Keywords
Inter personal physical Violence; Trauma; South Ari district
Introduction
Background
Interpersonal physical violence is the intentional use of physical force or power, threatened or actual, against another person that either results in or has a high likelihood of resulting in injury, death, psychological harm, mal-development or deprivation [1]. It is the part of our day to day life coincidences that parallels the history of the evolution of human being, with his aggressive instincts, and endless ambition to dominate others or deserve privilege and safeguard his territory and properties without regard to the price he must pay to achieve these goals. Globally, studies indicate that the problem of interpersonal violence related-injuries is recognized as the leading causes of emergency visits to health facilities and is a significant contributor to surgical morbidity and mortality [2]. Interpersonal violence results in long-term disability where people with even a minor injury can remain disabled for at least one year after the incident [2]. Beyond physical injuries, the health effects of violence are lifelong health and social problems including disabilities, depression, reproductive and physical health problems, smoking, alcohol and drug misuse, and high-risk sexual behaviors [2,3]. Violence also erodes the economic fabric of communities as local economies are impacted by workforce absenteeism, lost productivity, loss of human capital, and face disincentives for investment and economic development [4].
The possible causes (triggering factors) of interpersonal violence are widespread poverty, unemployment, income inequality among citizens, patriarchal system, risk-taking, defense of honor, weak parenting, access to firearms, widespread alcohol misuse, and a weakness of the government and leadership in the mechanisms of tracking assailants. This occurs despite; advances in development of services for victims of violence, innovation from non-governmental organizations, and evidence from research [5]. World Health Organization (WHO), United Nation Office on Drugs and Crime (UNODC) and United Nation Development Program (UNDP) conducted a study on the Global Status Report on Violence Prevention (GSRVP 2014), highlights data from 133 countries, covering 6.1 billion people and representing 88% of the world’s population [4,6,7]. According to this report, the health and social consequences of violence take an economic toll on countries, although the precise burden is unknown, particularly in developing countries where economic losses and impact tend to be underestimated. The provision of treatment, mental health services, emergency care and criminal justice responses are some of the direct costs associated with violence. There are also a wide range of indirect costs. Victims of violence are more likely to experience spells of unemployment, absenteeism, and to suffer health problems that affect job performance. Other indirect costs include those related to lost productivity because of premature death; long-term disability; the provision of places of safety for children and women; disruptions to daily life because of fears for personal safety; and disincentives to investment and tourism [3,4,6,7]. Therefore; as a conclusion, violence is a significant public health problem in its own right, and a major risk factor for lifelong ill health and other social problems that in combination can lead to substantial economic costs [3,4,6,7].
Statement of the problem
Interpersonal physical violence related injury has an important negative impact on individual’s daily life and economic status of every country. The problem has still neglected worldwide and became the leading cause of injury at emergency visit particularly in Africa [3,4,6]. Globally, the magnitude of intentional interpersonal physical violence related injury is about 30%. The burden of this problem is high in low and middle income countries covering 14% and 27% respectively. Women (42%), children (22.6%) and elderly people (6%) bear the highest burden of the non-fatal consequences of physical violence [4,6]. According to the trend analysis report on conflict related injury over the period 2000–2012, death rates were estimated to have declined by just over 16% globally (from 8.0 to 6.7 per 100,000 population), and in high-income countries, by 39% (from 6.2 to 3.8 per 100,000 population) [3,4]. By contrast, in low- and middle income countries have shown fewer declines over the same period. For both upper and middle-income countries, the decline was 13%, and for lowincome countries it was 10%. Nevertheless, deaths are only a fraction of the health and social burden arising from violence [3,4,6]. Though national level scientific studies on the magnitude of interpersonal physical violence in Ethiopia is limited, reports from health care financing and health service delivery system indicated higher magnitude of the problem. According to the study conducted at North Gondar Administrative zone, Ethiopia, a total of 386 patients visited the Hospital during the study period (2014) with a main complaint of interpersonal conflict [8]. Similar studies in Addis Ababa, Ethiopia, on injuries related to interpersonal violence found that interpersonal conflict was the most common cause of injury after road traffic injuries [9]. In South Ari district, even though no previous scientific study was conducted on the interpersonal violence, HMIS reports indicated that throughout 2009 EFY, there were a total of 3,502(12.26%) trauma cases who visited the emergency department of the nine health centers of the district. Intentional interpersonal physical violence parts 393(11.2%) of all trauma cases, resulted from different predisposing factors.
To tackle this public health important problem, multi-dimensional collaboration and effort is obligatory, and every country including Ethiopia has incorporated to their surveillance and diseases reporting system [4,6]. But still low focus of health organizations along with the poor reporting system as compared with other public health problems resulted that the true estimate for prevalence of injury due to interpersonal conflict remains masked in middle and low income countries [4,6].
Therefore the aim of this study was assess the magnitude and predisposing factors for intentional interpersonal physical violence injury in South Ari district, South Omo zone, Southern Ethiopia.
Rationale of the study, in many developing countries including Ethiopia, injury due to interpersonal conflicts is a common public health problem. Although this injury is preventable, still it continues to be the widespread health problem globally. In Ethiopia, despite multi-dimensional collaboration efforts have done to reduce conflict related injury; it is increasing at an alarming rate and constitutes the major cause of emergency department visits of the health facilities. On the other hand, paucity of sufficient data about its magnitude leads to underestimation of the injury burden. Without reliable information, health care planners at all levels are unable to allocate resources so as to achieve the greatest impact in preventing injuries, treating and rehabilitating injured persons. Similarly, in South Ari district there is lack of clear data on interpersonal physical violence related injury both in its magnitude and possible triggering factors. Therefore; any comprehensive violence prevention strategy must identify ways to mitigate or buffer against these triggering factors. This can be done by conducting scientific study that contribute scientific presentations on the magnitude of injury and its associated factors in order to construct resource planning and prevention modalities that can help the policy makers in designing effective prevention strategies. So findings of this study conducted on the magnitude and predisposing factors of intentional interpersonal physical violence injury are going to contribute a lot at South Ari district to take any possible preventive measures. In an Indian study, in 2013 conducted to analyze injury characteristics, 813 victims of interpersonal violence presented to emergency department at a government medical college and hospital from a major city in Central India. Of these victims 74% were male and 26% were female. The majority of male victims reported having been physically assaulted by unknown male while most of the females were victims of spousal assault. On the other hand, 28.5% of cases were females who were subjected to violent assaults by strangers. Of these Indian males, financial disputes, robbery, and conflicts with police were the most common predisposing factors for those male victims. The same study revealed that blunt trauma was more prevalent both in male and female victims. Firearms and heavy cutting weapons were rarely used. The head, neck, and face region was the most commonly injured anatomical site both in male (37%) and female (55.4%) victims. A history of alcohol consumption and objective smell of alcohol were found positive in 54.61% of victims in this study [10,11]. The research has also indicated that some socioeconomic characteristics of women have a significant correlation with an increased risk of domestic violence. These characteristics include: Living in urban area, advanced age, low levels of education and lower family income [12].
In America in the year 2000, more than 2.5 million injuries were related to interpersonal violence and self-injury, resulting in a loss of $70 billion. Almost $5.6billion was spent on medical care for these violence related injuries and $64.7 billion was lost due to decreased work and family productivity. Violence was recognized as a leading cause of mortality and morbidity in the United States It has resulted in approximately 50,000 deaths and 2.2 million injuries annually that require medical attention [13,14]. In Tanzania a study on interpersonal injuries was conducted in Dodoma in 2011, spouse’s conflict injuries represented 20% of all injuries. The age group ranged from 18–36 years old was the most injured followed by victims with an age in between 36-54 year old. For male victims the injuries mostly occurred outside their home (72%), comparatively, female victims were just as likely to be injured inside or outside their homes (50%).The study revealed that single people were mostly injured during day, whereas married and cohabitating people were most often injured at night. Eighty percent of men were injured while they were attempting to steal, while statistically the main cause for females stemmed from sexual violence [15]. The instruments used to cause harm to the victims were knives and machetes in 42% of cases followed by wooden sticks in 26% of incidences. Seventy- nine percent of all injuries occurred on the head and neck followed by chest and abdomen with 19%.
In a prospective study of all trauma admissions for one year at Groote Schuur Hospital in Cape Town, South Africa, the most common mechanisms of injury due to assaults was with a sharp object (20.9%) or blunt object (17%), road traffic accidents (18.8%), and falls (18.4%). Firearm caused 4.8%of injuries. Male had higher percentages of injury caused by violent crimes. Injury with sharp objects, blunt objects (physical beating) and injury by firearms covered 34.4%, 12.5%, 8.1% of cases respectively. Most intentional violent crimes occurred because of interpersonal disputes (71.6%), assault within the community (10.1%), and gang related violence (8.3%) [11,16].
According to the study conducted at North Gondar Administrative zone, Ethiopia, a total of 386 patients visited the Hospital during the study period (2014) with a main complaint of interpersonal conflict. Of these 352 (91.2%) were male and 34(8.8%) female, giving a male to female ratio of 10:1. The age group of 21- 40 accounted for 61.8% of the victims. The great majority 354 (92.0 %) were living in rural area and only 32 (8.0 %) from urban. The commonest occupation were farmers 290 (75.1%) followed by 41 (10.6%) students and 26 (6.7%) house wives. Among the victims almost half had formal education and half never go to school, 48.0% and 47.0% respectively. Of the injured patients, 295 (76.0%) were responsible for household with a mean family member of five. The victim offender relationship were neighbors in 216 (56.0%), 54 (14.0%) family members and 21(5.4%) friends and 95 (24.6%) others. The finding revealed that the commonest motives of the conflict were land dispute 123 (31.9%) but 70(18.1%) were not willing to tell their reason. The interpersonal conflicts were mainly occurred on the street/village 156 (40.4%), followed by (19.4%) in farm [8].
At the time of the conflict at least one of the victims was drank alcohol (in 49.2%). The instruments used to fight were blunt object like stick in 332 (86.0%), 36 (9.3%) sharp objects and 18 (4.7%) gunshots. The main reason of visiting the hospital were seek medical care in 209 (54.1%), 127 (32.9%) for certificate and 50 (13.0%) to have x ray examination [8]. Similar study on interpersonal injuries conducted in Gondar, revealed land conflict to be the predominant cause at 31.9%. The most common locations of injury in the road 40.4% and home 33.4%, The most common type of injury was fractures at 66,6%, of which 86 percent of fractures were caused by a stick; The offenders were neighbors in 56% of cases and friends in 24,6%. Furthermore, 49.2% of victims were drinking alcohol. The main reasons for consulting the hospital were medical care 54.1%, 32% for medical certificate and for 13% of cases for imaging especially x-rays. 66% of victims were managed as our patients, while 32.6% were admitted, and 0.8% was referred to another medical facility [8]. It is estimated that in the year 2000, 520,000 people around the world died from intentional injuries and 95% occurred in low and middle income countries [1,2].Similar studies in Addis Ababa, Ethiopia, on injuries related to interpersonal violence found that interpersonal conflict was the most common cause of injury after road traffic injuries [9] (Figure 1).
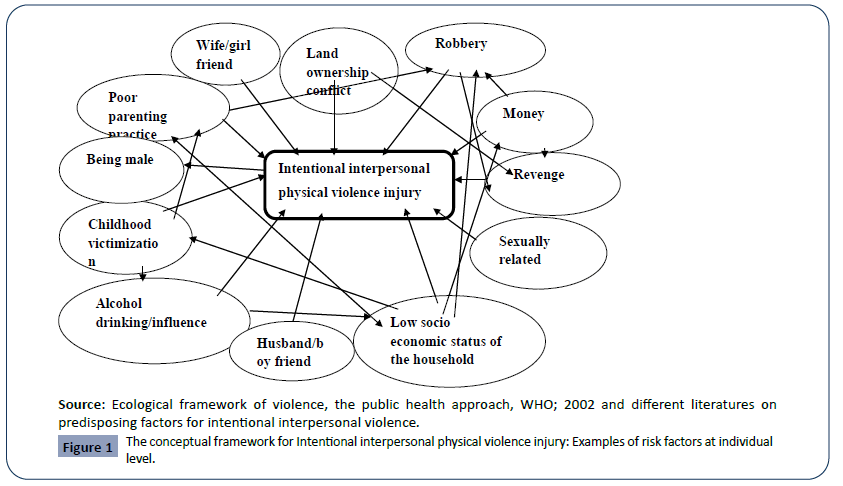
Figure 1: The conceptual framework for Intentional interpersonal physical violence injury: Examples of risk factors at individual level.
Description of individual level factors for IIPPV related injury
Violence related behavior is strongly associated with both relationship and individual level factors such as gender, age, poor parenting practice, marital discord, violent parental conflict, low socio-economic household status, friends that engaged in violence. Being a victim of childhood maltreatment, psychologically/personally disordered, Alcohol/substance abuse and previous exposure to violent act are other known factors to develop violent personal behavior [4,17,18].
Gender/sex: Males are more at risk of experiencing violence and correspondingly drug related violence [4,17]. For example, a study of heroin users in Scotland found that males were significantly more likely to have been victims and perpetrators of assault than women [17]. However, women who have been abused and/or neglected in childhood may be at greater risk than males of subsequently developing drug use and dependence and being arrested for both violent and non-violent crimes [17]. In a Norwegian study, female hard drug users admitted to treatment had experienced more childhood emotional and sexual abuse and neglect than males [17].
Age: Age is a risk factor for both violence perpetration and victimization [17,18]. Young people (age from10 to 29 years; according to WHO age classification) are at a higher risk of substance related interpersonal violence; particularly intimate partner and gang-related violence [1,4].
A history of childhood victimization: A history of abuse and/or witnessing violence in childhood increases the risk of subsequent use of substances like alcohols, khat and others. At the same time it increases the risk of being a victim of violence, particularly intimate partner violence, in later life [17].
Alcohol drinking: individuals who start drinking alcohol at an early age are more likely to develop alcohol problems in adolescence and adulthood. This results in drinking more frequently and in greater quantities than those who delay drinking and are more likely to drink and to get drunk. Vulnerability to alcohol misuse in later adolescence appears to be greatest among those who begin drinking before age 13years. It ends up with increased health risks, including alcohol-related injuries, involvement in violence, and suicidal thoughts and attempts. Family standards and rules, parental monitoring, and close family relationships are important in delaying alcohol initiation in early adolescence [18].
Low socio economic status due to spending money: Alcohol consumption by young people and/or family members or friends, including heavy and regular drinking, increases as the amount of spending money young people and the household have available to them increases. This is associated with low socio-economic status of the family or individuals predisposing directly for violent activities or robbery and ganging [18].
Land conflicts: The relationship between land and conflict often changes over time. Land issues readily lend themselves to conflict. Land is an important economic asset and source of livelihoods; it is also closely linked to community identity, history and culture. Communities, therefore, can readily mobilize around land issues, making land a central object of conflict. Tensions over land may also be closely related to, or manipulated by, political interests [18].
Parenting approaches: Young people who are poorly monitored by their parents and care givers begin drinking alcohol at an earlier age, tend to drink more, and are more likely to develop problematic patterns of drinking. Parental monitoring like, family standards and rules and close family relationships are important in delaying alcohol initiation in early adolescence. Harsh parenting, family conflict and a permissive approach to alcohol by parents are associated with risky drinking in adolescence and become violent [18].
Methods and Materials of the Study
Study setting
South Ari district is one of the eight districts of South Omo zone with a total of 50 administrative kebeles, of which 46 are rural. The district has nine health centers and 46 health posts. The total population estimate for the year 2017/2018 is 247,952, covers approximately 32% of the zone’s population and the most populous district from the zone. The capital of South Ari district, Gazer is located 542kms to the south from the capital of Southern Nation Nationalities and People region (SNNPR) ‘Hawassa,’ and 17kms from South Omo zone capital, Jinka [19].
The district covers 152,062.48km2 total surface area and bordered by Basketo Special District and North-Ari district to the North, Benatsemay district to the South, Malle district and Uba Debretsehay of Gamogofa zone to the East and Salamago district to the West. The district is divided into three principal agroecological zones. About 60% of the climatic condition is Dega followed by 28% Kola and 12% Woynadega with altitude above sea level reaches 526-1645 meters with mean annual rainfall ranges 800-1600 ml3 (cube-ml) and monthly mean temperature scores about 210C [19]. Agriculture is the main income source for the population and the community has been cultivating lands for their annual harvesting of crops from July through January. Local or traditional drink preparations (like Cheka, Areki, Local-beer, Borde, Tej) are common. Especially Cheka has been used as food and a common drink in the community [20].
Sample size determination
The sample size was calculated using Epi-info-Stat Cal- based on the following assumptions. Assumptions for the magnitude/ prevalence of intentional interpersonal physical violence related injury was 37.4% [21] with 95% level of confidence and 5% margin of error. Then thecalculatedsamplesizewas360 and by adding 10% of the calculated sample size for non-response rate, the final sample size was 396 (for the first objective).
Assumptions to the risk factor: percent outcome to non-exposed groups to violence or violence related behavior is 39.5%, percent outcome to exposed group to violence or violence related behavior 64.5%, ratio of unexposed to exposed group for violence or violence related behavior is 4:1 [21]. By taking 95% confidence interval and 80% power for the study, the sample size was 215 and by adding 10% for non-responders, the final sample size was 237(for the second objective). However, the sample size calculated for the second objective (n=237) is smaller than the sample size for the first objective (n=396). Therefore, the final sample size for the project was the larger one, i.e. 396 (Table 1).
Table 1. Shows that sample size determination for the study at South Ari district; 2018.
| Objectives |
Power (%) |
C.I (%). |
Ratio |
Prevalence (%) |
Sample size |
Non- response rate (10%) |
Final sample size |
References |
| Objective-1 |
Prevalence |
80 |
95 |
|
37.4 |
360 |
36 |
396 |
[21] |
Objective-2:
Predisposing factors |
Previous exposure to violence |
80 |
95 |
4:1 |
64.5 |
215 |
22 |
237 |
[21] |
| Alcohol use |
80 |
95 |
1:1 |
70.0 |
278 |
28 |
306 |
[29] |
| Male sex |
80 |
95 |
1:1 |
64.0 |
140 |
14 |
154 |
[29] |
Sampling procedure
First, all of the nine functional health centers of South Ari district were included in this study after getting the list from the district’s health office. Then, a total number of intentional interpersonal violence injured cases who visited the emergency department of each health center in the past three months was obtained from the registration book of emergency departments. The number of victims of injury in each HCs, in the past three months, were as follow: 42 in Bethimal health center, 87 in Gazer health center, 79 in Metser health center, 76 in Tembel health center, 29 in Tolta health center, 31 in Berka health center, 33 in Senegal health center, 29 in Shengama Billi health center, and 112 in Wubhamer health center. Thus, we expected a total of 518 victims of injury who visited the emergency department of all health centers in the past three months in the district. Next to that, based on our expectation, we allocated our sample-size (n=396) to each health centers using proportional sampling methods (Shown in Figure 2 below).Then, all individuals with trauma who visited to the emergency department of all the nine health centers at South Ari district from January 10/2018 through April15/2018were interviewed face-to-face till the desired number achieved. In the case of children and cases who couldn’t conduct interview, data were collected by interviewing care givers and surrogates respectively, provided that they should be witness of the incident (Figure 2).
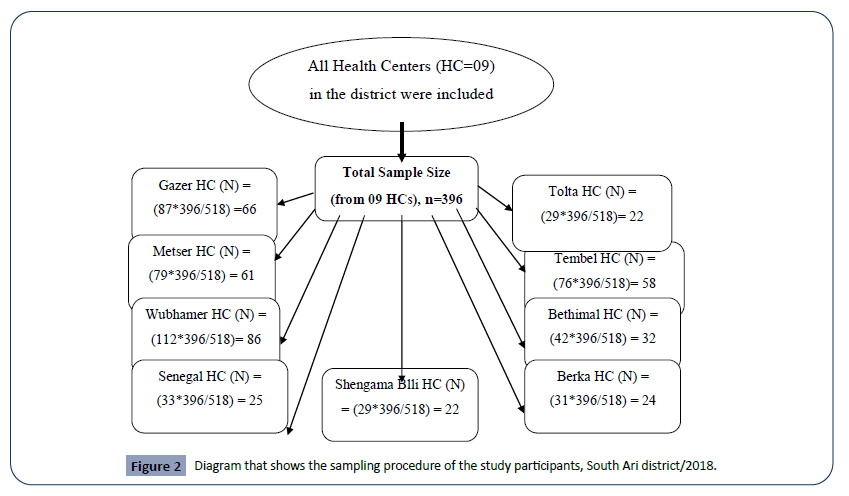
Figure 2: Diagram that shows the sampling procedure of the study participants, South Ari district/2018.
Data collection tools and procedures
Structured questionnaire on variables for intentional interpersonal physical violence injury and predisposing factors was adapted from different literatures [1,2,4,8,22,23] and modified contextually to the study area for interview. The questionnaire was initially prepared in English and translated to Amharic language (majority of the population at the district speak Amharic language) to the data collectors who were native health workers that have been worked at the health centers of the district; then clear description was given to them about how to collect the data if there would be a case that can’t speech Amharic completely. Finally, it was translated back to English language to check its consistency. The questionnaire had four parts: The first part was about socio-demographic factors that encompass; age, occupation, educational status, family size, and residence. The second part was about the comprehensive knowledge of the respondents about the problem and its predisposing factors. The third part was about the potential predisposing factors of interpersonal violence and the last part deals the status of injury. Eight diploma holder nurses and two degree holders in public health were participated in the data collection procedure.
Data quality assurance
Before the data collection activity, three days orientation was given to eight data collectors and two supervisors focusing on the objective of the study, contents of the questionnaire and value of collecting actual clear data and how to interview with local language Arigna by using the Amharic questions. The questionnaire was discussed by going through every part and clarification was provided to data collectors. It was then pre-tested on 5% of the sample in areas other than the study catchment health centers. The questionnaire was then assessed for its simplicity to fill and clarity. Questions that were difficult to ask were rephrased based on the finding from the pre-test. Throughout the data collection activity, all filled questionnaires were checked by supervisors immediately after collected for accuracy, clarity and consistency and necessary corrections was made if it exists before the victim leave the health center. Data were entered into Epi Version 7; exported to and analyzed using the Statistical Package for Social Sciences (SPSS) version 20.0. Completeness and consistency of variables during data entry and analysis were checked using frequency distributions and cross-tabulations. Bivariate analysis between dependent and independent variables was performed using binary logistic regression. The strength of association between dependent variable and independent variables was expressed in odds ratio (OR) through 95% confidence interval (CI). Variables which have association in bivariate analysis (p-value <0.25) were included in multivariate analysis. Finally, multivariate analysis was done to evaluate the independent effect of each candidate variable on experiencing intentional interpersonal physical violence injury by controlling the effect of other variables. A statistical significance was determined through 95% C.I. for each independent variable or using a p-value < 0.05 as a cutoff point.
Ethical considerations
All participation in the study was voluntary and it wouldn’t be involve any risk to the participants in terms of management nor compulsive approaches to give response. The participants were free to leave the study at any time. This study was approved by IRB-CMHS, Hawasa University, ethics and research committees. Permission letter was obtained from South Omo zone health department and South Ari district health office, and because of majority of study subjects was illiterate, informed consent was obtained after clearly explaining the purpose of the study and data confidentiality after read to them the consent form by persons other than the data collectors. Before informed/verbal consent was obtained, the respondents were told that they have the right to be involved or not in the study. For those who were not mentally alert; a family member was requested to consent in accordance with the laws of Ethiopia. The study subjects were assured that no trouble about confidentiality and all the data collected from them are going to be handled with utmost confidentiality, and only used for the purpose of this study.
Results
Socio demographic characteristics of study participants
All participants of this study gave a complete responses (n=396). Findings showed that males out-numbered females by a sex ratio of 1.34, as males counted to 227 (57.3 %). Most victims that visited to the emergency department of the health centers have age between 23 and 45 years (42.4%) with the overall mean age of respondents was 30.1years (with a SD ± 12.8 years). Regarding the marital status, 243 (61.4%) of the participants were married and cohabited with their partners. The data about the educational level of the study subjects’ showed that 237 (59.8 %) have no formal education and 57 (14.4%) have attended secondary school education and above. Among the 396 victims, majority of the respondents, i.e. 139 (35.1 %) have average monthly income less than or equal to 1000 Ethiopian birr but only 9 (2.3%) of the respondents have income greater than 4000 Ethiopian birr. Regarding the occupational status of trauma victims, the findings of this study revealed farmers were the most affected population groups (60.8%) and students (25.4%) took the second rank (See the characteristics of respondents on Table 2 below).
Table 2. Socio-demographic characteristics of the study participants visiting the selected health centers’ emergency departments (EDs) of South Ari district, 2018; (n = 396).
| Variables |
Category |
Frequency(n=396) |
Percent (%) |
| Sex |
Female |
169 |
42.7 |
| Male |
227 |
57.3 |
| Total |
396 |
100 |
| Age in years |
≤4 |
9 |
2.3 |
| May-14 |
27 |
6.8 |
| 15-19 |
45 |
11.4 |
| 20-24 |
91 |
23 |
| 25-44 |
168 |
42.4 |
| ≥45 |
56 |
14.1 |
| Total |
396 |
100 |
| Marital status |
Married/cohabited |
243 |
61.4 |
| Single/widowed |
50 |
12.6 |
| Others |
103 |
26 |
| Total |
396 |
100 |
| Educational level |
Illiterate |
237 |
59.8 |
| Preschool children |
15 |
3.8 |
| Primary education |
87 |
22 |
| Secondary and above |
57 |
14.4 |
| Total |
396 |
100 |
| Average monthly income in ETB |
< 1000 |
139 |
35.1 |
| 1001-2000 |
89 |
22.5 |
| 2001-3000 |
109 |
27.5 |
| 3001-4000 |
50 |
12.6 |
| > 4001 |
9 |
2.3 |
| Total |
396 |
100 |
| Occupation |
Farmer |
241 |
60.8 |
| Student |
100 |
25.4 |
| Merchant |
39 |
9.8 |
| Others |
16 |
4 |
| Total |
396 |
100 |
Prevalence of intentional interpersonal physical violence related injury
The magnitude of intentional interpersonal physical violence injury in this study was found to be 167(42.2%). Regarding the mechanism of injury the study showed that unintentional injuries were the primary cause for emergency department visit accounted 207 (52.3 %) of all injured cases. Self-inflicted injuries after quarreled with other persons 12(3%) and fight between siblings/children 12(3%) were the other mechanisms of injury for this study.
In this study, emergency department visits cases with injury due to intentional interpersonal physical violence was high in Gazer and Tolta health centers scoring 60.6% and 59.1% respectively. The least magnitude of this problem was scored at Senegal health center (12.0%) as shown on Figure 3 below. Majority (59.0%) of victims sustained the injury during day time and the remaining proportion of victims assaulted during night.
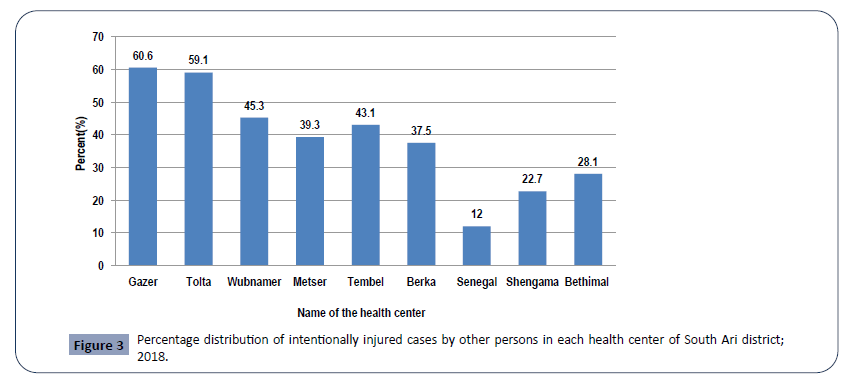
Figure 3: Percentage distribution of intentionally injured cases by other persons in each health center of South Ari district; 2018./p>
In this study as shown on Table 3 below, male were more suffered from intentional interpersonal conflict injury (57%) as compared with females (43%). The highest burden of conflict related injury (63.5%) was occurred among married/cohabited individuals and the least score occurred among singles/widows. Regarding educational level, around 61.7% of victims were illiterate and only 3.0% of victims were pre-school children. Data on occupation of the cases in this study indicated that, farmers were the most affected with proportion of 66.5%.
Table 3. Socio-demographic characteristics of victims from intentional interpersonal physical violence visiting the selected health centers’ emergency departments (EDs) of South Ari district, 2018; (n =167).
| Variables |
Category |
Frequency(n=167) |
Percent (%) |
| Sex |
Female |
71 |
43 |
| Male |
96 |
57 |
| Total |
167 |
100 |
| Married/cohabited |
106 |
63.5 |
| Marital status |
Single/widowed |
16 |
9.6 |
| Others |
45 |
26.9 |
| Total |
167 |
100 |
| Educational level |
Illiterate |
103 |
61.7 |
| Preschool children |
5 |
3 |
| Primary education |
37 |
22.2 |
| Secondary and higher education |
22 |
13.1 |
| Total |
167 |
100 |
| Occupation |
Farmer |
111 |
66.5 |
| Student |
33 |
19.7 |
| Merchant |
16 |
9.6 |
| Others |
7 |
4.2 |
| Total |
167 |
100 |
In this study, the average monthly income distribution of victims from intentional interpersonal conflict injury has different patterns as shown in Figure 4 below. Around 42.0% of victims have average monthly income below 1001 Ethiopian birr and only 6.4% of cases have average monthly income above 3001 Ethiopian birr.
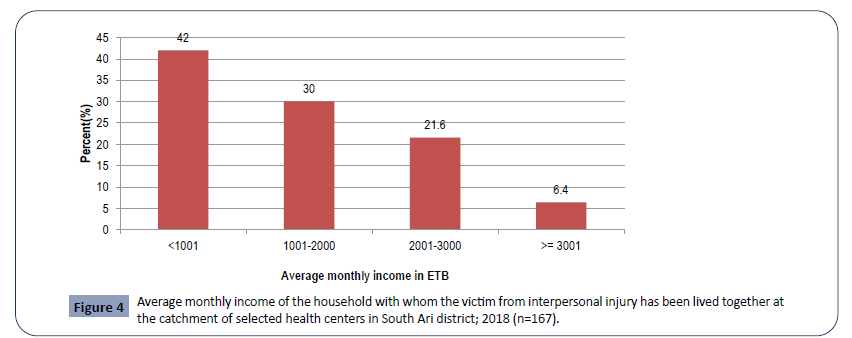
Figure 4: Average monthly income of the household with whom the victim from interpersonal injury has been lived together at the catchment of selected health centers in South Ari district; 2018 (n=167).
The result of this study shows that the higher proportion of victims due to intentional interpersonal physical violence related injury have the age between 25 and 44 years (54.5%) but the frequency of individuals with this type of injury was lower in age categories below 5 years (2.3%) and above 44 years (see Figure 5).
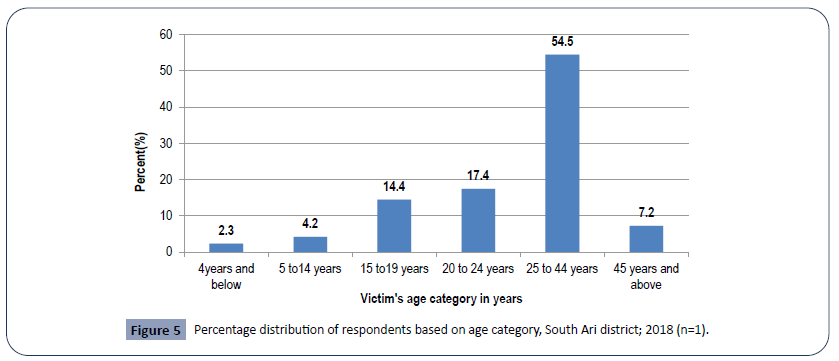
Figure 5: Percentage distribution of respondents based on age category, South Ari district; 2018 (n=1).
In the current study, around 59.8% of individuals with assault related physical injury didn’t know the predisposing factors of IIPPV related injury and only 9.0% responded as land ownership competitions are the reasons for the problem. Disability (29.3%), death (25.1%) and Death and disability (21.0%) were the top three potential outcomes of this IIPPV related injury as explained by the victims. Around 42.0% of the responders replied that the primary responsible body to prevent this problem is police and the role of every individual of the community was only 6.6% (See Table 4).
Table 4. Percentage distribution of respondents by selected variables related to general knowledge about IIPVI, South Ari district; 2018 (n=167).
| Knowledge related Variables |
Category |
Frequency |
Percent |
| (n=167) |
(%) |
| Predisposing factors of IIPV |
Land ownership |
15 |
9 |
| Alcohol influence/substance abused |
35 |
21 |
| Others |
17 |
10.2 |
| I don’t know |
100 |
59.8 |
| Total |
167 |
100 |
| Potential outcomes of assault |
Death |
42 |
25.1 |
| Disability |
49 |
29.3 |
| Death and disability |
35 |
21 |
| Economic deficit |
27 |
16.2 |
| I don’t know |
14 |
8.4 |
| Total |
167 |
100 |
| Responsible body for prevention |
Not preventable |
33 |
19.7 |
| Police |
70 |
42 |
| Political leaders |
53 |
31.7 |
| Every individual of the community |
11 |
6.6 |
| Total |
167 |
100 |
| Risk population groups |
Children |
9 |
5.4 |
| Adults and adolescents |
39 |
23.3 |
| Any age group of both male and females |
75 |
44.9 |
| I don’t know |
44 |
26.4 |
| Total |
167 |
100 |
According to the current study findings, majority (25.6%) of cases were assaulted by their family members. About 22.8% of cases sustained conflict related trauma by unknown assailants and conflict between friends contributed 20.4% of all trauma cases from IIPPV (See Figure 6 below).
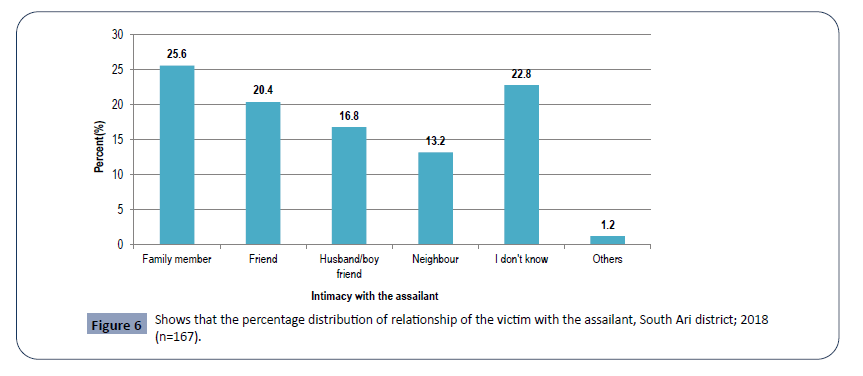
Figure 6: Shows that the percentage distribution of relationship of the victim with the assailant, South Ari district; 2018 (n=167).
The most affected area of the body was head and neck region parted 67(40.1%) of all crime victims and the list was head and trunk region (3.0%) (See Figure 7 below). Concerning the type of injury resulted from intentional interpersonal physical violence, 67(40.0%) of victims were suffered from blunt injury and about 39.0% sustained penetrating type of injury (See Figure 8). The violence act resulted fracture was only in 5(3 %) of patients and referred to the nearby hospital for further management. There was no any death report due to intentional physical violence during the study period (See Figure 8) and 71(40.0%) were committed by stick and the list proportion of victims (5.4%) were injured by Machete (See Table 5).
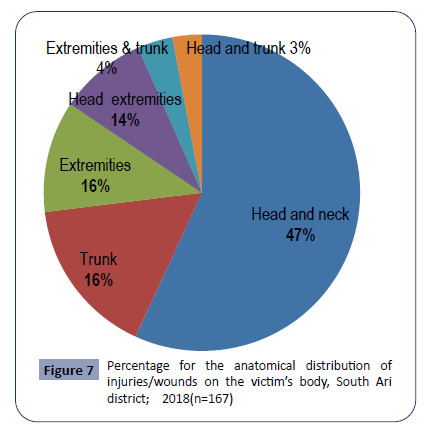
Figure 7: Percentage for the anatomical distribution of injuries/wounds on the victim’s body, South Ari district; 2018(n=167)
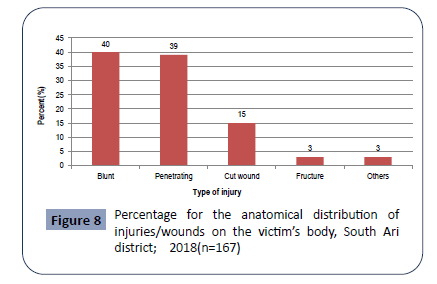
Figure 8: Percentage for the anatomical distribution of injuries/wounds on the victim’s body, South Ari district; 2018(n=167)
Table 5. Type of weapon used by the assailant during the crime incidence, South Ari district; 2018 (n=167).
| Type of weapon used by the assailant |
Frequency (n=167) |
Percent (%) |
| Axe |
13 |
7.8 |
| Stone |
34 |
20.4 |
| Machete |
9 |
5.4 |
| Stick |
63 |
37.7 |
| Knife/Stab |
15 |
9 |
| Punch |
33 |
19.7 |
| Total |
167 |
100 |
According to findings in this study, the highest proportion of victims sustained intentional interpersonal violence related injury at home (37.0%) followed by at road (30.0%).Only 1.8% of cases assaulted at schools.
Associated factors for intentional interpersonal physical violence injury
In the bivariate analysis, land ownership conflict, low socioeconomic status of the household, neglected parenting practice, revenge/indemnity and alcohol influence were found to be significantly associated with interpersonal physical violence injury with 95%CI and P-value ≤ 0.25 (See Table 6).
Table 6. Distribution of the assault regarding to the place where it was happened, South Ari district; 2018 (n=167).
| Place of the incident |
Frequency (n=167) |
Percent (%) |
| Home |
62 |
37.0 |
| Road |
50 |
30.0 |
| Farm |
21 |
12.6 |
| Hotel/Grocery |
22 |
13.2 |
| School |
3 |
1.8 |
| Market |
9 |
5.4 |
| Total |
167 |
100 |
However after multi-variable analysis in multiple logistic regression analysis of this individual factors (See Table 7), only land ownership conflict, low socio-economic status of the household, neglected parenting practice and alcohol influence were found to be significantly associated with interpersonal physical violence injury with 95% CI and P-value ≤ 0.05. Land ownership conflict are significantly associated with interpersonal conflict related injuries (AOR=2.18; 95% CI, 1.32-3.58) as land is the main source of income/assets to the majority of the district’s community and protecting it from invasion is mandatory. Similarly, low socioeconomic status was the reason for ED visits of victims at the health centers of the district (AOR=1.73; 95% CI, 1.08-2.92) as it persuade individuals to spend their time to gather daily income in harsh behaviors like robbery and gangster. Neglected parenting practice (AOR=7.97; 95% CI, 4.77-13.34) and alcohol influence (AOR=3.39; 95% CI, 2.05-5.61) also significantly associated with intentional interpersonal physical violence related injury as they predispose to unwanted places that favored to date and experience violence related behaviors.
Table 7. Bivariate and multivariate analysis output on predisposing factors for intentional interpersonal physical violence injury, South Ari district; 2018 (n=167).
| |
Intentional injury by others: No (%) |
|
|
| Predisposing factors for IIPPVI |
Yes (N=167) |
No (N=229) |
Bivariate analysis COR(CI) |
Multivariate analysis AOR(CI) |
| Low socio-economic status** |
Yes |
89 (53.3%) |
81 (35.4) |
1.78 (1.08-2.92)* |
1.73 (1.08 2.92)@ |
| |
No |
78 (46.7%) |
148 (64.6) |
|
|
| Land ownership conflict |
Yes |
112 (67.1%) |
107 (46.7) |
2.29 (1.37-3.82)* |
2.18(1.32-3.58)@ |
| |
No |
55 (32.9%) |
122 (53.3) |
|
|
| Alcohol influence |
Yes |
127(74.0%) |
98 (42.8) |
3.27 (1.96-5.46)* |
3.39(2.05-5.61)@ |
| |
No |
40 (26.0%) |
131 (57.2) |
|
|
| Childhood victimization |
Yes |
34 (20.4%) |
56 (24.5) |
0.87 (0.47-1.60) |
|
| |
No |
133 (79.6%) |
173 (75.5) |
|
|
| Revenge/indemnity |
Yes |
22(13.2%) |
22 (9.6) |
1.85 (0.85-4.03)* |
1.93(0.90-4.15) |
| |
No |
145 (86.8%) |
207(90.4) |
|
|
| Neglected parenting practice |
Yes |
102 (61.1%) |
34 (14.8) |
8.06 (4.75-13.69)* |
7.97(4.77-13.34)@ |
| |
No |
65 (39.9%) |
195 (85.2) |
|
|
| Authoritarian parenting practice |
Yes |
7 (4.2%) |
19 (8.3) |
0.84 (0.28-2.49) |
|
| |
No |
160 (95.8%) |
210 (91.7) |
|
|
| Money |
Yes |
10 (6.0%) |
17 (7.4) |
1.42 (0.56-3.62) |
|
| |
No |
157 (94.0%) |
212 (92.6) |
|
|
| Husband/boyfriend |
Yes |
5 (3.0%) |
2 (0.9) |
1.52 (0.26-8.99) |
|
| |
No |
162 (97.0%) |
227 (99.1) |
|
|
| Sexually related |
Yes |
10 (6.0%) |
16(7.0) |
0.62 (0.23-1.77) |
|
| |
No |
157 (94.0%) |
213 (93.0) |
|
|
| Wife/girlfriend |
Yes |
2 (1.2%) |
11 (4.8) |
0.58 (0.11-3.30) |
|
| |
No |
165 (98.8%) |
218 (95.2) |
|
|
*Significantly associated variables at p-value ≤ 0.25 in bivariate analysis. Variables included in the multivariate analysis were: alcohol influence, revenge/indemnity, neglected parenting practice, Land ownership conflict and Low socio-economic status.
@Variables significantly associated with IIPPVI at p-value ≤ 0.05 after multivariate analysis.
**Socio-economic status category: low (<=1000ETB), Medium (1001-5000ETB) and High (>=5001ETB)
Source: Nigusse Regassa, Poverty and housing status: Hawassa city, Southern Ethiopia: 2016.
Discussion
The prevalence of intentional interpersonal physical violence related injury at South Ari district was 42.2 %. The result of this study was slightly lower than the hospital based secondary data analysis reports on the magnitude and pattern of injuries conducted in Gondar university hospital (47.24%) [24] and Jima university specialized hospital (49.1%) [22]. A possible explanation of the difference may be due to the variation in the source of data since the current study is based on primary data sources, while the studies conducted in Gondar university hospital and Jima university specialized hospital were a review of secondary data from ward logbooks, charts, registrations and other secondary data sources for injury [22]. Data completeness issues in secondary data analysis may also contributed for the difference [22]. The finding of this paper is much higher than the finding from a hospital based descriptive cross sectional study on the burden of intentional injuries in Mwanza City, north-western Tanzania conducted at a tertiary hospital (23.7%) [25]. This may be due to the fact that the difference in study population and study setting, since the current study was done in one urban and eight rural health centers of the district where every traumatized individuals are expected to visit this health facilities while the study conducted in Tanzania was at the referral hospital level where obviously, majority of cases who attend this type of health institution are as referral cases so that the chance of getting some moderate and all mild cases is low [26,27].
The finding of this study is much lower than the report of primary data analysis (92%), obtained from the public hospital based cross sectional study conducted in Jamaica by the injury surveillance system of the country’s ministry of health throughout 2010 GC. The possible explanation for this may be due to the difference in the duration of the study along with seasonal variation because of variation in social behavior and predisposing factors [28]. The magnitude of interpersonal conflict related injury is expected to decrease during harvesting and planting seasons of a year as majority of the population spent the day on working but slightly increase during the seasons when the population is out of work [29]. The study conducted in Jamaica encompassed all the four seasons of the year 2010 which increases the probability of getting adequate number of injury cases that visit the hospital [21,23] unlike the current study, which was conducted within three months of the year 2018(from January to April) during this time, majority of the population at the district spent their time on harvesting crops and this may lower the magnitude of conflict related injury from the finding in Jamaica.
In this study, land ownership conflict was significantly associated with inter personal physical violence related injury. Individuals have the risk of 2.18 times more likely to sustain intentional interpersonal physical violence related injury due to land ownership disputes in the district. This is supported by the findings of a study conducted in Gondar, Ethiopia. According to this study, individuals have the risk of around two times more likely to sustain conflict related physical injury due to land ownership disputes [22].
Alcohol drinking also found to be another important variable associated with intentional interpersonal physical violence related behavior and injury for this study. Individuals who drink alcohol were 3.39 times more likely to visit the emergency department of the health centers at South Ari district due to interpersonal physical violence related injury. This is similar to findings with the world health organization; around 45% of the victims who visited to the ED had history of alcohol consumption before they sustained injury and findings from three referral hospitals at Amhara region indicated that patients who had reported to use alcohol were 2.16 times more likely to present for conflict related injury [2,4,6].
The study has also indicated that victims with low socio economic status (average monthly income <1000 ETB) were 1.73 times more likely to visit the emergency department of the health centers due to conflict related injury. The result is in line with a study conducted by WHO which revealed that low and middle income regions are the most affected by assault especially African Region with a rate of 10.7 per 100 000 population [4] and a hospital based cross sectional study on prevalence of injuries in three referral hospitals at Amhara region indicated that inter personal conflict injury is high in individuals with average monthly income less than or equal to 34.2USD [26,27]. The possible explanation for this is, individuals with low socio economic status are more likely to be exposed to harsh behavior for conflict and violence like gangster and robbery acts to earn their daily bread [4].
This study has also indicated that, individuals with neglected parenting practice have the risk of 7.97 times more likely to visit EDs for conflict related injury. According to the study conducted by world health organization 2014, children who are the family members of neglected parenting care have three times more risk of developing violent behavior and conflict related physical trauma [4]. This is due to the probability of exposure to the cause of assault and dating of violence act and risky behavior [4].
Limitation of the study was: Since the study was conducted in health institutions, merely in emergency departments of the health centers, it cannot be generalized to the population living in the catchment area and prevalence of intentional interpersonal physical violence related injury may be overestimated [30-33]. In addition, the time period of the study may also create a selection bias in the results, as injury patterns have been shown to vary seasonally; this could affect the number of injured patients to the emergency room, limiting the interpretation of the results. Furthermore, since the study focused only on the human factor of intentional interpersonal physical violence related injury the other factors remained untouched and may create bias to the findings.
Conclusions
We can conclude that the magnitude of intentional interpersonal physical violence injury is considerably high in South Ari district health centers’ emergency department visits. Among the factors; land ownership conflict, low socio-economic status of households, neglected parenting practice and alcohol influence were remained significantly associated with assault related injury. Recommended awareness creation should be done about the causes, consequences and prevention measures of intentional interpersonal physical violence related injuries at community level. Land ownership competitive disputes should be alleviated with collaborative effort of the district’s governmental bodies and the community. Families should supervise their children to prevent them from risky/un-recommended/places and behaviors for assault and education shall be given in schools about the outcomes of attending such places by using Mini- Medias and clubs. Alternative measurements for sustainable incomes generation should be arranged by the government (create opportunities for entrepreneurship, promoting saving habits and others). Use any opportunities to give health education about the consequences of alcohol drinking aiming to halt or decrease drinking habits. Further studies should be conducted about non -human causes and factors of violence behavior separately from the human ones. Further community based studies shall be conducted to know the nearly actual status of intentional interpersonal physical violence related physical injuries.
Acknowledgment
First of all, I would like to give my heartily thank to my advisor Mr. Wondewosen Teklesilassie (MPH, PhD- candidate) for his willingness and readiness to invest his priceless support throughout the work, recommending and directing my work towards the scientific world of performing activities. The contribution of other peoples is also appreciable and crucial throughout this work and deserved many thanks.
I would also like to give thanks to South Ari district administration, health office and other sectors for their delighting support. I have many thanks to Hawassa University College of Medicine and Health Science, for providing financial support and permission of my interested title to deal upon it.
Finally, I have a great thank for South Omo Zonal health department head Mr. Mintesinot Melka for his very essential regulatory and supporting work to make my activities hospitable, Mister Tilahun (driver) and other staffs that will play crucial role for my work from starting to the end.
29715
References
- Safari S (2016) International violence injuries predisposing factors as seen at CHUK and CHUB.
- Babu BV, Kar Sk (2010) Domestic violence in Eastern India: Factors associated with victimization and perpetration. Public Health 124: 136-148.
- World Health Organization (2014) Global Health Observatory Data Repository.
- (2013) United Nation Office on Drugs and Crime: Global study on homicide. Vienna.
- (2014) Center for Disease Control and Prevention: Injury prevention and control.
- United Nations Office on Drugs and Crime (2019) Global study on homicide.
- Mensur O, Yigzaw K, Sisay A (2003) Magnitude and Pattern of injuries in North Gondar Administrative Zone, Northwest Ethiopia. Ethiop Med J 41: 213-220.
- Taye M, Munie T (2003) Trauma Registry in Tikur Anbesa Hospital, Addis Ababa, Ethiopia. Ethiop Med J 41: 221-226.
- Seedat M, van Niekerk A, Jewkes R, Suffla S, Ratele K (2009) Violence and injuries in South Africa: Prioritizing an agenda for prevention: Lancet 37: 11-22.
- Corso PS Mercy JA, Simon TR, Finkelstein EA, Miller TR (2007) Medical Costs and Productivity Losses Due to Interpersonal and Self-Directed Violence in the United States. Am J Prev Med 32: 474-482.
- National Center for Injury Prevention and Control (2011) Web-based injury statistics query and reporting system (WISQARS), Atlanta GA.
- Mwashambwa MY, Kapatalata SN, Akoko LO (2015) Intentional injury; The experience of Dodoma regional hospital, Central Tanzania. East Cent Afr J Surg 20.
- Norman R, Matzopoulos R, Groenewald P, Bradshaw D (2007) The high Burden of Injuries in South Africa. Bulletin of the World Health Organization 85: 695-702.
- Abrahams N, Jewkes R, Martin LJ, Mathews S, Vetten L, et al. (2009) Mortality of women from intimate partner violence in South Africa: a national epidemiological study. Violence Vict 24: 546-556.
- Norman R, Schneider M, Bradshaw D, Jewkes R, Abrahams N, et al. (2010) Interpersonal violence: an important risk factor for disease and injury in South Africa. Popul Health Metr 8: 32.
- Center for Diseases Control and Prevention (2007) Intimate partner violence overview.
- Tingne CV, Shirigiriwa M, Ghormade PS, Kumar MB (2014) Quantitative analysis of injury characteristics in victims of interpersonal violence: An emergency department perspective. Journal of Forensic and Legal Medicine 26: 19-23.
- Odujinrin O (1993) Wife battering in Nigeria: Int J Gynaecol Obstret 41: 159-164.
- Nicol A, Knowlton LM, Schuurman N, Matzopoulos R, Zargaran E, et al. (2014) Trauma Surveillance in Cape Town, South Africa: An Analysis of 9236 Consecutive Trauma Center Admissions. JAMA Surg 149: 549-556.
- Seedat M, van Niekerk A, Suffla S, Jewkes R, Ratele K (2009) Violence and injuries in South Africa: prioritizing an agenda for prevention.
- Kalesan B, Mobily ME, Keiser O, Fagan JA, Galea S (2016) Firearm legislation and firearm mortality in the USA: a cross-sectional, state-level study. The Lancet 387: P1847-1855
- Sir Liam Donaldson Chief medical officer for England (2009) Guidance on the consumption of alcohol by children and young people.
- (2008) Susanne Tonsing and Sandy Lazarus: Risk and protective factors to male interpersonal violence.
- (2016) South Omo zone health department and Natural Resource and Agro Forestry Office: joint report on zonal districts’ profile, Ethiopia.
- (2015) South Ari district Custom and Tourism Office: population biography report.
- Woldemichael K, Berhanu N (2011) Magnitude and Pattern of Injury in Jimma University Specialized Hospital, South West Ethiopia. Ethiop J Health Sci 21: 155-165.
- World Health Organization (2013) Definition of key terms: Consolidated ARV guidelines.
- Bashah DT, Dachew BA, Tiruneh BT (2015) Prevalence of injury and associated factors among patients visiting the Emergency Departments of Amhara Regional State Referral Hospitals, Ethiopia: a cross-sectional study. BMC Emerg Med 15: 20.
- Davis A (2008) FOCUS. Views from the National Council on Crime and Delinquency. Interpersonal and Physical Dating Violence among Teens.
- Ayele TA, Zeleke BM, Tessema GA, Melak MF (2017) Magnitude and patterns of injuries among patients in Gondar University Hospital, northwest Ethiopia: an institutional-based study. Open Access Surgery 10:25-31.
- Chalya PL, Gilyoma JM (2012) The burden of intentional injuries in Mwanza City, north-western Tanzania: a tertiary hospital survey. Tanzan J Health Res 14: 204-211.
- Crawford TV, Mcgrowder DA, Barnett JD, Shaw-Sanderson JH (2014) Epidemiological Features of violence-related Injuries in Jamaica. J Clin Diagn Res 8: JC01–JC04.

