Keywords
Anemia; Iron; Folic acid; Food security
Introduction
Anaemia is a condition in which the number of red blood cells is insufficient to meet the physiological needs in an individual or the oxygen carrying capacity of red blood cells is impaired which vary by age, sex, altitude, smoking and pregnancy status (UNICEF & WHO (World Health Organization) [1-23]. Globally, iron deficiency is thought to be the most common cause of anemia, although other conditions such as folate, vitamin B12 and vitamin A deficiencies, chronic inflammation, parasitic infections among others contribute to the burden of anemia [23].
Anemia in pregnancy reduces tolerance to blood loss and leads to impaired function and cardiac failure. Anemia prevalence data remains an important indicator in public health since anemia is related to morbidity and mortality in the population groups usually considered to be the most vulnerable especially pregnant women and children under five years [9].
Anemia is the result of one of the most prevalent micronutrient deficiencies in women; its consequences include impaired health and well- being and increased risk of maternal and neonatal adverse outcomes [11]. It was observed that 42% of women in Ghana are anemic, 32% are mildly anemic, 10% are moderately anemic and less than 1% are severely anemic and Anemia among pregnant women was 45% [11].
There is high prevalence of anemia among pregnant women in Ghana. According to the 2014 Ghana Demographic and Health Survey, the prevalence of anemia is highest (48%) among youngest women aged 15-19. Even among women aged 30-39years who are said to record the lowest prevalence, anemia among them is still as high as 39%. Anemia among pregnant women is similar to that among lactating women (45%) and slightly higher than non- pregnant or breastfeeding mothers (41%) [11]. The Wassa East District has a high teenage (10-19yrs) pregnancy rate of 18% which explains partly the reason for high anemia prevalence among pregnant women.
The prevalence of anemia in Wassa East district rose from 25% in 2016 to 30% in 2017. Also, anemia at 36 weeks of pregnancy has seen a marginal decline from 2016 to 2017 (29% to 24 % respectively) [10]. Anemia prevalence continue to soar despite the interventions – Iron and folic acid supplementation, deworming, Intermittent Preventive therapy with Sulphurdoxine pyrimethamine and distribution and use of Long-Lasting Insecticide nets (LLIN) put in place by the Ghana Health Service for pregnant women to help address the situation.
Iron deficiency anemia (IDA) is a public health concern globally, as it affects 17% of women [12]. Most of the burden occurs in low-resource settings in Southeast Asia and Africa largely because of poverty, poor dietary intake and high burden of diseases. Iron deficiency anaemia impairs health and well-being in women and is associated with adverse reproductive outcomes such as maternal deaths. 24% of perinatal deaths around the world are attributed to IDA [12]. Maternal IDA is associated with congenital birth defects, small for gestational age births, low birth weight infants and growth impairment in infants, and is a major contributor to disability adjusted life years in women [12].
The factors which predispose pregnant women to anemia and the gestation at which anemia at which anaemia begins in during pregnancy has not been documented in the Wassa East District of Ghana. The study therefore sets out to determine the factors which predispose pregnant women to anemia [24-28].
Global burden of Anemia
Anaemia is the condition that develops when the body does not have enough healthy red blood cells or hemoglobin. Hemoglobin is the main part of the red blood cells that binds oxygen. When there are few or abnormal hemoglobin, cells in the body will not get enough oxygen [29]. The WHO defines anaemia as blood hemoglobin levels of less than 11g/dl. Symptoms include fatigue because the organs do not get enough oxygen to function efficiently. Some types of anemia are hereditary and may be passed on from parents to offspring’s. Women in child-bearing age are more susceptible to anemia because of blood loss during menstruation and the increase blood supply demands during pregnancy. Older adults are also susceptible because of poor diet and medical conditions [27]. Iron deficiency accounts for over fifty percent (50%) of all anemia globally, also anaemia is an indicator of poor nutrition and poor health [26]. Anemia is the second leading cause of disability and affects more than half of the population of preschool children and pregnant women in developing countries and about 40 to 50% in developed countries [26]. In poor malaria endemic countries, anemia is one of the major cause of mortalities in children under five years and pregnant women [27]. The 2011 multiple indicator cluster survey of Ghana estimate the prevalence of anemia in children less than five years to be 57%. However, males had a higher rate (60%) than females (53%) and there was variation between urban and rural settings, with urban areas having an anemia prevalence of 48% whereas rural areas had a prevalence of 64% [16]. The 2011 global prevalence of anemia report estimate that 42.6 % of women are anemic globally. Regional variations exist, with the African Sub-Region recording the highest anemia prevalence of 62.3%, followed by Southeast Asia region with 53.8% prevalence and the Americas is 22.3% [27]. Anemia is associated with sub-optimal work performance, reduced mental functioning, and productivity among adults [27]. This implies reduced earning capacity for the concerned individual and often times, the entire household. When pregnant women are anemic, in a resource-constrained environment such as Ghana, the effect on the individual and household economy can be enormous. Pregnant anemic women are more likely to produce anemic offspring, with its attendant effects of reduced cognitive capacity, psychomotor challenges, and behavioral anomalies, which are sometimes lifelong [17]. This exerts additional strain on the household and community resources, available for childcare. Due to its adverse health and associated consequences, particularly increased infant and maternal morbidity and mortality, maternal anemia should be controlled through intersectional action. The poor socioeconomic conditions and health-related factors, predisposing to anemia and iron deficiency in women and children, are underlying issues that need to be considered, if sustainable progress will be made in reducing maternal and child morbidity. Food security aids in the realization of dietary diversification, at the individual and household levels. The importance of dietary diversity and nutrient adequacy in pregnancy need to be emphasized in program planning, implementation, and evaluation, especially as it relates to community-level programs, which have a potential to reach all pregnant and lactating women, in order to optimize their health and wellbeing, as well as those of their babies in utero.
Anemia is a major factor in women’s health, especially reproductive health in developing countries. Severe anemia during pregnancy is an important contributor to maternal mortality, as well as to the low birth weight which is in turn an important risk factor for infant mortality [26]. Even moderate Anemia makes women less able to work and care for their children. The causes of anaemia are multi- factorial, including diet, infection, and genetics, and for some of the commonest causes of anaemia there is good evidence of the effectiveness of simple interventions: for example, iron supplementation, longlasting insecticide nets and intermittent preventive treatment for malaria [27]. Human hookworm infection results in intestinal blood loss which, in turn, can contribute to anaemia [5].
Progress on reducing the incidence of anaemia has been made in some regions, while further improvements are still needed in others. At a global level, in all age and gender groups, anaemia is estimated to have decreased roughly seven percentage points between 1990 and 2010, from 40% to 33% [2]. During roughly the same period (1995 to 2011), anaemia was estimated to have decreased by 4–5 percentage points in the three highestrisk groups (children aged under 5 years, pregnant women, non- pregnant women of reproductive age) [3]. At a regional level, Africa (central and west, and east) and south Asia had the lowest mean hemoglobin concentrations, as well as the highest prevalence of anaemia among high-risk groups in both 1995 and 2011, despite significant improvements for children in the African regions (larger than in any other region). No improvement was seen among some groups with low hemoglobin levels and high prevalence of anaemia in 1995, including non-pregnant women in West Africa, central Asia, the Middle East and North Africa, and pregnant women in southern Africa and south Asia. Hemoglobin concentrations among children appear to have declined in southern Africa, while the largest improvements in women’s hemoglobin levels were seen in central America and the Caribbean, east Africa, east and south-east Asia and Oceania [23]. The global average of the prevalence of anaemia in women of reproductive age increased slightly between 2005 and 2016, although the increase was not statistically significant. It declined from 42% to 38% in Africa and from 25% to 22% in Latin America and the Caribbean, although this was offset by slight increases in all other regions [14].
Effects of anaemia in pregnancy
Iron deficiency (low serum ferritin and sparse or absent of iron in bone marrow) anaemia in pregnancy is a risk factor to preterm delivery and subsequent low birth weight and compromises the health status of the neonate and the pregnant mother. Evidence indicates that maternal iron deficiency in pregnancy reduces fetal iron stores; perhaps well into the first year of life. This deserves further exploration because of the tendency of infants to develop iron deficiency anemia and because of the documented adverse consequences of this condition on infant development. During pregnancy, there is substantial increase in the demands of iron because part of it is transferred into the fetus through the placenta for the growth and development of the foetus and as such a women who enters pregnancy with inadequate stores of iron might become anaemic at advanced stages of the pregnancy because of this increasing demand. Anaemia is associated with increase in maternal and child morbidities and mortalities [28,29]. Severe or untreated anemia in pregnancy can increase the risk of having preterm or low birth weight baby, blood transfusions as a result of significant blood lose during delivery, post-partum depression and developmental delays in babies [30].
Vitamin C is known to affect iron metabolism, particularly enhancing absorption of non-haem iron, but also increasing mobilization of iron from stores. Vitamin C deficiency can also contribute to hemolysis, through oxidative damage to erythrocytes and also capillary hemorrhaging leading to blood loss. Populations at risk of vitamin C deficiency include pregnant women, infants fed exclusively with cow’s milk, the elderly, and smokers. Vitamin C supplementation has been shown to increase haemoglobin concentration and serum ferritin in children and non-pregnant women [19]. Low levels of vitamin D have been associated with anaemia in children and adults from the USA, and individuals with chronic kidney disease, end-stage heart failure, and type 2 diabetes from several countries. The mechanism linking vitamin D deficiency to decreased hemoglobin concentration is not entirely understood, but there is evidence indicating that low levels of vitamin D may lead to decreased local calcitriol production in the bone marrow, which may limit erythropoiesis [13].
Anaemia associated with vitamin E deficiency is characterized as a hemolytic anaemia, owing to the protective effect of vitamin E on polyunsaturated fatty acids in the membranes of red blood cells. Deficiency of vitamin E is thought to be largely limited to premature and low-birth-weight infants, and individuals with pathological malabsorption syndromes, as vitamin E is common in foods, particularly vegetable and seed oils. Vitamin E is routinely provided to premature/low-birth-weight infants in high-income countries, to avoid anaemia of prematurity [24].
Methodology
The study design was cross-sectional. Pregnant women in Wassa East were interviewed and their Hbs taken from their maternal health record books. The study was done in Daboase in the Wassa East District of the Western Region. Daboase is a cosmopolitan Community and the capital of the Wassa East District. The population of the district according to the 2010 population and housing Census with a projected growth rate of 2% is 100,741. The major economic activities are farming, trading, and fishing [11]. The district has a total of 30 health facilities which serves the health needs of the people.
Study population and inclusion criteria
The target population for this study was pregnant women assessing antenatal services at Health facilities in Wassa East District. Mothers who were in their first trimester and assessed ANC were recruited into the study. Also, mothers with preexisting health conditions such as sickle cell disease were not included in this study. The sample size for study participants (pregnant women in first trimester) were fifty (50). Women who are resident in the district were considered for this study.
Sampling method
Simple random sampling was used to recruit pregnant women into this study. Any pregnant woman who was resident in the district and was within the first trimester, who will stay in the district and assess health service until delivery was involved in this study after they consented. The recruitment and data collection took a period of one month. Expectant mothers who were in first trimester and visited the facility were qualified to be recruited into this study. Technique and tools Information was obtained from respondents using a structured interviewer administered questionnaire. The consent of the mothers was sought before the commencement of the questionnaire administration. Mothers who were identified to be eligible were invited orally, to partake in the study. Eligible participants were interviewed at their own place and time of convenience.
Before commencement of the data collection, research assistants were recruited and orientated. They were sensitized on the purpose of the research, the focus of the research, the administration of completing questionnaires, and handling of unresponsive interviewees during the process. The structured questionnaires were then distributed to the research assistants for administration over a period of one month. The questionnaires consisted of three sections. The first part included questions on socio-demographic characteristics of respondents; the second part assessed food security and usage of Anaemia prevention interventions.
Data processing and analysis
The data entry and analysis were performed using International Business Management statistical package for social scientists (SPSS) version 22. Administered questionnaires were collated at the end of each day.
Data was edited and coded manually before entering computer software. The data was then analyzed on IBM – SPSS version 22. Dietary practices and Hb Anaemia status were presented with frequencies and percentages using tables. IBM-SPSS was used to compare the proportion- differences of dietary practices by type of demographic factors such age of respondents, level of education and marital status with 95 % confidence interval.
Ethical consideration
Ethical clearance to carry out this study was sought from the Wassa District Health Directorate. Permission was also obtained from the Nurses and all health Staff of Daboase and Ateiku. Informed consent was obtained from all participants after the objectives and the methodology of the study has been explained to them. Participation in the study was completely voluntary, no financial or material benefits were given and participants were told they could choose to withdraw from the study at will and at any time even if administration of questionnaire has started. The privacy and confidentiality of every participant were ensured throughout the study period.
Results
Characteristics of the sample
Fifty (50) expectant mothers were interviewed using structured questionnaires. They were selected randomly in health facilities in all the four sub-districts of the Wassa East District. Data was collected on their demographic characteristics, household food security, deworming, LLIN and SP us as well as the household dietary diversity where diet was classified according to the four -tar diet principle.
Table 1 depicts the major characteristics of expectant mothers sampled in this study. Teenagers who fall under 20 years were 11 (22.0%), 20-24 years were 12 (24.0%) each, those who were 25- 29 years were the majority of respondents, 17 (34%), 7(14.0%) were between 30-34 years, and a few 3(6.0%) were aged 35-39 years. The proportion of married women was (26.0%) whereas 74.0% were cohabiting.
The major religious denomination of pregnant women was Christianity (96.0%), whilst 2.0% of the respondents belonged to Islam and Traditional Religion respectively. The findings of the study also estimated that 52% of children were females with 48% being males.
Table 1 also shows the socio-demographic characteristics of mothers during the survey, majority (48.0%) of mothers completed Junior high school, whilst 26% had primary education. Majority (74.0%) of the respondents belonged to the lowest middle quintile whilst 26.0% belonged to the middle wealth quintile (Figure 1).
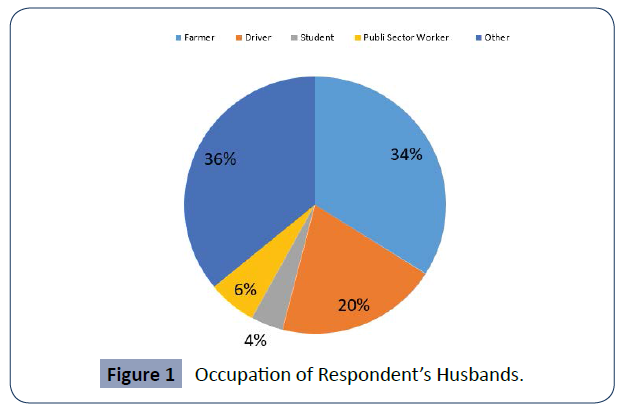
Figure 1 Occupation of Respondent’s Husbands.
| Attribute |
Frequency |
Percentage (%) |
| Age of respondents (in years) |
| >19 years |
11 |
22 |
| 20-24 |
12 |
24 |
| 25-29 |
17 |
34 |
| 30-34 |
7 |
14 |
| 35-39 |
3 |
6 |
| Total |
50 |
100 |
| Marital Status |
| Married |
13 |
26 |
| Cohabiting |
37 |
74.0 |
| Total |
50 |
100 |
| Religion |
| Christianity |
48 |
96 |
| Islam |
1 |
2 |
| Traditional |
1 |
2 |
| Total |
50 |
100 |
| Highest Education Completed |
| No Formal Education |
7 |
14 |
| Primary education |
13 |
26 |
| Junior High School |
24 |
48 |
| Senior High/Vocation/Technical |
6 |
12 |
| Total |
50 |
100 |
| Occupation |
| Farmer |
14 |
28 |
| Trader |
17 |
34 |
| Housewife |
1 |
2 |
| Student |
1 |
2 |
| Unemployed |
15 |
30 |
| Other |
2 |
4 |
| Total |
50 |
100 |
| Wealth Quintile |
| Low |
37 |
74 |
| Middle |
13 |
26 |
| Total |
50 |
100 |
| Number of people in a household |
| 1-4 people |
32 |
64 |
| 5-7 people |
18 |
36 |
| Total |
50 |
100 |
Table 1 Background and socio-demographic characteristics of respondents (n=50).
Food security
Table 2 below shows the trends of food security among pregnant women in the study. Using the past month as a reference point, 20% indicated that they were sometimes worried about their food not being adequate and 2% indicated they were worried more often about inadequate food availability in the household. Also, 8% mentioned that they sometimes are unable to eat the kind of foods needed whilst 4% said they are often unable to eat the kinds of foods they need in their households. Of the respondents, 4% indicated that they often eat the kinds of food they will prefer not to eat but due to unavailability of resources they are compelled to eat whatever is available and affordable. A total of 3 respondents representing 6% of the sample mentioned that they often eat smaller meals because of non-availability of resources to purchase food, 4% indicated that they sometimes go to bed hungry due to food unavailability.
| Food security situation |
Frequency |
Percentage (%) |
| Worried about food inadequacy in the past month |
| Never |
32 |
64 |
| Rarely |
7 |
14 |
| Sometimes |
10 |
20 |
| Often |
1 |
2 |
| Total |
50 |
100 |
| Unable to eat the kinds of foods needed |
| Never |
20 |
68 |
| Rarely |
10 |
34 |
| Sometimes |
4 |
8 |
| Often |
2 |
4 |
| Total |
50 |
100 |
| Eat the same food in the past month |
| Never |
42 |
84 |
| Rarely |
2 |
5 |
| Sometimes |
6 |
10 |
| Total |
50 |
100 |
| Eat Food you do not Preferred |
| Never |
42 |
84 |
| Rarely |
6 |
12 |
| Sometimes |
2 |
4 |
| Total |
50 |
100 |
| Eat Smaller meal than you preferred |
| Never |
35 |
70 |
| Rarely |
7 |
14 |
| Sometimes |
5 |
10 |
| Often |
3 |
6 |
| Total |
50 |
100 |
| Reduced meal in the last month |
| Never |
30 |
60 |
| Rarely |
13 |
26 |
| Sometimes |
5 |
10 |
| Often |
2 |
4 |
| Total |
50 |
100 |
| Have you ever gone to bed hungry in the past month? |
| Never |
43 |
86 |
| Rarely |
5 |
10 |
| Sometimes |
2 |
4 |
| Total |
50 |
100 |
| Was there no ever food in the house |
| Never |
36 |
72 |
| Rarely |
5 |
10 |
| Sometimes |
5 |
10 |
| Often |
4 |
8 |
| Total |
50 |
100 |
Table 2 Food Security.
Dietary diversity and anaemia prevalence
The diet of most respondents was found not to contain all the required nutrients. Four-star diet which is made up of staples, animal source foods, legumes and vitamin A rich fruits and vegetables and other fruits and vegetables. Intake of two (2) star diet was 9 (18), 3-star diet was 31 (62%) and those who indicated they took four-star diet were 10 (20%).
Anaemia prevalence was found to be high in the district. The prevalence of severe Anaemia (Hb<7g/dl) was 2% and that of moderate Anaemia (Hb<11g/dl) was 72%.
Anaemia prevention interventions
All pregnant women in this study indicated that they were allowed to take all foods they consume prior to becoming pregnant and they also mentioned that their religious affiliation had no influence on dietary intake during pregnancy. All (100%) of the respondents indicated that they took SP before health care providers. Table 3 below shows the usage of interventions for Anaemia and malaria control in pregnancy.
| Intervention Frequency Percentage (%) |
| LLIN Use |
| Yes |
49 |
98 |
| No |
1 |
2 |
| Total |
50 |
100 |
| SP Intake |
| Yes |
47 |
94 |
| No |
3 |
6 |
| Total |
50 |
100 |
| IFA Intake |
| Yes |
48 |
96 |
| No |
2 |
4 |
| Total |
50 |
100 |
| Source of SP |
| Public Hospital/CHPS/ |
|
|
| Health Centre/Clinic |
50 |
100 |
| Private pharmacy 0 |
0 |
0 |
| Total 50 |
50 |
100 |
| Took IFA in the past week |
| Yes |
47 |
94 |
| No |
3 |
6 |
| Total |
50 |
100 |
| Intake of dewormer |
| Yes |
39 |
78 |
| No |
11 |
22 |
| Total |
50 |
100 |
Table 3 Anaemia and malaria control interventions.
Discussion
Anaemia prevalence
This study revealed that the prevalence of Anaemia among pregnant women in this study was 74%, as compared to the 2014 GDHS which reported an Anaemia prevalence of 45% among pregnant women and 48% among young women aged 15 to 19 years [11]. This finding is closely related to the GDHS results and explains that teenagers are more likely to develop Anaemia during pregnancy because in this present study, 22% of the participants were teenagers aged less than 20 years old. It also exposes that there is a great deal of other health conditions among teenagers. The participants were also less educated because only 12% of the participants had secondary education or above and this shows that they were less educated and indicate their vulnerable to diseases and Anaemia. A similar study in Nigeria reported that the prevalence of Anaemia in pregnancy was 51% [4] which was similar to the findings of this study. But a study in Pakistan found that the prevalence of Anaemia was 18.1% [12] which was quite lower than the findings of this study.
Progress on reducing the incidence of anaemia has been made in some regions, while further improvements are still needed in others. At a global level, in all age and gender groups, anaemia is estimated to have decreased roughly seven percentage points between 1990 and 2010, from 40% to 33% [8]. During roughly the same period (1995 to 2011), anaemia was estimated to have decreased by 4–5 percentage points in the three highestrisk groups (children aged under 5 years, pregnant women, non-pregnant women of reproductive age) [7]. At a regional level, Africa (central and west, and east) and south Asia had the lowest mean haemoglobin concentrations, as well as the highest prevalence of anaemia among high-risk groups in both 1995 and 2011, despite significant improvements for children in the African regions (larger than in any other region) [8]. No improvement was seen among some groups with low haemoglobin levels and high prevalence of anaemia in 1995, including non-pregnant women in West Africa, central Asia, the Middle East and North Africa; and pregnant women in southern Africa and south Asia. Haemoglobin concentrations among children appear to have declined in southern Africa, while the largest improvements in women’s haemoglobin levels were seen in Central America and the Caribbean, east Africa, east and south-east Asia and Oceania. The global average of the prevalence of anaemia in women of reproductive age increased slightly between 2005 and 2016, although the increase was not statistically significant. It declined from 42% to 38% in Africa and from 25% to 22% in Latin America and the Caribbean, although this was offset by slight increases in all other regions [19].
Anaemia among older adults is less well documented, but it is known that the prevalence of anaemia among adults aged over 50 years rises with advancing age, particularly among men. Data from predominantly high- income countries estimate that 17% (ranging from 3% to 50%) of individuals aged over 65 years in the community have anaemia, with a significantly higher prevalence among older adults in nursing homes (47%) [5]. Data from lowincome and middle-income countries are limited, though WHO estimated that roughly 24% of older adults (over 60 years of age) globally had anaemia in 2005. In Uganda, 20% of adults aged over 50 years had anaemia (24% of men and 17% of women) [9]. Though the proportion of elderly individuals affected is lower than that seen among children or pregnant women, both the proportion and the number of older adults affected are rising worldwide. Lifetimes are also lengthening, indicating a potentially substantial burden in this population group in the future.
This study also revealed that there was food insecurity among the respondents which could have partly accounted for the high prevalence of Anaemia among pregnant women in the Wassa East District. These findings correspond to a study by Habib, et al. [12] where it was observed that food insecurity existed and contributed significant to the cause of Anaemia. This implies that in efforts at combating Anaemia food security should be factored into programming. The use of malaria prevention by LLINs use was found to be high. Also many pregnant women were dewormed.
Discussion
Summary, conclusions, and recommendations
Summary: This study revealed that the prevalence of anaemia was high (74%) among pregnant women in the Wassa East District. The proposition of respondents who were teenagers was found to be high (22%) and many of these teenagers were more anaemic compared to other age categories. The use of anaemia prevention interventions such as IFA supplementation and ITN use were also high.
Conclusions: This study presents findings on predisposing factors to Anaemia in the Wassa East District. The main factors contributing to Anaemia among this group of pregnant women were food insecurity and dietary practices. Also, the intake of iron and folic acid supplement was high but not 100 hundred. Knowledge of pregnant women on dietary sources of iron rich foods was found to be low.
Recommendations: In order to reduce Anaemia prevalence and improve delivery outcomes as well as the general wellbeing of pregnant women, the following interventions and recommendations have been suggested:
• Government through the Ministry of Food and Agriculture should subsidize prices of farm inputs and agrochemicals to boost food production and provide incentives for farmers and also to attract the youth into farming.
• The Ghana Health Service through the RCH, Nutrition and Health promotion unit should intensify education on benefits of intake of IFA, Iron rich foods and iron inhibitors to the general population.
• Local health services providers such as district health directorate should collaborate with non- governmental organizations (NGOs), Faith based organizations and community leadership and volunteers working in the area of health to sensitized communities in their jurisdictions.
Funding Details
None.
Acknowledgement
We are grateful for the contribution of Dr. Sutherland, Amarch and Najat P. Karim.
Disclosure Statement
The Authors report no conflict of interest.
40909
References
- Allen LH (2008) To what extent can food-based approaches improve micronutrient status? Asia Pac J Clin Nutr 17: 103-105
- André B, Canhão H, Espnes GA, Rodrigues AMF, Gregorio MJ, et al. (2017) Is there an association between food patterns and life satisfaction among Norway’s inhabitants ages 65 years and older? Appetite 110: 108–115
- Baig-Ansari N, Badruddin SH, Karmaliani R, Harris H, Jehan I, et al. (2008) Anemia prevalence and risk factors in pregnant women in an urban area of Pakistan. Food Nutr Bull 29: 132–139
- Bhadoria AS, Kapil U, Bansal R, Pandey RM, Pant B, et al. (2017) Universal health coverage - There is more to it than meets the eye. J Family Med Prim Care 6: 169-170
- Biggs JM, Morgan JA, Lardieri AB, Kishk OA (2017) Abuse and Misuse of Selected Dietary Supplements Among Adolescents: a Look at Poison Center Data. J Pediatr Pharmacol Ther 22: 385–393
- Clements SJ, Maijo M, Ivory K, Nicoletti C, Carding SR (2017) Age-Associated Decline in Dendritic Cell Function and the Impact of Mediterranean Diet Intervention in Elderly Subjects. Front Nutr 4: 65
- Dimaria-ghalili RA, Amella EJ (2012) Assessing Nutrition in Older Adults. Hartford Institute for Geriatric Nursing, New York.
- Engelheart S, Brummer R (2018) Assessment of nutritional status in the elderly: a proposed function- driven model. Food Nutr Res 1: 1-6.
- Feleke BE, Feleke TE (2018) Pregnant mothers are more anemic than lactating mothers, a comparative cross-sectional study, Bahir Dar, Ethiopia. BMC Hematology 18: 1-7
- Food MOF (2021) Household Food and Nutritional Security Assessment. Government of Ghana.
- Ghana Statistical Service, Ghana Health Service, ICF International (2014) Ghana Demographic and Health Survey 2014. Rockville, Maryland, USA
- Habib MA, Raynes-Greenow C, Soofi SB, Ali N, Nausheen S, et al. (2018) Prevalence and determinants of iron deficiency anemia among non-pregnant women of reproductive age in Pakistan. Asia Pac J Clin Nutr 27: 195-203
- Harris D, Haboubi N (2005) Malnutrition screening in the elderly population. J R Soc Med 98: 411–414
- Korenromp EL, Armstrong-Schellenberg JRM, Williams BG, Nahlen BL, Snow RW (2004) Impact of malaria control on childhood anaemia in Africa - A quantitative review. Trop Med Int Health 9: 1050–1065.
- Kwak-Kim JYH, Chung-Bang HS, Ng SC, Ntrivalas EI, Mangubat CP, et al. (2003) Increased T helper 1 cytokine responses by circulating T cells are present in women with recurrent pregnancy losses and in infertile women with multiple implantation failures after IVF. Hum Reprod 18: 767–773.
- United Nations Children's Fund (2011) Ghana Multiple Indicator Cluster Survey with an Enhanced Biomarker and Malaria Module. UNICEF, USA.
- Scholl TO, Reilly T (2018) Anemia, Iron and Pregnancy Outcome. J Nutr 130: 443–447.
- Smith JL, Brooker S (2010) Impact of hookworm infection and deworming on anaemia in non-pregnant populations: A systematic review: Systematic Review. Trop Med Int Health 15: 776–795.
- Steiner-Asiedu M, Pelenah SJM, Bediako-Amoa B, Danquah AO (2010) The Nutrition Situation of the Elderly in Ghana: A Case Study. Asian J Med Sci 2: 95-103.
- Dalton RL, Sowinski RJ, Grubic TJ, Collins PB, Coletta AM, et al. (2017) Hematological and Hemodynamic Responses to Acute and Short-Term Creatine Nitrate Supplementation. Nutrients 9: 1359
- UNICEF, UNAIDS, WHO, UNFPA (2003) HIV and infant feeding Guidelines for decision-makers. United Nations System Standing Committee on Nutrition.
- UNICEF, WHO (2009) Baby-friendly hospital initiative: revised, updated and expanded for integrated care. Section 1, Background and implementation. WHO, Geneva
- Unnikrishnan D, Annam R, Jacob A, Thyagarajan B, Farrugia P (2018) STEMI in a Young Male after Use of Synephrine-Containing Dietary Supplement. Case Rep Cardiol 2018: 7074104.
- WHO (2009) Weekly iron-folic acid supplementation (Wifs) in women of reproductive age: Its role in promoting optimal maternal and child health. WHO, Geneva.
- WHO (2011) Guideline: Use of multiple micronutrient powders for home fortification of foods consumed by infants and children 6–23 months of age. WHO, Geneva.
- World Health Organization (2011) The Global Prevalence of Anaemia in 2011. WHO, Geneva.
- World Health Organization (2011b) Use of multiple micronutrient powders for home fortification of foods consumed by pregnant women. WHO, Geneva.
- World Health Organization (2017) Nutritional Anaemias: Tools for Effective Prevention. WHO, Geneva.
- World Health Organization (2012) Guideline: Daily iron and folic acid supplementation in pregnant women. WHO, Geneva.

