Ana-Maria Dumitrescu1, Roxana Gabriela Cobzaru2*, Carmen Rîpă2, Ana-Maria Slănină3, Roxana Florentina Șufaru1, Maria Cristina Gavrilescu4, Elena Rezuș5, Liviu-Ciprian Gavril1 and Anca Sava1
1Department of Anatomy and Embriology, Grigore T. Popa University of Medicine and Pharmacy, Iasi, Romania
2Department of Microbiology and Parasitology, Grigore T. Popa University of Medicine and Pharmacy, Iasi, Romania
3Department of Family Medicine, Grigore T. Popa University of Medicine and Pharmacy, Iasi, Romania
4Department of Internal Medicine,Grigore T. Popa University of Medicine and Pharmacy, Iasi, Romania
5Department of Rheumatology, Grigore T. Popa University of Medicine and Pharmacy, Iasi, Romania
- *Corresponding Author:
- Roxana-Gabriela Cobzaru
Lecturer, Department of Microbiology Grigore T. Popa University of Medicine and Pharmacy, Iasi, Romania
Tel: 0040740533005
E-mail: roxanabahnea@yahoo.com
Received Date: March 02, 2021; Accepted Date: March 15, 2021; Published Date: March 18, 2021
Citation: Dumitrescu AM, Cobzaru RG, Rîpă C, Slănină AM, Șufaru RF, et al. (2021) Paradoxical Stroke Related to Asymmetrical Circle of Willis - Case Presentation and Literature Review. Health Sci J. 15 No. 3: 813.
Keywords
f- PCA; Stroke; Circle of willis; Anatomical variants
Introduction
The fetal posterior cerebral artery (f-PCA) is an anatomical variant of the circle of Willis that is correlated with a blood supply of the territory of the posterior cerebral artery (PCA) from the anterior circulation. In the presence of f-PCA, thromboembolism in the anterior circulation can lead to paradoxical infarction in the controlateral posterior cerebral artery (PCA) territory with or without concomitant infarction in the territories of the middle cerebral artery (MCA) or anterior cerebral artery (ACA) [1].
f-PCA clearly contributes to the mechanism of paradoxical infarction and revealed the clinical significance of this anatomical variant of the circle of Willis. The posterior cerebral artery is involved in 5-10% of strokes. Its role is to ensure the irrigation of the posterior part of the brain, namely: the occipital lobe, the lower part of the temporal lobe, the hippocampus, the lower part of the parietal lob, the brainstem, the basal nuclei and the thalamus [2].
Material and Method
We present the case of a male 82-year old patient, with several submissions in the emergency care unit of the “Prof. Dr.N.Oblu” Emergency Clinical Hospital, Iasi, which is a main health care centre of the Nord-Eastern region of Romania. The patient presented several comorbidities such as diabetes mellitus, hypertension stage 2, renal hydronephrosis, atrial fibrillation, and ischemic cardiopathy. His first submission to the emergency unit in 2014 had been due to an episode of transient ischemic attack, but after one year of not respecting his treatment and not willing to engage enough in occupational therapy procedures, he developed a second stroke, this time a large one, with secondary reperfusion, which lead to patient's death in a short time from his admission in our hospital. The patient died due to a brain infarction with reperfusion in the territory of the right PCA. At autopsy, an asymmetrical circle of Willis due to the presence of a left fetal PCA and right hypoplastic posterior communicating artery (PComA). Data from literature regardingthis particular type of paradoxal stroke and the coexistence of the two anatomical variants in the circle of Willis has been researched with the selection of 13 significant articles published in the period of the last 20 years.
Results and Discussions
Case presentation
A 82 year-old male patient, smoker, with a history of type 2 diabetes mellitus, uncontrolled hypertension and atrial fibrillation was brought to the emergency department (ED) by his son for evaluation of an 1-hour history of nausea, new onset headache, dizziness, paresthesia, limb weakness and confusion. The patient denied a history of falls, head trauma, seizures. His vital signs were temperature (T): 37.3°C, blood pressure (BP): 190/100 mm Hg, heart rate (HR): 99/min. He kept being alert and oriented in space and time. He had an acute onset of dysarthria, left upper extremity weakness, and a recent episode of monocular vision loss that resolved on its own. The brain magnetic resonance imaging (MRI) revealed small acute infarcts in the right PCA area. The cerebral computed tomography (CT) did not show any haemorrhage. He was diagnosed with transient ischemic attack (TIA) located in the territory of the right posterior cerebral artery (PCA). The patient was prescribed antithrombotic drugs, vasodilator drugs, antihypertensive and oral anti-diabetic medication. Afterwards, the patient went to see his family practitioner in order to complete and continue his therapy at home. But after one year of non-compliance to treatment and the refusal of occupational therapy home based interventions, the patient was submitted again in the emergency unit department with left hemiplegia and deep vein thrombosis. He underwent a cerebral CT which revealed hypodensity in the right temporal-occipital lobes with diffuse densities of blood. On the pulmonary X-ray, there was noticed the presence of a cardiomegaly and the electrocardiography (EKG) revealed an aspect of atrial fibrillation and trigeminy. Within one day from the second admission, the patient entered in a coma and died after a few hours. An autopsy was performed and revealed the following macroscopical aspects:
• Two anatomical variants of of the constituent arteries of the circle of Willis, i.e. hypoplasia of the right posterior communicating artery (PComA) and right fetal posterior cerebral artery (f-PCA).
• Presence of atherosclerotic plaques in all the vessels of the circle of Willis
• After sectioning the brain, a massive infarcted area with blood reperfusion in the right temporal-occipital lobes was observed.
• The autopsy also revealed: acute myocardial infarction, Left kidney hydronephrosis, and pancreatic lipomatosis.
Occupational therapy and rehabilitation recommendations in the case of patients with transient ischemic stroke
Even though patients with TIA and stroke manifest similar symptoms, TIA symptoms usually resolve within the first few hours of onset, whereas stroke symptoms persist much longer [3].
According to the American Occupational Therapy Association (AOTA) In the United States, stroke represents an important cause of adult disability, having approximately 7 million individuals that have survived a type of stroke.
In our case, the patient responded little to therapeutical procedures, by being a un-cooperative individual. There is taken into discussion whether the involvement of systematic occupational therapy for transient ischemic attack (TIA) would have ameliorated and prolonged the patient’s lifespan. In case of post-stroke survivors, the AOTA recommends collaboration between occupational therapists, clients and their families and other healthcare professionals (nurses, carers etc.). It is also indicated that the occupational therapist relates the interventions to the client’s functional environment, the place where they would have to continue to work or to live in after the stroke occurred [4].
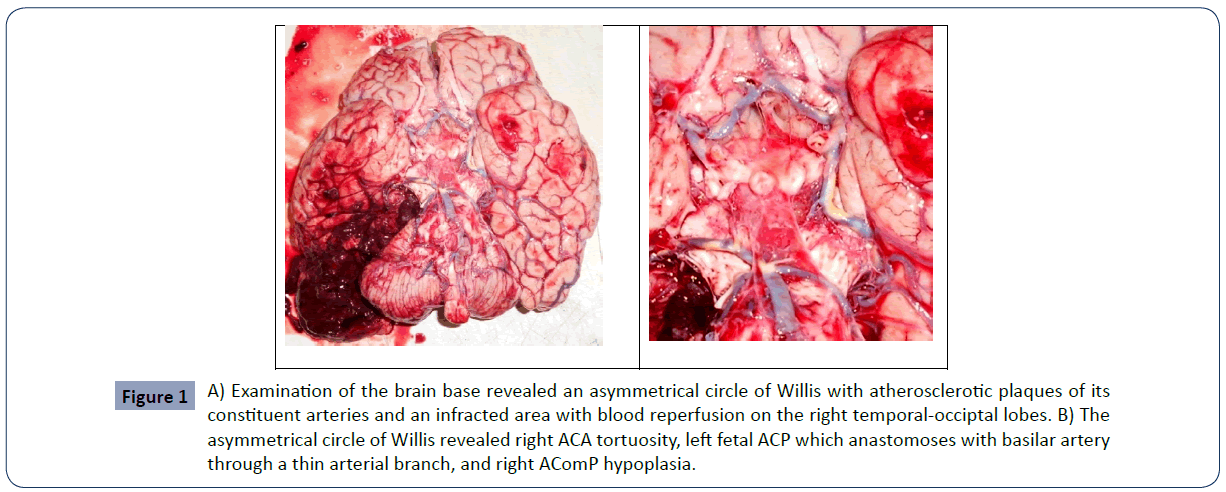
Figure 1 A) Examination of the brain base revealed an asymmetrical circle of Willis with atherosclerotic plaques of its constituent arteries and an infracted area with blood reperfusion on the right temporal-occiptal lobes. B) The asymmetrical circle of Willis revealed right ACA tortuosity, left fetal ACP which anastomoses with basilar artery through a thin arterial branch, and right AComP hypoplasia.
As procedures to be indicated in these cases, there is a highlight on daily living adjustments regarding cooking a meal, going to the grocery, money management and eventually parenting (the IADLs), through the improvement of patients’ global sense of weakness, sensory loss and other cognitive or visual issues. There is a focus on therapeutical procedures such as: upper limb positioning, mobilization techniques-through positioning, turning, and transferring, prevention of pressure injuries through cushions and padding, barrier sprays. The occupational therapist’s role is to educate patients on energy conservation techniques, ability of self-care, global functional improvement or therapeutic exercise in post stroke patients [4-6].
Patients with posterior cerebral artery stroke usually experience severe visual alteration and will require changing in their activities of daily living (ADLs). Therefore, they become more exposed to falls and they are not allowed to drive until they get a complete follow-up and a visual-field examination by an ophthalmologist. These patients, being in post stroke states, should also maintain a close contact with their family physician, for obtaining further guidance and better management. In the case of hemiparesis which may occur quite often in the case of these patients, they should obtain the help of their occupational therapists through transfer techniques, mechanically assisted walking and changing of their ADLs. Depending on the severity of their states, it would be beneficial for them to be under the care of an occupational therapist in a home-based setting [7].
The occupational therapist could be very beneficial in the case of post stroke rehabilitation, because of the great help it could offer to these patients. Work-related tasks, as well as the re-involvement in leisure activities are some of the key factors contributing to the patient’s wellbeing [5].
Literature review on paradoxical stroke related to the asymmetrical circle of willis
The case we presented here developed a temporal-occipital infarction with reperfusion due to a thromboembolism of the right posterior cerebral artery. We also identified the presence of an ipsilateral hypoplastic PComA and a left fetal posterior cerebral artery (f-PCA). Taken together, all these anatomical variants have a role in the development of the cerebral infarct with reperfussion. Van Raamt et alclaims that the patients with f-PCA have an increased risk of ischemic lesions of the anterior and posterior brain areas due to the absence of proper collateral arteries [8]. In our case the infarction affected the controlateral hemisphere, event which is named in literature as paradoxical stroke, probably due to the presence of the hypoplastic right PComA.
The thromboembolism was favoured by the presence of atherosclerosis in the intima of the constituent arteries of the circle of Willis, which reduced the lumen of the vessels, including the right PCA. Also, the presence of associated atherosclerotic plaques caused the occurence of thrombosis that completely obstructed the right lumen of the PCA and caused the right temporal-occipital infarction. The mechanism of the development of the cerebral infarction could have been as follows: due to the obvious hypoplasia of the right posterior communicating artery (PComA), the PCA territory lacked the blood supply that could have been brought by the right internal carotid artery (ICA), so as to ensure the normal blood supply in right PCA obstruction. Due to the fact that the cerebral infarction was massive, there was an increased risk of reperfusion in the mentioned territory because of the antithrombotic treatment. There are authors who state that the greater the extent of the infarction area is, the higher the incidence of hemorrhagic transformation becomes [9].
Moreover, massive cerebral infarction is often accompanied by substantial cerebral edema, which leads to compression of the peripheral vasculature. Increased permeability of the vascular wall due to prolonged ischemia and hypoxia caused by vascular compression greatly increases the chances of hemorrhagic transformation of a cerebral infarction after removal of edema by medication.
There are authors which consider that the presence of an ACP-f does not cause a stroke on the same side [10].
Others emphasize the fact that f-PCA can increase the extent and severity of a stroke on the opposite side [1].
In an autopsy study realized on 49 infarcted brains and 88 control brains, more f-PCA were found in patients with cerebral infarction than in control patients (27 vs. 17%) [11].
In another autopsy study, which analysed the circle of Willis from 167 infarcted brains and 90 control brains, the authors found out that more f-PCA were associated with infarcted brains than with normal brains [12].
Recently, a study showed that f-PCA and occipital lobe infarction were linked [13]. In 174 patients with cerebral ischemic stroke, angio-MRI shown that angio MRI showed that ipsilateral strokes were observed in two-thirds of patients and contralateral strokes were identified in one-third of patients [14].
In the present case, we consider that the presence of the left fetal-type posterior cerebral artery ensures good irrigation on the left side, but probably it realizes a kind of "theft" of blood from the internal carotid system, leaving too little blood for the opposite side. This mechanism lead to a controlateral infarction especially due to the fact that the artery that should realize a connection between the anterior circulation with the posterior one failed due to the hypoplastic right PComA.
Conclusion
The paradoxical type of stroke is less discussed in the literature, representing a rare stroke development. It becomes important in the context of anatomical variants of the circle of Willis, as discussed above. With the correct therapy administration and the help of occupational therapy home-based procedures, a transient ischemic attack could be better controlled, and its evolution towards an ischemic or hemorrhagic stroke would be slowed down. In case of recurrent ischemic strokes could be prevented by a multi-disciplinary team made of a medical doctor (either neurologist, family physician and other practitioners), nurses, carers, occupational therapists and physiotherapists and correct drug-administration.
35971
References
- Lambert SL, Williams FJ, Oganisyan ZZ, Branch LA, Mader EC Jr. (2016) Fetal-Type Variants of the Posterior Cerebral Artery and Concurrent Infarction in the Major Arterial Territories of the Cerebral Hemisphere. J Investig Med High Impact Case Rep 4: 2324709616665409.
- Kuybu O, Tadi P, Dossani RH (2021) Posterior Cerebral Artery Stroke. Treasure Island (FL): StatPearls Publishing.
- Coutts SB (2017) Diagnosis and Management of Transient Ischemic Attack. Continuum (MinneapMinn) 23: 82–92.
- (2015) The role of Occupational Therapy in Stroke Rehabilitation. American Journal of Occupational Therapy.
- Rowland TJ, Cooke DM, Gustafsson LA(2008) Role of occupational therapy after stroke. Ann Indian Acad Neurol 11:S99-S107.
- Schmid AA, Butterbaugh L, Egolf C, Richards V, Williams L (2008) Prevention of secondary stroke in VA: Role of occupational therapists and physical therapists. J Rehabil Res Dev 45: 1019-1026.
- Eroğlu M, Karapolat H, Atamaz F, Tanıgör G, Kirazlı Y (2020) Occupational therapy assessment and treatment approach in patients with subacute and chronic stroke: A single-blind, prospective, randomized clinical trial. Turk J Phys Med Rehabil 66: 316–328.
- van Raamt AF, Mali WPTM, van Laar PJ, van der Graaf Y (2006) The fetal variant of the circle of Willis and its influence on the cerebral collateral circulation. Cerebrovasc Dis 22:217-224.
- Zhang J, Yang Y, Sun H, XingY (2014) Hemorrhagic transformation after cerebral infarction: current concepts and challenges. Ann Transl Med 2: 81.
- Shaban A, Albright KC, Boehme AK, Martin-Schild S (2013) Circle of Willis Variants: Fetal PCA. Stroke Research and Treatment2013: 105937.
- Macchi C, Catini C, Federico C, Gulisano M, Pacini P, et al. (1996) Magnetic resonance angiographic evaluation of circulus arteriosus cerebri (circle of Willis): a morphologic study in 100 human healthy subjects. Ital J Anat Embryol 101: 115-123.
- Kameyama M, Okinaka SH (1963) Collateral circulation of the brain with special reference to atherosclerosis of the major cervical and cerebral arteries. Neurol 13: 279-286.
- Jongen JC, Franke CL, Ramos LM, Wilmink JT, van Gijn J (2004) Direction of flow in posterior communicating artery on magnetic resonance angiography in patients with occipital lobe heart attacks. Stroke 35: 104-108.
- Adhithiya V, Nadhamuni K, Hussain MRK, Anand A, Amirthalingam U, et al. (2021) Influence of Foetal Origin of Posterior Cerebral Artery on Ischaemic Stroke. International Journal of Anatomy, Radiology and Surgery 10: RO41-RO43.

