Keywords
Diagnosis; Lunotriquetral coalition; Plain radiography
Introduction
Lunotriqetral coalition refers to fusion of the lunate and triquetral bones of the carpus. It is the most frequent and often bilateral type of congenital carpal coalition [1,2]. Carpal coalition is largely asymptomatic and often found incidentally on radiographs taken during work-up for trauma or unrelated hand and wrist pain [3,4]. Carpal coalition is also known by other appellations as carpal fusion or carpal synostosis.
Lunotriquetral coalition constitutes 90% of all cases of carpal coalitions followed by coalition between the capitate and hamate (capitohamate coalition), pisiform-triquetral and then trapezium-trapezoid coalitions [2,3,5-11]. Carpal coalition is an unusual anomaly reported to occur in about 0.1% to 9% of the population with a higher incidence in females (F:M=2:1) and people of African descent [12].
Congenital coalitions are deemed to be a failure of differentiation. It may be transmitted as an autosomal (Mendelian) dominant pattern of inheritance which is not sexlinked [4,6,7,13]. The carpus of the wrist arises from undifferentiated mesenchyme between the fourth and eighth weeks of fetal life [5]. All carpal bones originate normally from a single cartilaginous anlage. Synovial joint spaces appear between individual carpal bones following an orderly period of cellular apoptosis [1]. Lunotriquetral coalition results from malsegmentation of the common cartilaginous carpal precursor of the lunate and triquetral bone [4]. This coalition may be fibrous (syndesmosis), cartilaginous (synchondrosis), predominately a mixture of both or osseous. At about the age of 6-15 years, ossification process usually occurs and this become visible on plain radiograph [1,14,15].
Carpal coalition is a bony, fibrous, or cartilaginous connection between adjacent carpal bones [13]. Carpal fusion may occur in two or more adjacent bones in almost any combination (lunotriquetral, capitate-hamate, trapezium-trapezoid, scaphotrapezium, scapho-lunate, capitate-lunate, pisiform-hamate, hamate-triquetrum, triquetral-pisiform and trapezoid-capitate) [1]. The carpal bones on the ulnar side are more commonly affected [18]. The bone fusion may involve two or more carpals or even all carpals may appear as a single bony mass. However, most coalitions occur between carpals within the same carpal row [18]. Coalitions between carpals from different rows are uncommon [19].
Lunotriquetral coalition is classified based on the degree of synostosis between the lunate and triquetrum. In an earlier attempt to classify lunotriquetral coalition, Burnett [20], classified this condition into two types; osseous and nonosseous. In 1952, De Villiers Minnaar [21], suggested a classification system known as the Minnaar types on plain radiograph. The Minnaar type classification is more frequently used and is it comprises of four types namely:
• Type 1: Incomplete (or fibrocartilaginous) fusion - resembles a pseudoarthrosis (2%)
• Type 2. Incomplete osseous fusion (22%)
• Type 3. Complete osseous fusion (75%)
• Type 4. Complete osseous fusion with other carpal abnormalities (1%) [3,22].
Carpal coalition may be congenital or an acquired anomaly seen in healthy individuals. Isolated coalitions normally involve the same carpal row, while syndromic coalitions are complex and often involves bones in different rows with more than two carpal bones involved [10,23,24]. Complex coalitions are linked to other congenital anomalies and hereditary syndromes [9,11,25], such as arthrogryposis, synphalangea, diastrophic dwarfism, Turner’s syndrome, Ellis-van Creveld syndrome, handfoot- uterus, Holt-Oram, otopalatodigital, and dyschondrosteosis [19]. An association with foetal alcohol syndrome is also documented [26]. Acquired intercarpal coalition may be a consequence of multiple inflammatory arthropathies including rheumatoid arthritis, juvenile arthritis, psoriatic arthritis, and Reiter's syndrome among others. It may also result from wrist infection or intentional surgical arthrodesis.
Plain radiography is the primary imaging modality of choice in patients with trauma or pains in the hand, especially when osseous pathology is being considered [27]. Computed Tomography (CT) and Magnetic resonance imaging (MRI) may also be of use especially when there is need to classify fibrocartilagenous type of this anomal [28]. There is dearth of information on this entity in the literature in our setting, hence the need to reappraise this seemingly normal anatomic variant with a potential of causing wrist pain of unclear origin.
Case Report
Case A
The patient is a 38-year old female who presented for X-ray of the right hand. She had complained of pain in the hand following a brawl in a shared rented apartment. Consequently, plain radiograph of her right hand was obtained. The radiograph revealed fusion of the lunate and triquetral bones of the carpus with widening of scapholunate joint space (lunotriquetral synostosis). No fracture was seen in Figure 1.
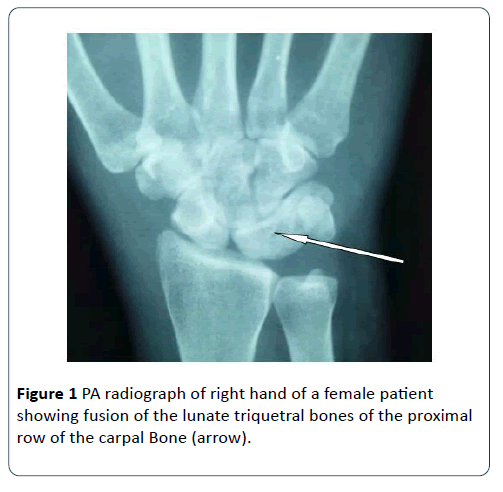
Figure 1: PA radiograph of right hand of a female patient showing fusion of the lunate triquetral bones of the proximal row of the carpal Bone (arrow).
Case B
A 42-year-old man presented for radiograph of both hands following pains in the hands. Patient attributed pain to suspected fracture which he presumed he sustained during a squabble with the law enforcement agents. On physical examination, there was no limitation in range of motion of the wrist. There was no swelling or tenderness in the wrist. Other findings were normal. Plain posteroanterior radiographs of both wrists showed bilateral lunotriquetral coalition (Figures 2 and 3).
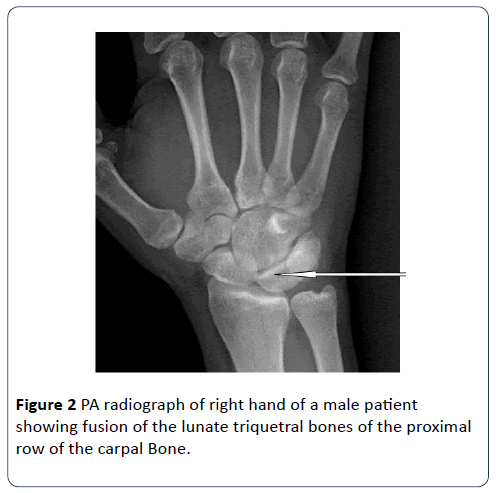
Figure 2: PA radiograph of right hand of a male patient showing fusion of the lunate triquetral bones of the proximal row of the carpal Bone.
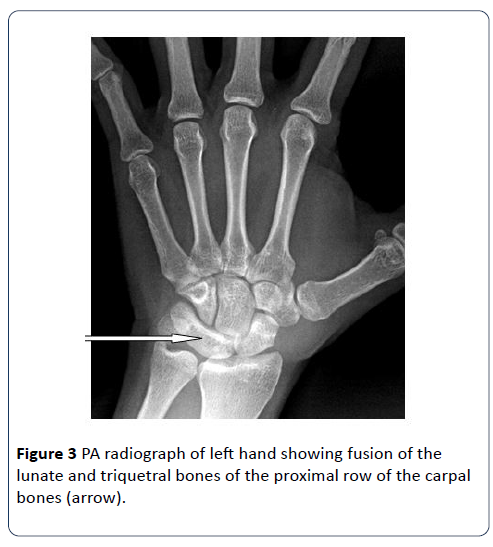
Figure 3: PA radiograph of left hand showing fusion of the lunate and triquetral bones of the proximal row of the carpal bones (arrow).
Discussion
Carpal coalitions are known anatomical variants, which have been documented in their different forms of occurrence. The most commonly documented pattern in the literature is the lunate-triquetral synostosis [3,4,29]. In the study of ancient diseases, lunotriquetral coalition was found in a Neanderthal individual dated at 74.000 to 68.000 years before the present (BP) [30,31]. Carpal coalition was first described by Sandifort in 1779 and the first clinical case report of carpal coalition was by Corson in 1908 [10,32]. Fusion of carpal bones may be congenital or an acquired anomaly. Mostly, it is a chance finding usually found on radiographs obtained for other reasons [1]. Most cases of this condition are often asymptomatic, but may become symptomatic following trauma. The two cases under review were being investigated for suspicious fracture. However, there was no fracture but lunotriquetral coalition was found incidentally. Although, we could not ascertain the relationship between hand pain and the coalition.
In the two cases under review, patients developed pain in the hand as a result of trauma sustained following a brawl. This is in keeping with the literatures documented by [4,23,33]. According to Singh et al. [4], coalitions may predispose or lead to symptomatic pathology following trauma or excessive load to the affected wrist. They attributed the origin of the pain to biomechanical alterations that result from structural fusion at the wrist. In Knenzvich et al. [23] study, they stated that loss of movement between the fused bones and a compensatory increase in motion at surrounding joints theoretically predisposes individuals to recurrent sprains and pain under conditions of excessive physical stress. Gross et al. [32], equally reported that this condition may be particularly true for nonosseous coalitions, in which deficient intra-articular cartilage formation may lead to a clinical and anatomical state resemble degenerative arthritis.
The two patients being reviewed are Nigerian and are of West African descent. The rate of occurrence of intercarpal fusion has been documented to have a wide geographic variation [3,15,18,19,34]. Similarly, among the various populations reported, the highest rate of occurrence of this anomaly was seen in individuals of West African descent, with reports as high as 9.5 % in some groups [3,12,15,35]. These are in agreement with our report.
None of our patients reported a history of arthritis, trauma or previous surgical procedure such as arthrodesis. Furthermore, none of the radiographs in this study demonstrated evidence of carpal malalignment, arthrosis or intercarpal diastasis. Thus, our cases likely reflect congenital malformations in carpal development. Lunotriquetral coalition was bilateral in one of them who had bilateral wrist radiographs. These findings are similar to those observed in the literature, with increased incidence in black people and the presence of bilaterality [3,15,36].
Carpal coalitions are most commonly incidental findings. Unlike tarsal coalitions they are usually asymptomatic. When symptomatic, they are one of the differential diagnoses to be included in wrist pain. Clinical information should always exclude an acquired fusion secondary to arthritis, trauma, surgery, drug intake during pregnancy or a metaplastic conversion of intraarticular structures (fibrous tissue, ligaments or cartilage) [35].
Most cases can be treated conservatively but persistent symptoms may require operative intervention. Limited resection of the distal scaphoid with excision of the coalition may be another treatment option when symptoms fail to settle with non-operative treatment.
Conclusion
Lunotriquetral coalition is the most common type of carpal coalition and generally asymptomatic. However, coalitions may predispose or lead to symptomatic pathology following trauma or excessive load to the affected wrist. Highest prevalence of carpal coalition has been observed in blacks especially of West African descent. Radiography is an important tool to diagnose this anomaly. Lunotriquetral coalition should be considered in the differential diagnosis in patients with wrist pain. Careful assessment of the carpal bones during evaluation of the radiograph of the hand following work-up of wrist pain is very rewarding.
24568
References
- Vanhoenacker F, Verstraete K (2015) Lunotriquetral coalition, a normal variant that may rarely cause ulnar sided wrist pain. JBR-BTR 98: 72-78.
- Lotter O, Stahl S, Luz O, Pfau M, Schaller HE (2010) Bilateral paradoxically symptomatic lunotriquetral coalition: a case report. Open Access J Plastic Surg 10: e47.
- DeFazio MV, Cousins BJ, Miversuski Jr RA, Cardoso R (2013) Carpal coalition: a review of current knowledge and report of a single institution's experience with asymptomatic intercarpal fusion. Hand 8: 157-163.
- Singh P, Tuli A, Choudhry R, Mangal A (2003) Inter-carpal Fusion-A Review. J Anat Soc India 52: 183-188.
- Xipoleas GD, Villanueva NL, Ting J (2014) Trans-scaphoid trans-lunotriquetral perilunate dislocation in a patient with a carpal coalition. Plast Reconstr Surg Glob Open 2: e144.
- Van Schoonhoven J, Prommersberger KJ, Schmitt R (2001) Traumatic disruption of a fibrocartilage lunate-triquetral coalition: a case report and review of the literature. Hand Surg 6: 103-108.
- Carlson DH (1981) Coalition of the carpal bones. Skeletal Radiol 7: 125-127.
- Ingram C, Hall RF, Gonzalez M (1997) Congenital Fusion of the Scaphoid, Trapezium, Trapezoid and Capitate. J Hand Surg (European Volume) 22: 167-168.
- Weinzweig J, Watson HK, Herbert TJ, Shaer JA (1997) Congenital Synchondrosis of the Scaphotrapezio-Trapezoidal Joint. J Hand Surg (Am) 22: 74-77.
- O’Rahilly R (1953) A Survey of Carpal and Tarsal Anomalies. J Bone Joint Surg 35: 626-642.
- Simmons BP, McKenzie WD (1985) Symptomatic carpal coalition. J Hand Surg 10: 190-193.
- Timins ME (1999) Osseous anatomic variants of the wrist: findings on MR imaging. Am J Roentgenolol 173: 339-344.
- Ritt MJ, Maas M, Bos KE (2001) Minnaar type 1 symptomatic lunotriquetral coalition: a report of nine patients. J Hand Surg Am 26: 261-270.
- Cockshott WP (1963) Carpal fusions. Am J Roentgenol Radium Ther Nucl Med 89: 1260-1271.
- Pfirrmann CW, Zanetti M (2005) Variants, pitfalls and asymptomatic findings in wrist and hand imaging. Eur J Radiol 2013: 286-295.
- Garn SM, Frisancho R, Poznanski AK, Schweitzer J, McCann MB (1971) Analysis of Triquetral-Lunate fusion. Am J Physical Anthropolog 34: 431-434.
- Poznanski AK, Holt JF (1971) The carpals in congenital malformation syndromes. Am J Roentgenol Radium Ther Nucl Med 112: 443-459.
- Burnett S (2011) Hamate-pisiform coalition: morphology, clinical significance and a simplified classification scheme for carpal coalition. Clin Anat 24: 188-196.
- De Villiers Minnaar AB (1952) Congenital fusion of the lunate and triquetral bones in the South African Bantu. J Bone Joint Surg Br 34: 45-48.
- Kahane S, Isaac SM, Wildin C (2012) A new type of carpal coalition. J Hand Surg Eur 37: 581-582.
- Knezevich S, Gottesman M (1990) Symptomatic Scapholunatotriquetral Carpal Coalition with Fusion of the Capitometacarpal Joint. Clin Orthop Relat Res 251: 153-154.
- Smith-Hoefer E, Szabo RM (1985) Isolated Carpal Synchondrosis of the Scaphoid and Trapezium. J Bone Joint Surg 67: 318-320.
- Jaffer Z, Nelson M, Beighton P (1981) Bone fusion in foetal alcohol syndrome. J Bone Joint Surg 63B: 569-571.
- Weathers WM, Spence SC, Beckman NM (2015) Osseous Scaphotrapezial Coalition. Case Rep Radiol 2015: 1-3.
- Porteous R, Harish S, Parasu N (2012) Imaging of ulnar-sided wrist pain. Can Assoc Radiol J 62: 18-29.
- Pruszczynski B, Saller J, Rogers KJ, Holmes L Jr, Ty JM (2016) Incidence of carpal coalition in the pediatric population. J Pediatr Orthop 36: e106-e110.
- Saccheri P, Sabbadini G, Crivellato E, Canci A, Toso F, et al. (2017) Capitate-trapezoid synostosis: analysis of an early bronze age case and review of the literature. Folia Morphol (Warsz) 76: 149-156.
- Oberlin C, Sakka M (1989) The most ancient case of synostosis of the carpal bones: pyramido-lunate synostosis in La Ferrassie man. Ann Chir Main 8: 269-272.
- Athar MS, Aerialis G, Ashwood N, Bain G (2017) Symptomatic scaphotrapeziotrapezoid carpal coalition: the natural history and a surgical option for treatment. Open J Orthop 7: 127-139.
- Gross SC, Watson HK, Strickland JW, Palmer AK, Brenner LH, et al. (1989) Triquetral–lunate arthritis secondary to synostosis. J Hand Surg Am 14: 95-102.
- Orlin H, Alpert M (1967) Carpal coalition in arthrogryposis multiplex congenita. Br J Radiol 40: 220-222.
- Satbler A, Glaser C, Reiser M, Resnick D (1999) Symptomatic fibrous lunato–triquetral coalition. Eur Radiol 9: 1643-1646.
- Szaboky GT, Muller J, Melnick J, Tamburro R (1969) Anomalous fusion between the lunate and triquetrum. J Bone Joint Surg 51: 1001-1004.

