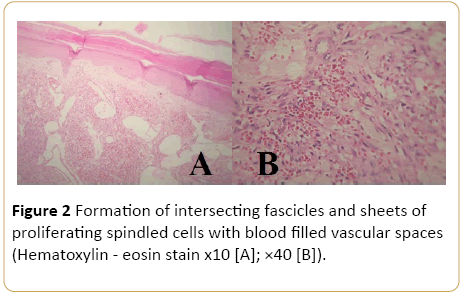
Figure 2: Formation of intersecting fascicles and sheets of proliferating spindled cells with blood filled vascular spaces (Hematoxylin - eosin stain x10 [A]; ×40 [B]).
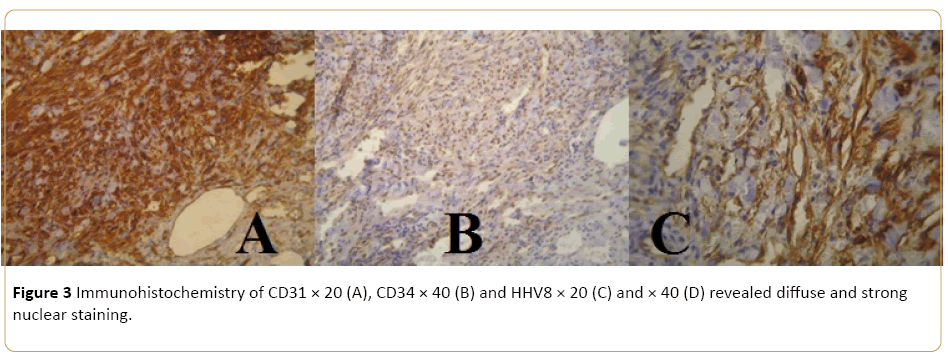
Figure 3: Immunohistochemistry of CD31 × 20 (A), CD34 × 40 (B) and HHV8 × 20 (C) and × 40 (D) revealed diffuse and strong nuclear staining.

Figure 4: Plantar view (A) and dorsal view (B) of the right foot 1 month after radiotherapy showing clinical improvement of lesions.

Figure 5: Dorsal view (A) and plantar view (B) of the right foot 6 month after treatment showing a good response to radiotherapy.
19445

