Keywords
Accreditation; Patient satisfaction; Joint commission international
Introduction
Accreditation of health market has been implemented in many countries in the world, and this approach is growing to ensure quality of services provided to the patients [1]; those countries use this program to improve the quality of services [2]. Healthcare organizations consider accreditation a tool that measures the quality improvement of the health care organizations’ provided services, along with other quality indicators, such as morbidity, mortality, hospital infection rates and patient satisfaction [3], which is considered in many countries an integral part of the health system [4]. The Appraisal of Quality program is required by the accreditation body [5]. The key parameter to evaluate the quality of care and the health care services provided in the hospital setting is patient satisfaction [3], thus many health care organizations, and mainly hospitals, have considered measuring patient satisfaction [6].
In some countries, accreditation is still voluntary [4] and in other countries it is mandated by the government [6]. Health care organizations may be accredited by a national or local accreditation body, for example the Health Care Accreditation Council (HCAC) in Jordan, or by an international accreditation body like Joint Commission International (JCI). One of the famous accreditation bodies and largest in the world.
According to the study conducted by Nicklen in 2014, there are many areas of accreditation that require further studies. Of these areas were patient involvement in quality improvement and methods of assuring quality, like performance measures [4]. There is insufficient information about patient satisfaction with JCI [8].
Accreditation
Healthcare organizations are usually accredited for their compliance with pre-standards. The survey focused on the implementation of the standards and processes; the assumption is that if healthcare organizations are regulated and controlled properly as per the standards, patient health outcomes and patient satisfaction are likely to be improved [3]. Accreditation may have a positive impact with the standardization of procedures, cost containment or even marketing, especially in competitors’ market where accreditation is perceived by the public as a quality indicator.
JCI accreditation
Improving the quality of care in hospitals began in the early 20th century; three associations decided to expand accreditation through joining to establish Joint Commission on Accreditation of Hospitals (JCAHO) in 1951. JCAHO accredited health care organizations in the USA [9]. The international branch for JCAHO is the Joint Commission International (JCI), which was established in 1991 to accredit health care organizations around the world. JCI developed measures in quality and safety to provide innovative solutions across all healthcare organizations, improve their performance and health outcomes and finally award them JCI accreditation and certification [34].
Patient satisfaction
The flourishing and rapid progression in the quality program and health system introduces the patient-centred care (PCC) concept to be one of the core concepts in the health system. The patient satisfaction measure has become an acceptable tool for the evaluation of the quality program and health services provided, adding to that the patient’s needs and preferences being a valuable issue in the health system [11]. Satisfaction as a concept is the affective judgment on the health services provided formed by the patient [13] or the comparison between expectations and perceptions depending on this meaning, healthcare managers are trying to achieve excellence of services when designing the quality program and take patient perception into account [14]. The measurement of patient satisfaction is an important and legitimate indicator, and some countries make it mandatory, as France did in 1996 [10] and Germany in 2005 [14]. The measurement is built on that the level of quality of services experienced by patients is determined by the gap between their expectations and perception of what they actually receive [15]. The patient’s opinion, safety and the clinical effectiveness are all pillars of the quality of healthcare. The patient’s safety and clinical effectiveness have a positive impact on his experiences [12]. Patient satisfaction may be dependent on various factors other than the services provided, it may also depend on the demographic patient characteristics or the hospital’s characteristics [16]. The demographic patient characteristics include: age, gender, health status, socio-economic factors, educational level, LOS, occupation etc. [18]. The literature showed that characteristics have a significant correlation with patient satisfaction, while other studies showed no correlation with the level of patient satisfaction [19]. Some literatures studied the LOS’s impact on patient satisfaction to ensure that the LOS influences the patient’s satisfaction [21], while others found no evidence that the hospital LOS, either for a short or a long period, had any correlation with patient satisfaction [22]. The hospital characteristics include teaching status, size, region, profit orientation and staffing per bed [17,24]. These variables may have a significant impact on patient satisfaction or may not have a significant impact on the patient satisfaction [27].
The studies that assessed patient satisfaction and accreditation
Patient satisfaction is an important dimension that reflects patients’ experiences of the quality of services provided [2]. The patient satisfaction findings are used to monitor the quality of health care and accreditation [8]. Some studies assessed the patient satisfaction and accreditation have shown that the impact of hospital accreditation on patient satisfaction is significantly positive [1,8,18], while other studies showed that hospital accreditation has no significant impact on patient satisfaction [3,20].
Methodology
Study design and sampling
There are different types of scientific methods of research that differ in their purpose, approach and process. In this study, quantitative descriptive cross-sectional research and convenient sampling was utilized. Convenient sampling is a non-probability sampling technique where the participants who meet the criteria of the study are used. This sampling method was not used because it was easier for the researcher, but because it can represent the target population and meet the criteria to obtain representative data [29].
Inclusion and Exclusion Criteria: Inclusion criteria in this study include patients who are treated at hospital as inpatient, adult patient (above 18 years old) and patients who stayed in the hospital for more than 1 day and equal to or less than 30 days. Exclusion criteria include patients who are critically ill (CCU and ICU patients), patients who are mentally or psychologically and patients who are not able to read and write.
Study population and sample size: The study population includes a sample of patients who are treated at Al Makassed Al-Arabi Hospital as in patients. There are formal statistics from the hospitals that show that the number of inpatients, and according to the inclusion and exclusion criteria, is 2400 patients, and so the sample size was calculated depending on that number from the two hospitals. The sample size, taking into consideration that the marginal error=5%, confidence level 95%, response rate of around 60%, was calculated based on this equation from Raosoft® Application.
x=Z(c/100)2r (100-r), n=N x/((N-1) E2 + x), E=Sqrt [(N-n) x/n (N-1)]
N is the population size, r is the fraction of responses that you are interested in, and Z(c/100) is the critical value for the confidence level c.
The Recommended Sample Size is 332.
Instrument
The researcher used the SERVQUAL questionnaire developed by Parasuraman et al. [7] which was designed to measure a patient's perception and expectation of services provided by the hospitals. SERVQUAL is constructed of 22 items representing five dimensions. A Likert -type scale, ranking from (1) for ‘Strongly Disagree’ to (5) for ‘Strongly Agree’ was used to measure the service quality scales [7].
The dimension suggested by Parasuraman were:
• Tangibles: Availability of physical facilities, equipment, personnel appearance.
• Reliability: Ability to perform the promised service dependably and precisely.
• Responsiveness: Willingness to assist patients and provide appropriate services.
• Assurance: Employees’ knowledge, kindness and their ability to inspire trust.
• Empathy: caring; individualized attention given to patients.
The questionnaire was translated to Arabic, being it the formal language of Palestine and the language spoken was also Arabic. The Arabic version of this questionnaire is the same as the instrument which was used by the Jordanian researcher. Permission from the researcher was obtained, and the translation was revised by a legal Palestinian translator then compared to the Jordanian version.
Reliability and validity
It is the extent to which the measurement is consistent over time. Homogeneity is the consistency of scoring, calculated by Cronbach Alpha test, by correlating each item with all other items (0-1). What is considered a satisfactory level of reliability is a score higher than 0.70 [23]. All dimensions of the questionnaire have had an acceptable level of scoring measurement, as illustrated in the Table 1.
Table 1 Cronbach alpha results for the reliability test.
| Reliability Statistics |
| Dimensions |
Alpha |
| Tangible |
0.825 |
| Reliability |
0.822 |
| Responsiveness |
0.824 |
| Assurance |
0.825 |
| Empathy |
0.825 |
| Total |
0.824 |
The researcher had contacted four experts to validate the questionnaire used in the study. Two of these experts are specialized in the quality of services and accreditation, and the other two were academic experts and researchers, in addition to the statistician. They reviewed the questionnaire and gave their recommendations to the researcher, and modified by the researcher based on those recommendations.
Data collection
The researcher distributed the questionnaires to the inpatients who planned for discharge into the two hospitals that participated in this study according to these criteria, then collected the data from the patients in the same day, and during that same time, data collection started in October/2016 and continued till the end of November/2016.
Data entry and analysis
The researcher entered all the data using the statistical package for social sciences, and the total questionnaires entered were 332. All data was analyzed using the SPSS software program version 18 for analyzing quantitative data with the assist of a statistician, frequencies, percentages, ranges, means and standard deviation, in addition to T-test and ANOVA which were also used.
Ethical consideration and permission
Ethical approval and an official letter from Al-Quds University was obtained to facilitate the work and allow the researcher get the permissions letters from the hospitals. The two hospitals’ directors gave their approval for conducting the study and formal approval letters were obtained, then data collection started. The cover page of the questionnaire has written information to provide all the participants with a brief introduction about the study, its aim and its objectives.
Results
The demographic characteristics in this study were age, gender, educational level and place of residency. 332 patients filled the questionnaire, most of whom were participants from the accredited hospital (65.7%) while (34.3%) of the sample were from the non-accredited hospital, based on the number of admissions for each hospital. The data showed that the percentage of females from the total sample was 56.3%, while 43.7% were men. The average age of the respondents was 41.6 years, the age category between 26-50 years which represent highest percentage 49.7%. The average length of the stay of respondents was 6.4 days, and the patient who stayed between 2-7 days equal 72.9%.
In general, patients have a high level of satisfaction with a total mean of (4.33). Also, data showed patients have a high level of satisfaction for each patient’s satisfaction subscales were as follows:
For the Tangibles subscale, the total mean equals (4.28) and standard deviation is (0.73), "clean smart staff" has the highest satisfaction with a mean of (4.53) and a standard deviation of (0.55), as illustrated in the Figure 1.
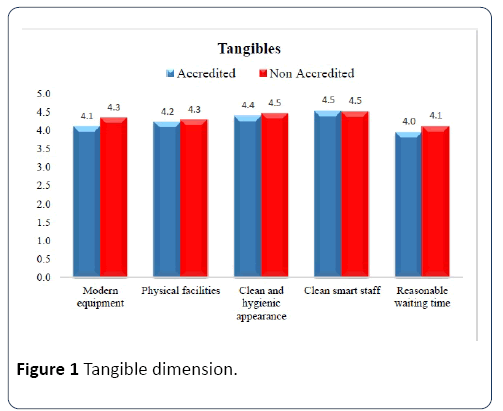
Figure 1: Tangible dimension.
Reliability subscale had a mean equalling (4.43) and a standard deviation of (0.67). "Sympathetic attendance to patients" has the highest satisfaction with a mean of (4.55) and a standard deviation of (0.61), as illustrated in the Figure 2.
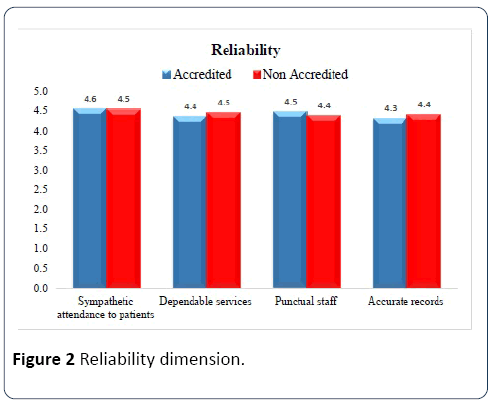
Figure 2: Reliaility dimension.
In the Responsiveness subscale, the total mean equals (4.22) and the standard deviation is (0.82). "Staff always willing to help" has the highest satisfaction with a mean of (4.39) and a standard deviation of (0.73), as illustrated in the Figure 3.
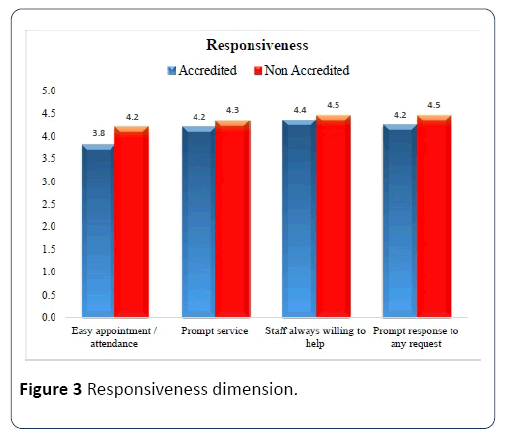
Figure 3: Responsiveness dimension.
The Assurance subscale’s total mean equals (4.42) and the standard deviation is (0.63). "Polite staff" has the highest satisfaction with a mean of (4.51) and a standard deviation of (0.60), as illustrated in the Figure 4.
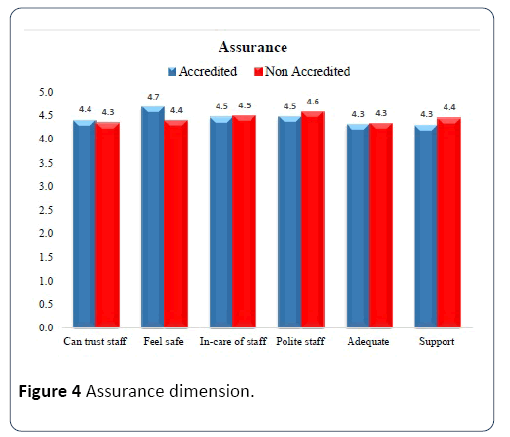
Figure 4: Assurance dimension.
For the Empathy dimension, the total mean equals (4.30) and the standard deviation is (0.68). "Individual attention to patients" has the highest satisfaction with a mean of (4.39) and a standard deviation of (0.65) as shown in the Figure 5.
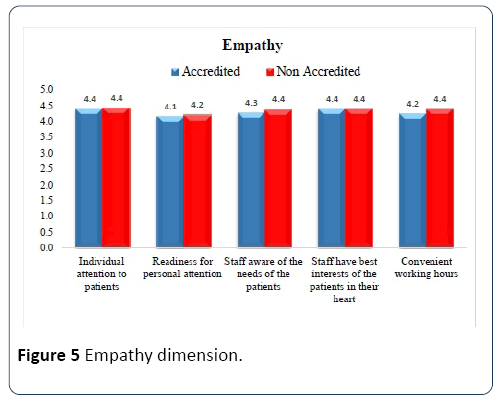
Figure 5: Empathy dimension.
Figure 6 indicates that patients’ satisfaction in nonaccredited hospitals was slightly more than in accredited hospitals, where the total mean for accredited hospitals is (4.33) and the total mean of satisfaction for non-accredited hospitals is 4.40. Moreover, for all subscales, patients have more satisfaction in the non-accredited hospital than in the accredited one.
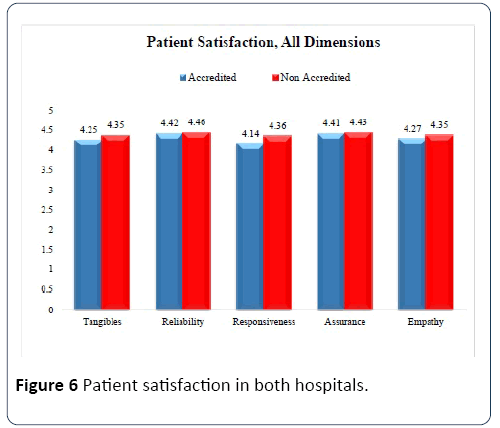
Figure 6: Patient satisfaction in both hospitals.
In the accredited hospital, all questions rate more than 85% except three questions: “Easy appointment” (71.6%), “Reasonable waiting time” (75.2%) and “Modern Equipment” (82.6%). For the Non-accredited hospital, all questions rate more than 90% except two questions: “Easy appointment” (86%) and “Reasonable waiting time” (86%).
Testing hypothesis
Table 2 indicates that there are no statistically significant differences at the level (P ≤ 0.05) between the means of patient satisfaction attributed to accreditation status. On the other hand, that there are no statistically significant differences between the means of a patient’s satisfaction subscales (tangibles, Reliability, Assurance, Empathy) related to accreditation status at level (P ≤ 0.05) where the p-values equal (0.126, 0.609, 0.644, 0.282) respectively. However, there are significant differences the level (P ≤ 0.05) between the means of patient’s satisfaction subscale (responsiveness) attributed to accreditation status. The differences in responsiveness were in favour of the non-accredited hospital, with a higher mean of satisfaction for the non-accredited hospital compared to the accredited hospital.
Table 2 Patient satisfaction according to accreditation status (T-test).
| Variables |
Patient Satisfaction |
| Mean |
T- value |
P-value |
Interpretation |
| Accreditation Status |
Accredited |
103.51 |
-1.432 |
0.153 |
Accept |
| Non-Accredited |
105.34 |
The results indicated that there are statistically significant differences at the level (P ≤ 0.05) between the means of patient satisfaction relating to patient demographic characteristics (with the exception of gender).
The study shows that there are no significant differences at the level (P ≤ 0.05) between the means of patient satisfaction relating to organizational factors.
Discussion
Patient satisfaction in accredited and nonaccredited hospitals
Patients who participated in the study showed a high level of satisfaction in both hospitals with a total mean of (4.33). The means of the results of all questions ranged from 3.95 to 4.53. These findings are compatible with study conducted by Ajarmah et al. [28] which states that, regardless to the hospitals type, the patient satisfaction level that was reflected was acceptable, since all the question results were above the mean of the scale (3); this ensures us that the patient who participated in this study perceived that they had received an acceptable level of services quality in both hospitals. The study findings showed differences in patient satisfaction levels; the findings indicated that the Non-accredited hospital has higher patient satisfaction score. The order of the patient satisfaction dimensions was as follows: Reliability, Assurance, Empathy, Tangible and the Responsiveness. Of the accredited and nonaccredited hospitals, regarding the responsiveness dimension, the non-accredited hospital was more favourable from patients’ perspectives.
The reliability dimension is considered an important dimension that influences the patient satisfaction [28]. Regarding this dimension, the mean of patient satisfaction was high; the lowest score across this dimension for the accredited hospital was “accurate records” and “punctual staff” for the non-accredited hospital. In the assurance dimension, the findings were relatively close in both accredited and nonaccredited hospitals. The lowest score in this dimension for the accredited hospital, was in “staff support to patients” and the causes for that may be relating to the heavy workloads. On the other hand, in the non-accredited hospital, it was in “adequate services provided by the hospital”, and this may refer to the financial issues, whereas the hospital services provided to the patients were based on the amount of payment. Another thing affecting patient satisfaction regarding this dimension is the hospital’s flexibility and willing to provide healthcare services [30]. Regarding the empathy dimension, the findings were close, and the lowest mean across the two hospitals was in regards to “readiness to personal attention”. This may refer to the weakness of patient-centred care culture in both hospitals, a point that helps in building trust in the provider-patient relationship and constructing the treatment plan well [31,32]. Patient satisfaction regarding the tangible dimension in both hospitals the lowest score was given to “Reasonable waiting time”, which according to the literature has a significant influence on patient satisfaction, and makes the patient less satisfied with the services provided [33]. This waiting time may be accounted for by the heavy workload on the hospitals, old hospital design and lack of hospitals’ financial resources. Finally, regarding the responsiveness dimension, patients in both hospitals were not highly satisfied with “easy appointment/attendance”, where the mean was 4.19 in the non-accredited hospital and 3.81 in the accredited hospital which may refer to heavy workload, difficulty of accessing hospitals from Gaza patients into West bank and West bank patients into Jerusalem, high bed occupancy rate, ineffective communication between the hospital and the patients, in addition to increased demand on hospital services.
The patient satisfaction attributed to accreditation status
The study findings showed that there are no significant differences at the level (P ≤ 0.05) between the means of patient satisfaction attributed to accreditation status. This means that accreditation status doesn’t affect or influence patient satisfaction level. These findings are consistent with the results of the Almasabi study [6] that found no clear evidence that healthcare accreditation improves patient satisfaction. The findings are also consistent with those of Sack et al. [3,32] who concluded that accreditation is not linked to better quality of care, and those who found no difference in patient satisfaction between accredited and non-accredited hospitals. Haj-Ali [2] also found no statistically significant differences between patient satisfaction and accreditation classification, and also the study of Heuer [25] displayed no relationship between accreditation and patient satisfaction.
These findings also may have to do with the fact that the accredited hospital that participated in this study is newly accredited by JCI, and the benefits of the accreditation program may touch on the structure, process, uniformity of care, access to care, safety culture and safety environment, but are still not visible to the patient. The non-accredited hospital that participated in this study has a strong system of evaluating patient satisfaction through daily random sampling, which is carried out by the patient satisfaction officer available in the hospital, who would have been assigned to collect the data about the patient satisfaction and follow up the hospital survey findings with hospital management to improve the process which scored least satisfaction from patients’ perspective. In addition, all patients planned for discharge from the hospital were asked by the medical secretary to fill the patient satisfaction questionnaire developed by the hospital for the evaluation of the services provided to them during hospitalization. Additionally, the findings showed that there are no significant differences between the means of a patient’s satisfaction subscales (Tangibles, Reliability, Assurance, and Empathy) concerning accreditation status. These findings were consistent with the findings of Haj-Ali [2], who stated that there is no significant relationship between the four dimensions of patient satisfaction, including reliability, assurance, responsiveness and empathy.
However, there are significant differences level (P ≤ 0.05) between the means of patients’ satisfaction dimension of (responsiveness), which are attributed to accreditation status. The differences in responsiveness were in the advantage of the non-accredited hospital, which had a higher mean of satisfaction than the accredited one. These findings are compatible with the study findings of [20] who concluded that the least satisfaction was in the responsiveness dimension. According to Jardali et al. [26] the accreditation program was designed to improve the quality of healthcare services, quality of care and patient satisfaction. However, these findings may reflect how the accreditation standards are focused on improving the process of care rather than the outcome, which are not tangible by the patient.
Conclusion
The findings of the study showed that patients at both accredited and non-accredited hospitals have a high level of satisfaction, more so in non-accredited hospitals. The study indicates that there are no significant differences between the means of patient satisfaction attributed to accreditation status.
Further Studies
The study rates the patient satisfaction measurement as an important indicator in the healthcare system, so it is needed to conduct other studies to assess other quality indicators in hospitals, such as HAI’s rates, TAT for procedures, re-do surgeries, readmission within 30 days w… etc. Also, since the accreditation of hospitals is still not prevalent, and many hospitals plan to achieve JCI accreditation, the researcher suggests conducting studies comparing hospitals’ indicators before and after accreditation to assess the impact of accreditation on those hospitals.
22000
References
- Al-Tehewy M, Salem B, Habil I, El-Okda S (2009) Evaluation of accreditation program in non-governmental organizations' health units in Egypt: short-term outcomes. Int J Quality Health Care 21: 183-189.
- Haj-Ali, W, Karroum LB, Natafgi N, Kassak K (2014) Exploring the relationship between accreditation and patient satisfaction–the case of selected Lebanese hospitals. IJHPM 3: 341-346.
- Sack C, Scherag A, Lutkes P, Günther W, Jockel KH, et al. (2011) Is there an association between hospital accreditation and patient satisfaction with hospital care? A survey of 37 000 patients treated by 73 hospitals. Int J Quality Health Care 23: 278-283.
- Nicklin W (2014) The value and impact of health care accreditation: A literature review.
- Mahran SM, Nagshabandi E (2016) Oncology patients’ satisfaction towards quality health care services at Accredited University Hospital. Am J Nursing 5: 162-168.
- Almasabi M, Yang H, Thomas S (2014) A systematic review of the association between healthcare accreditation and patient satisfaction. World App Sci J 31: 1618-1623.
- Parasuraman A, Zeithaml VA, Berry LL (1985) A conceptual model of service quality and its implications for future research. J Marketing 49: 41-50.
- Al-Qahtani MF, Al-Dohailan SK, Al-Sharani HT, Al-Medaires MA, Khuridah EN, et al. (2012) The impact of the status of hospital accreditation on patient satisfaction with the Obstetrics and Gynecology Clinics in the Eastern Province, Saudi Arabia. J Med Med Sci 3: 665-673.
- Sprague L (2005) Hospital oversight in Medicare: accreditation and deeming authority. NHPF Issue Brief 6: 1-15.
- Boyer L, Francois P, Doutre E, Weil G, Labarere J (2006) Perception and use of the results of patient satisfaction surveys by care providers in a French teaching hospital. Int J Quality Health Care 18: 359-364.
- Almeida RSD, Bourliataux-Lajoinie S, Martins M (2015) Satisfaction measuremen instruments for healthcare service users: a systematic review. Cadernos de saudepublica 31: 11-25.
- Doyle C, Lennox L, Bell D (2013) A systematic review of evidence on the links between patient experience and clinical safety and effectiveness. BMJ open 3: e001570.
- Lavela SL, Gallan A (2014) Evaluation and measurement of patient experience. Patient Exp J 1: 28-36.
- Al-Abri R, Al-Balushi A (2014) Patient satisfaction survey as a tool towards quality improvement. Oman Med J 29: 3-7.
- Anbari Z, Tabaraie Y (2013) Measurement of quality of hospital services via SERVQUAL Model. Bull Env Pharmacol Life Sci 3: 51-56.
- Afzal M, Rizvi F, Azad AH, Rajput AM, Khan A, et al. (2014) Effect of demographic characteristics on patient’s satisfaction with health care facility. JPMI 28: 154-160.
- Bacon CT, Mark B (2009) Organizational effects on patient satisfaction in hospital medical-surgical units. J Nursing Administration 39: 220.
- Quintana JM, González N, Bilbao A, Aizpuru F, Escobar A, et al. (2006) Predictors of patient satisfaction with hospital health care. BMC Health Serv Res 6: 102.
- Wolf A, Olsson LE, Taft C, Swedberg K, Ekman I (2012) Impacts of patient characteristics on hospital care experience in 34,000 Swedish patients. BMC Nursing 11: 8.
- Hayati IN, Azimatun NA, Rozita H, Ezat WS, (2010) In-patient’s satisfaction in the medical and surgical wards-A comparison between accredited and non-accredited hospital in the state of Selangor. Jurnal Kesihatan Masyarakat 16: 60-68.
- Husted H, Holm G, Jacobsen S (2008) Predictors of length of stay and patient satisfaction after hip and knee replacement surgery: fast-track experience in 712 patients. Actaorthopaedica 79: 168-173.
- Borghans I, Kleefstra SM, Kool RB, Westert GP (2012) Is the length of stay in hospital correlated with patient satisfaction? Int J Quality Health Care 24: 443-451.
- Drost EA (2011) Validity and reliability in social science research. Educ Res Perspect 38: 105.
- Kraska RA, Weigand M, Geraedts M (2016) Associations between hospital characteristics and patient satisfaction in Germany. Health Expect 20: 593-600.
- Heuer AJ (2002) Testing the relationship between measures of patient satisfaction and hospital accreditation ratings. Seton Hall University Dissertations and Theses (ETDs). pp: 1-121.
- El-Jardali F, Hemadeh R, Jaafar M, Sagherian L, El-Skaff R, et al. (2014) The impact of accreditation of primary healthcare centers: successes, challenges and policy implications as perceived by healthcare providers and directors in Lebanon. BMC Health Services Res 14: 86.
- Foster DP, Zrull L (2013) Hospital performance differences by size and teaching status. 100 Top Hospitals: Study Overview (20th edn). Truven Health Analytics.
- Ajarmah BS, Hashem TN (2015) Patient satisfaction evaluation on hospitals; Comparison study between accredited and non-accredited hospitals in Jordan. Eur Scientific J 11: 298-313.
- Soufan S (2015) Prevalence of acute stress disorder among women after emergency caesarean section in Ramallah area, Al-Quds University.
- Owusu-Frimpong N, Nwankwo S, Dason B (2010) Measuring service quality and patient satisfaction with access to public and private healthcare delivery. Int J Public Sector Management 23: 203-220.
- Widmar SB (2012) Satisfaction with patient-centered care and self-care education in left ventricular assist device patients. Vanderbilt University, Tennessee. pp: 1-189.
- Sack C, Lütkes P, Günther W, Erbel R, Jöckel KH, et al. (2010) Challenging the holy grail of hospital accreditation: A cross sectional study of inpatient satisfaction in the field of cardiology. BMC Health Serv Res 10: 120.
- Kreitz TM, Winters BS, Pedowitz D (2016) The influence of wait time on patient satisfaction in the orthopedic clinic. J Patient Experience 3: 39-42.
- Joint Commission International (2016) Joint commission international accreditation, overview.

