Keywords
Encephalitis; Herpes simplex virus; Meningioma; Post-operative
Introduction
Herpes simplex virus (HSV) encephalitis is the most common form of sporadic viral encephalitis [1]. It can manifest at any time of the year, in patients of all ages, and is associated with significant morbidity and mortality [2-5]. HSV usually begins as a febrile illness with symptoms of diffuse and focal cerebral involvement, such as headaches, personality changes, obtundation, focal seizures and paresis [6,7]. Postoperative herpes simplex encephalitis has been rarely described. HSV encephalitis is an extremely life-threatening consequence of the HSV infection of the central nervous system. It is said that the HSV encephalitis is extremely rare, and only a minority of individuals return to normal functions. Antiviral therapy is most effective when early, necessitating prompt diagnosis started.
Actually, preventing the inflammation of spreading from a small area of the brain inflammation to a bigger involved area is an extremely important issue. In fact, of all different types of viral encephalitis, HSV encephalitis is one of the few viral causes of diseases for which we actually have accurate diagnostic tests and relatively cheap treatments already available [8].
The necessity for treatment is dictated by factors such as age, the immune system function, the type and severity of the disease, or mild cases- the amount of stress the condition causes [9]. The occurrence of HSV encephalitis after neurosurgery is rare and only a small number of cases have been reported in the literature. In this report we represent a rare case of HSV encephalitis in a 55-year-old man.
Methods and Materials
Case report
Intracranial infections following neurosurgery are most commonly caused by bacteria. Postoperative herpes simplex encephalitis has been described rarely before. Herpes simplex virus encephalitis is a life-threatening consequence of HSV infection of the central nervous system. Only a minority of individuals return to normal functions when faced by this disease (Table 1). Antiviral therapy is most effective when early, necessitating prompt diagnosis is started.
| Author and year |
Age/Sex |
Kind of Operation |
Symptoms |
Confirming Test Result |
Treatment |
outcome |
R Filipoet al.
2005 |
33/male |
Resection of acoustic neuroma |
Strong headache, impairment of consciousness and hypertonia of arms and legs |
Positive PCR HSV 1 DNA of CSF |
High dose antiviral therapy |
|
Raper DM et al.
2011 |
65/female |
C2-C5 laminectomy for spinal ependymoma resection |
fever, vomiting and rapid decline in mental status |
Positive PCR HSV 1 DNA of CSF |
High dose antiviral therapy |
Discharged after VP shunting and placing PEG and tracheostomy |
Kwon JW et al.
2008 |
13/female |
surgery for craniopharyngioma |
rapid deterioration in mental status |
Positive PCR HSV 1 DNA of CSF |
High dose antiviral therapy |
She recovered and could speak short sentences, but dysphasia and right hemiparesis remained |
A Spuler et al.
1999 |
78/female |
removal of a meningioma |
difficulties talking and counting while playing cards, followed by several focal motor seizures involving first the right face and later the arm and leg |
Positive PCR HSV 1 DNA of CSF |
High dose antiviral therapy |
Died nine days after the onset of symptoms |
S Aldea et al.
2003 |
28/male* |
Removal of a right frontocingularoligodendroglioma. |
fever, rightsidehemiparesis, meningeal syndrome, and mild motor aphasia |
Anti-HSV-IgG and IgM level |
High dose antiviral therapy |
Full recovery after one year |
Bourgeois et al.
1999 |
8/male** |
Left amygdalohippocampectomy for intractable complex partial seizure |
Severe clinical deterioration with partial statausepilepticus, aphasia and hyperthermia |
Positive PCR HSV 1 DNA of CSF |
High dose antiviral therapy |
Full recovery |
Jalloh et al.
2009 |
44/male |
Acoustic neuroma |
Pyrexia, vomiting, confusion |
Positive PCR HSV 1 DNA of CSF |
High dose antiviral therapy |
Good recovery |
Kim et al.
2013 |
11/male*** |
Epilepsy surgery for intractable seizure for 6 years |
Fever and confusion |
Positive PCR HSV 1 DNA of CSF |
High dose antiviral therapy |
Normal recovery one month after being discharged |
Hon Tang et al.
2013 |
29/F |
Right sided micro vascular decompression for trigeminal neuralgia |
Fever, headache and confusion |
Positive PCR HSV 1 DNA of CSF |
High dose antiviral therapy |
Good recovery after 2 weeks |
*Possible episode of viral encephalitis in 1995
**The patient had previously contracted HSV 1 meningo-encephalitis at the age of 16 months
***Past medical history of HSV encephalitis at the age of five
Table 1 Literature review of postoperative HSV encephalitis
In this study we represent a rare case of HSV encephalitis. After diagnosing convexity meningioma in a 55-year-old man, the patient underwent uneventful surgery for the removal of meningioma (Figure 1).
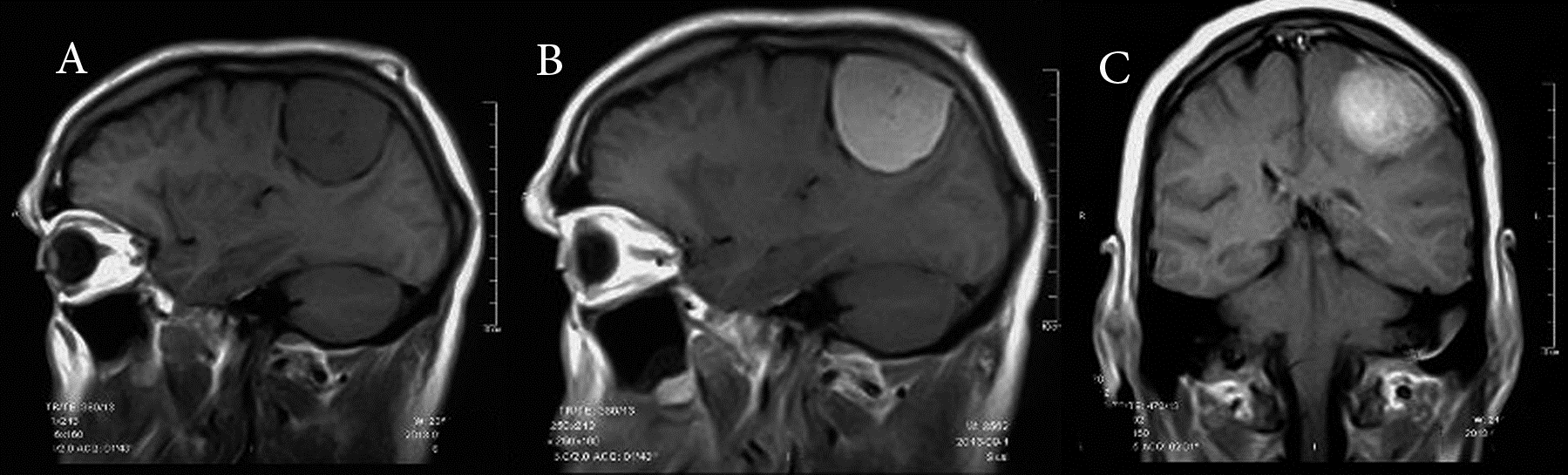
Figure 1: Pre-operative: MRI of the Brain showing the mass studied
The patient was awoken and was responsive after the surgery. The appearance of a high grade fever (40°C) and altered consciousness and spastic quadriparesis complicated the post-operative course 48 hours after surgery. Neurological exam was done, but there was not any specific finding. Laboratory findings were normal. The brain MRI detected brain abnormalities on the fourth day after the onset of symptoms, signal changes in left insula and temporal lobe and also in both sides of basal ganglia were detected as a sign of infarction (Figure 2).
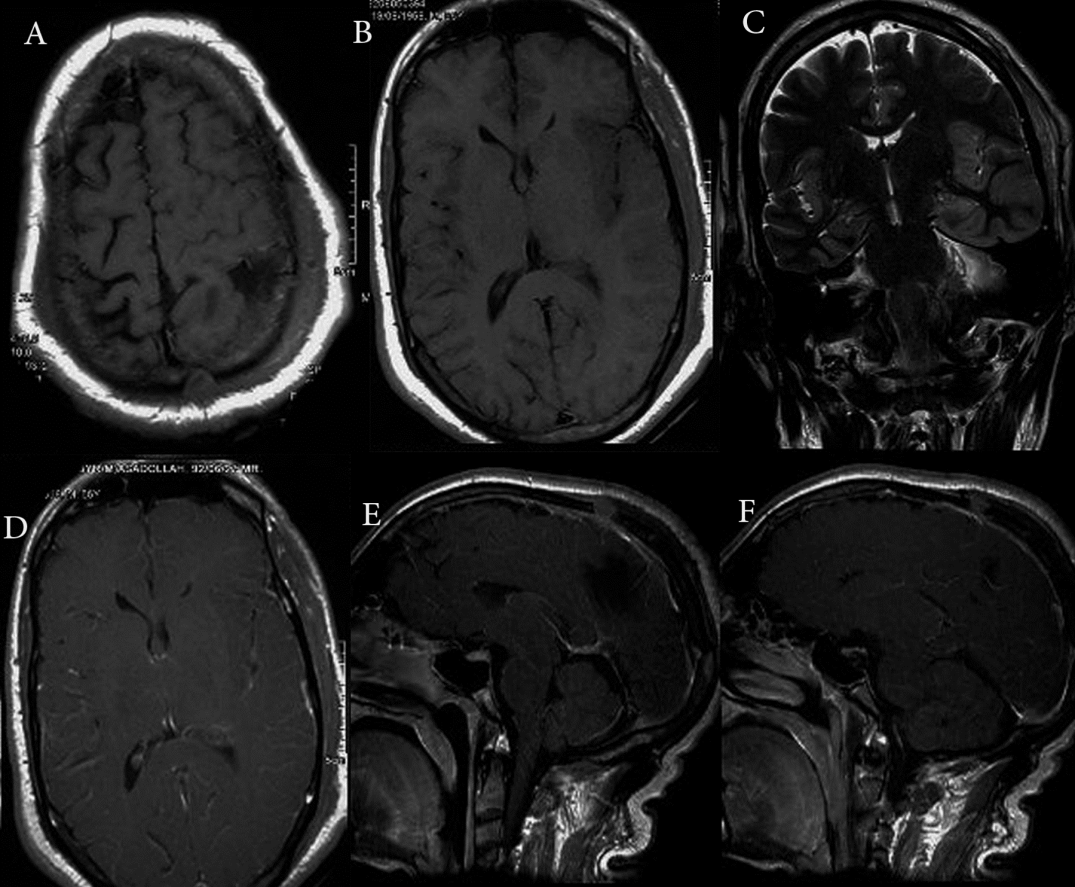
Figure 2: Post-operative: Magnetic resonance imaging of the brain reveals, signal changes in the left insula and temporal lobe and also in both sides of basal ganglia as a sign of infarction
Real-time Polymerase chain reaction identification of HSV 1 DNA by DNA extraction in the CSF sample confirmed the diagnosis. A positive prognosis was achieved due to the decision to start specific, high-dose antiviral therapy based on clinical suspicion, before a firm diagnosis was established. (30 mg/kg/day intravenous Acyclovir) Treatment with acyclovir was maintained for 8 weeks but unfortunately the patient died after severe sepsis.
Discussion
Herpes simplex virus-1 is the most common cause of lethal sporadic encephalitis. HSV-1 encephalitis is associated with persistent severe neurological deficits, although improved therapy with intravenous acyclovir has been adopted recently [2-4]. Encephalitis caused by HSV is not common. In fact the estimated incidence, derived from large series, is 2 to 4 cases per million populations per year [10]. The differential diagnosis of HSV encephalitis is extensive [11]. It includes such infectious conditions as bacterial abscess, empyema, listeriosis, mycobacterial infection, fungal infection (especially Cryptococcus), parasitic infection (toxoplasmosis, amoebic infection), other viral infections (Epstein-Barr virus, lymphocytic choriomeningitis virus, influenza virus, enterovirus, rabies, subacute sclerosing panencephalitis , arboviruses, adenovirus, rubella virus), and noninfectious conditions such as vascular malformations, tumors, and Reye syndrome [10,12]. This wide range of possibilities makes it impossible to treat empirically without more definitive diagnostic evaluations.
It has also been mentioned that postoperative infections that occur as complications of neurosurgical procedures are originally bacterial and include meningitis, subdural empyema, and cerebral abscess [2]. It has also been proven that HSV infection has a genetic immune etiology in which a deficiency exists in a protein or a toll-like receptor that helps mediate an immune response [3].
Finally it can be said that there are only few case repots of postoperative HSV 1 encephalitis. These reports suggest that this rare postoperative complication is associated with a poor prognosis, with high mortality and morbidity. Neurosurgical interventions involving peripheral nerve root or ganglia have been reported to cause reactivation of cutaneous herpes simplex infection. Factors compromising the immune system may also increase susceptibility to herpes infection, so does previous HSV infection.
Conclusion
To conclude, the most significant factor affecting the HSV encephalitis outcome is starting effective antiviral treatment as early as possible [13]. Although HSV encephalitis is rare, mortality rates reach 70% in the absence of therapy and only a minority of individual’s return to normal functions. So considering the possibility of HSV encephalitis in case of decreased level of consciousness and high grade fever after neurosurgical operations is logical. Owing to the lifethreatening nature of the disease, if there is a delay in diagnostic test results therapy should not be withheld until they become available. It means empirical acyclovir treatment13 is strongly recommended when encephalitis is suspected [4,14]. After the completion of therapy, PCR of the CSF can confirm the elimination of replicating virus, aiding further management of the patient. Unfortunately, despite all the improvements in the diagnosis and treatment of this disease, but there is still many failures. Actually, about 30% of patients with HSV encephalitis result in poor prognosis [15,16].
Conflict of Interest
All authors certify that they have NO affiliations with or involvement in any organization or entity with any financial interest, or non-financial interest in the subject matter or materials discussed in this manuscript.
“There is no funding or conflict of interest”
“There are no financial disclosures”
9133
References
- Lund M (2011) Herpes simplex virus reactivation and encephalitis after topectomy. J Pediatr Health Care 25: 323-327.
- Aldea S, Joly LM, Roujeau T, Oswald AM, Devaux B (2003) Post-operative herpes simplex virus encephalitis after neurosurgery: case report and review of the literature. ClinInfect Dis 36: e96-e99.
- Casrouge A, Zhang SY, Eidenschenk C, Jouanguy E, Puel A, et al. (2006) Herpes simplex virus encephalitis in human UNC-93B deficiency. Science 314: 308-312.
- Tunkel AR, Glaser CA, Bloch KC, Sejvar JJ, Marra CM, et al. (2008) The management of encephalitis: clinical practice guidelines by the Infectious Diseases Society of America. ClinInfect Dis 47: 303-327.
- Yamada S, Kameyama T, Nagaya S, Hashizume Y, Yoshida M (2003) Relapsing herpes simplex encephalitis: pathological confirmation of viral reactivation. J Of NeurolNeurosurg Psychiatry 74: 262-264.
- Mckendall RR (1989) Herpes simplex virus infections of the nervous system. Handbook of clinical neurology Revised series 12: 207-227.
- Jhun P, Bright A, Herbert M (2014) Don't let herpes melt your brain. Annals of Emergency Medicine 64: 589-590.
- Jones CA, Isaacs D (2004) Management of herpes simplex virus infections. Current Paediatr 14: 131-136.
- Skoldenberg B, Forsgren M, Alestig K, Bergstrom T, Burman L, et al. (1984) Acyclovir versus vidarabine in herpes simplex encephalitis-Randomisedmulticenter study in consecutive Swedish patients. Lancet 2: 707-711.
- Kohl S, James AR (1985) Herpes simplex virus encephalitis during childhood: Importance of brain biopsy diagnosis. J Pediatr 107: 212-215.
- Whitley RJ, Soong SJ, Linneman C Jr, Liu C, Pazin G, et al. (1982) Herpes simplex encephalitis. Clinical Assessment. JAMA 247: 317-320.
- Kimberlin DW (2007) Management of HSV encephalitis in adults and neonates: Diagnosis, prognosis and treatment. Herpes : TheJournal of the IHMF 14: 11-16.
- Steiner I, Budka H, Chaudhuri A, Koskiniemi M, Sainio K, et al. (2010) Viral meningo-encephalitis: a review of diagnostic methods and guidelines for management. Eur JNeurol 17: 999-957.
- Kamei S, Sekizawa T, Shiota H, Mizutani T, Itoyama Y, et al. (2005) Evaluation of combination therapy using aciclovir and corticosteroid in adult patients with herpes simplex virus encephalitis. J NeurolNeurosurg Psychiatry 76: 1544-1549
- Raschilas F, Wolff M, Delatour F, Chaffaut C, De Broucker T, et al. (2002) Outcome of and prognostic factors for herpes simplex encephalitis in adult patients: results of a multicenter study. ClinInfect Dis 35: 254-260.

