Key words
Substance abuse, street children, prevention, India
Introduction
Estimating numbers of ‘street children’ is fraught with difficulties. The exact number of street children is impossible to quantify, but the figure almost certainly runs into tens of millions across the world which shows that the numbers are in increasing trend’. [1,2] The number of street children has grown in recent decades because of widespread recession, political turmoil, civil unrest, increasing family disintegration, natural disasters and growing urbanisation. [3]
The problems of street children are more significant in the developing than developed world and it was estimated that more than 100 million children live and work on the streets in the developing countries. [4,5] Moreover, India alone is home to the world’s largest population of street children, estimated to be 18 million. [4]
Some estimates put the number of street children living in India’s six most populous cities at 500,000; more than 100,000 may be found in Delhi alone. [1,2,6] War, poverty, urbanization, rapid economic growth, the breakdown of families, and domestic violence are the most immediate causes of this phenomenon’s growing proportions. [7] Street children in India indulge in substance use at any time in their life and the minimum age at starting substance use in the study was 5 years. [6] Street children are abusing wide range of substances, from inhalant to solid cigarettes and some of the children are employed in preparation of "charas" cigarettes in India. [7,8] This situation brought the street children in various health and social effects. As a result, over half of the 18 year-old street girls reported Sexually Transmitted Infection (STI) and, and 20% of them admitted due to early pregnancy. [9]
To combat the causes and consequences of substance abuse among street children through preventive programmes it is important to understand how children end up on the streets in the first place. The aim of literature review was to identify the factors that put children on the streets, understand the context of substance abuse among street children and released health problems in order to develop a framework that can help in preventing substance abuse by street children. A conceptual framework was designed following the study to show the broader concept of causes, effects, and preventive strategies for the prevention of substance abuse among street children in India.
Conceptual framework
A conceptual framework on preventive strategies for substance abuse among street children was developed following the study on substance abuse among street children in India. The framework was built from three key components: causes, health outcomes and interventions. Individual, family level and structural causes are responsible for the children to be on the street. Street children start abusing substances, like alcohol, tobacco and drugs. As a result health and social effects are seen among them. To combat causes and consequences of substance abuse among street children, interventions from government and non-government level are shown in the conceptual framework. Figure 1 links the causes of street children to leave their homes and live on the street to the possible health outcomes that they faced during street. Besides this, it shows the link of two different intervention strategies to combat cause and consequences of substance abuse and street children as mentioned in figure 1.
Methodology
The literature review process was done through databases searching and grey literature citation index (Figure 2). After searching, the publications were processed for screening, analysis and review with necessary exclusions before the paper used for generating findings and synthesis discussion. [10]
Figure 2: Literature review process and selection of articles
Searching Strategies
Databases searching
Databases used to collect academic literature were Academic Search Premier, Google scholar, Medline/Pubmed. This method involves databases search from 1990 according to problem based keywords. It involves listing of abstracts for the initial set of several articles, articles reviewing to provide a broad mapping of the problem and finally mini and micro level analysis of selected articles focusing the objectives and problems of study.11 Keyword search used in the study were “Substance abuse”, “Street children”, and for narrow search “Substance abuse AND Street children” was done. The search was done as per the chapters, for demography and epidemiology, “Demography of Street Children” and “Epidemiology of Substance Abuse”. Additionally, for causes and effects of substance abuse and children being on the street, “Causes of Substance Abuse”, “Causes of Street Children”, and “Effects of Substance Abuse” were used. Finally, for implemented programmes, “Preventive Programmes for Street Children” and “Programmes Preventing Substance Abuse” were used.
Grey literature Citation Index
Grey literature include the references identified through the previous search strategy which were examined in order to compile a citation index of the books, book sections and reports referred to. References that were cited more than four times were sought for inclusion in this review. This was done to ensure that important grey literature was included in the review. Here, the published data and information from NGOs, INGOs, WHO, UNICEF, Save the Children, Eldis, Consortium for Street Children and Departments of Indian government were used.
Screening process
Inclusion criteria were developed to screen the literature identified for inclusion in the analysis. Recent, relevancy and English language were the major inclusion criteria. To ensure that the literature covers a long enough timeframe to be comprehensive but not so long as to be outdated published documents form 1990 were taken. For relevancy, documents related to the causes of children being on the street, substance abuse and preventive strategies were focused. Finally English language was taken to ensure that the article can be assessed by the review team.
Analysis
Analysis of the data was done utilising a grounded theory approach and thematic coding.
The major strategy of grounded theory employed in this research was constant comparative method. Constant comparative analysis is the process of coding data to develop concepts which are then refined by reviewing and comparing other data. On the basis of these comparisons concepts may be confirmed, discarded, refined or elaborated, and their relationships to one another are explored. [10]
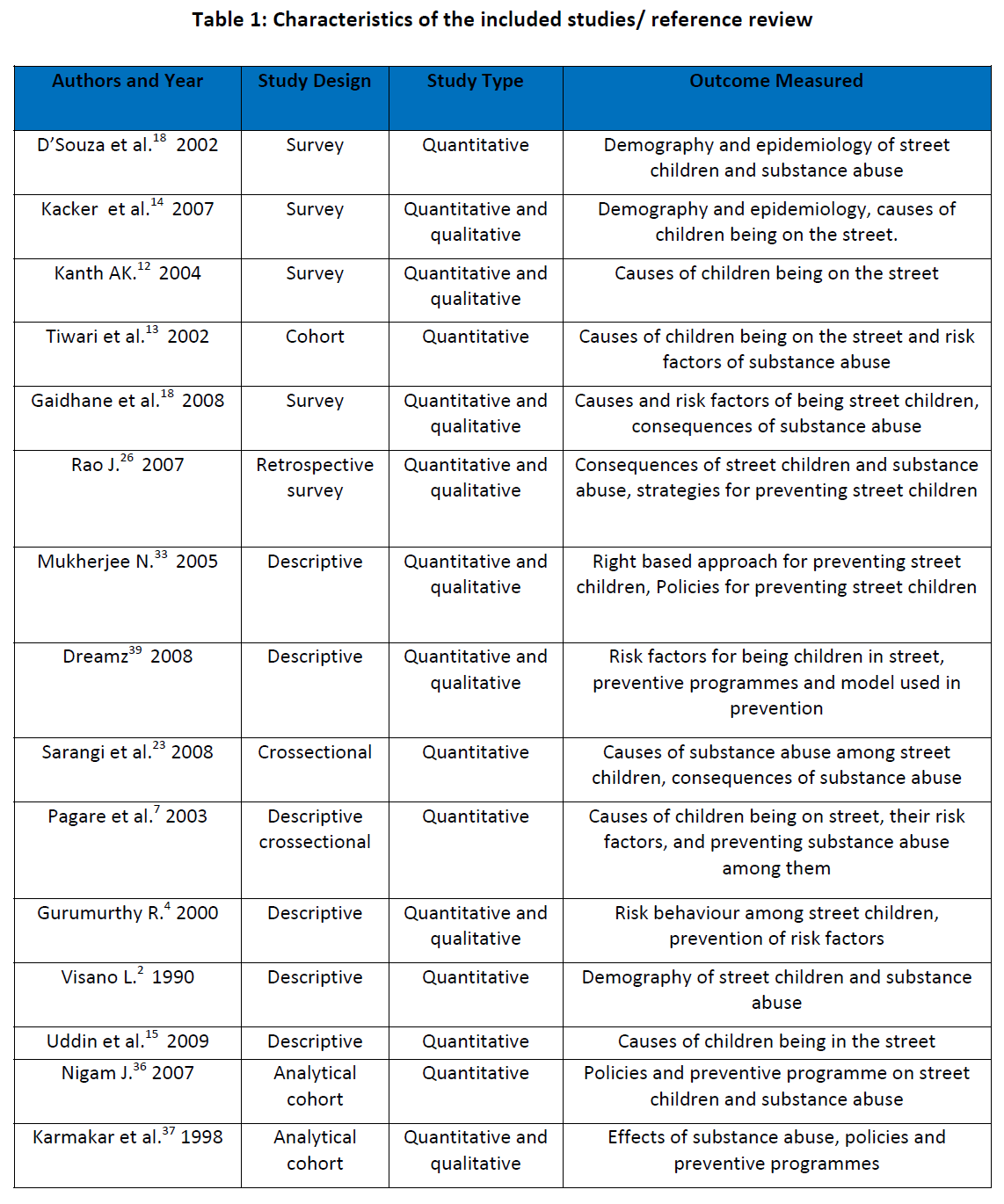
The text in each reference review document (see table 1) was thematically coded to facilitate the retrieval of text in relation to specific outcomes. Attributes were also assigned to each reference based on those identified in the assessment of document attributes, outcomes and objectives.
Finally, search and analysis within the PDF file was done to identify the content of each chapters and objectives. There were 15 academic articles which were used in this study, about substance abuse and street children in India.
Assumptions underpinning this review
This review process may not include some source of information, like published reports due to practical difficulties inherent in identifying and obtaining these reports. Other unpublished sources tend to be more highly valued within a field but inaccessible in this review.
Literature review process and selection of articles
Review and selection of the article was done as shown on figure 2 and necessary study exclusion was done as below.
Study Exclusions
Exclusion 1 (n1): After searching articles, during screening process the articles get excluded which were irrelevant in the topic and abstract. Topic related to medicine and drug therapies of substance abuse were excluded. After this, papers were analysis by re-evaluation.
Exclusion 2 (n2): Here, during review the papers which were duplicated and not relevant to objectives were excluded. After this, papers were retrieved for data extraction.
Exclusion 3 (n3): Here, the study exclusion was done on the basis of those papers which were not from India. After this, papers were included for synthesis of result and discussion.
Results
It has been found that a total of fifteen studies meet all the criteria and their selection was done as mentioned in figure 2. Review of the studies was done and the findings were synthesised in the study.
General overview of studies
Out of 15 academic articles that were used in this study, each of the articles was responsible to demonstrate more than one outcomes of the finding. It was found that six articles studied the causes of children being on the street, five articles studied the causes of substance abuse and risk factors, five articles studied effects and consequences, and six for policies and preventive programmes for preventing street children and substance abuse. Beside these, several publications from government and non-government organisations were used to support the findings of academic articles. The included studies were conducted mainly in the cities of India like Mumbai, Delhi, Chennai, Calcutta, Tamil-nadu, Sambalpur, Banglore and Orissa. However, the study design and study type varied according to the methodological quality (table 1).
Causes of children being on the street in India
Children who are vulnerable to street life include those who have been abandoned by their families or sent into cities due to family's intense poverty, often with hopes that a child will be able to earn money for the family. [12] It was found that most of the street children were from joint families and higher percentage of street children had illiterate parents. [13] Beside these, low income of the parents, presence of step parents, guardian other than parents and intra-familial physical abuse were associated with the runaway group of street children in India. [14,15]
Demography and epidemiology of street children and substance abuse in India
There is high burden of street children in India, which accounts 10% of world street children and despite efforts by the government and many NGOs, the number does not diminish or their plight grow better. [7,16] It was found that 11 million street children were in India where 82.7% of street children were boys whereas girls were more difficult to trace and were most vulnerable. [14,17] There was uneven distribution of street children where West Zone has more than half of the street children of India. [16,18] Various abuses were experienced by street children, where 82.98% of street children were substance abusers. [19] The most common substance consumed was nicotine, as cigarettes or "bidis’ and "gutkha" and inhalant / volatile substance use in the form of sniffing of adhesive glue, petrol, gasoline, thinner and spirit was reported by one fourth of children. [8,18,20] Beside these, drugs were used by street children. Heroin, Opium, Alcohol, Cannabis and Propoxyphene are the five most common drugs being abused by children in India. [7] Furthermore, the study explored that the substance abuse by street children is influenced with tendency of substance abuse by their family members. Similarly, Benegal et al shows that family members of street children use tobacco and alcohol and street children are more prone to use drugs and other substances. [21]
Causes and risk factors of substance abuse among street children in India
Almost three-quarter (70 %) of all substance users wanted to quit and about 40% had tried to quit but cannot, due to the associated causes of substance abuse. [19] This study showed the most common reasons for substance abuse by street children were peer pressure (62.1%), experimentation (36.3%) or to boost self-confidence (28.7%). Various Indian Foundations state that children abuse substances for a number of reasons, from curiosity, recreation to cope with stress as personal factors however drug abuse and addiction lead to a complex set of social, medical and economic problems. [20] Regarding risk factors, substance abuse was significantly associated with domestic violence, maltreatment of the child, nuclear families, runaway status and working status of the child. [7]
Health and Social effects of substance abuse among street children
Childline India Foundation states that even a single session of repeated inhalant abuse can disrupt heart rhythms and cause death from cardiac arrest or lower oxygen levels, enough to cause suffocation. [6,19] In Manipur, north-east India, which shares border with Myanmar, and Madras, are the examples where rapid increases of heroin injection take place mainly in street children and they have high rated of HIV/AIDS and STDs transmission rate. [22] The effects of substance abuse were lung problems (28%) like burning of lungs and tuberculosis (6%), vomiting (12%), cancer (11%), death (10%), teeth and facial problem (7%), heart or kidney problems (5%). [7] Besides these, a peer influence contribute significantly on higher level of adolescents using drugs i.e., (48.3%) had an addicted peer. [7,23] Furthermore, the majority of substance abusers either never went to school (54.4%) or were school drop-outs (51.7%) and the most common place for initiation of substance abuse was recreational avenues for males (49.7%) and home for females (36.6%). These adverse social effects, resulting homeless children are involved in robberies, prostitution, trafficking drugs and even murders in urban areas of the country. [24]
Policies and strategies on substance abuse among street children in India
The Government of India ratified the Convention on the Rights of the Child on 12 November 1992. [25] The Government took various initiatives to review the National and State legislations and brought it in line with the provisions of the Convention. Furthermore, the Government developed appropriate monitoring procedures to assess progress in implementing the Convention, which involve all relevant Ministries and Departments, international agencies, NGOs, and the legal profession in the implementation and reporting process. [7,26] The National Plan of Action has been worked out keeping in mind the needs, rights and aspirations of 300 million children in the country and sets out quantifiable time dimensions to India's Charter of Action for Children. [24] The Plan gives special consideration to children in difficult circumstances and aims at providing a framework, through the goals and objectives for actualisation of the Convention in the Indian context. [25] The Government of India had adopted a two-pronged strategy to tackle the problem of drug and substance abuse which includes supply control and demand reduction. [19,20,26] Similarly, Manihara states that the laws under the Juvenile Justice Act 1986, India relate quite strongly to the care and rights of street children and strategy for preventing substance abuse in general, however lacks in implemention. [16]
Programmes for preventing children on the street in India
The Integrated Programme for Street Children is a national programme operating in 56 cities in India. [27] The programme targets homeless children living alone, or with their families, on the street. It provides education, health care, nutrition and legal help and seeks to reunite runaway children with their families. [28] These components could strengthen family and children not to leave their home and prevent children living on the street. For example, in Tamil Nadu, Andhra Pradesh and West Bengal, Integrated Programme for Street Children provide support on bridging courses and alternative education for working children, girls, children from certain castes and tribal groups. [26,29]
An Integrated Programme on Street children in India constitute city wise surveys, where competent institutions carry out an enumeration of street children in all state capitals as well as in other cities having population of 1 million or more. [27,30] However, the cities with less than 1 million populations are not included in the programme where there might be high number of street children. [25] The programme documents existing facilities in the city for street children, formulation of plans, co-ordination with the different stakeholders, advocacy and awareness generation on the right of children, training NGOs, facilitating street children for community participation and advice government on formulation of policies and programmes of street children. [29] Besides the national programme many NGOs working for the prevention of the children being in the street and provide their needs. For Example, street and working children in Dindigul and Palani of India were offered immediate care and support at 24-hour drop-in centres located in each town. [31] Evaluation of an Integrated Programme on Street Children was done by performance appraisal mechanism. [32] In Delhi Mukherjee used “rights based approaches”, “empowerment and capabilities approaches” and “sustainable livelihoods approaches”, to evolve multiple yardsticks for participatory monitoring framework for street children from their perspectives and also for benchmarking achievements of programmes and projects related to them. [33]
Programmes for preventing substance abuse among street children in India
A national master plan for substance abuse was evolved in 1994 which focuses on the establishment of treatment and rehabilitation centres, training in substance abuse for primary care doctors and other personnel, collaborating with non-governmental organisations and carrying out education and awareness building programmes. [19] There are currently in India about 359 counselling centres for drug abuse prevention that also propagate awareness and the government finances more than 50 NGOs, which are engaged in drug and substance abuse prevention activities. [34] A tripartite agreement between the Government, ILO and UNDCP has been signed to help full rehabilitation and recovery of substance abuse and drugs. [18] Integrated Child Protection Scheme (ICPS) was launched in India aiming at creating safe and secure environment for children in need of care and protection for children in conflict, vulnerable and street children and preventing substance abuse among children. [32] India has adopted the Modified Social Stress Model for preventing substance abuse among street children in different cities and use WHO categories of response. [35,36] A cross-sectional, community-based study conducted among children residing in the slums of Sambalpur, and Orissa of India conceptualised by the Modified social Stress Model that an increased risk for drug use stems from distress, the normalization of drug use, the effect of drugs and a decreased risk of drug abuse due to social attachments, coping strategies, resources for their development. [22,37] The study done in Banglore, India supports the model that increased risk for drug use is a function of the level of perceived personal stress. However, the risk decreased by positive attachments that the child may have, the possession of adequate coping strategies and skills, and access to necessary resources. [20]
Discussion
It has been found that India has the highest number of street children in the world, however the number differs on different reports and most of them show more than 11 million street children living and working in Indian street. [16] Most of the street children were boys from the scheduled caste or tribes, which shows the poverty is the major cause among those groups. There was uneven distribution of street children where West Zone has more than half of the street children of India. [18] It was due to the major cities located in this Zone and numbers of children were high in these cities. However, demographic investigations on number of street children is limited and not conducted beyond the major cities.
It was found that the Indian street children face both the individual or family and community or social causes to be on street and abusing the substances as mentioned in conceptual framework. Thus, Kanth identified family intense poverty was responsible for children being on the street and family expectation for earning money. [12] However, Tiwari et al., [13] focus on illiteracy and joint family are the main cause of children being on the street in India along with the poverty, physical abuse being subsidiary causes. This supports the hypothesis of Aptekar, [38] that urban poverty is the major reason of children being on the street followed by aberrant families. On the other hand, the most common causes of substance abuse among street children in India were peer pressure followed by experimentation and boosting self confidence. [18] However, it differs from the main cause of children being on street which was poverty. Curiosity, recreation and coping with the stress were other factors influencing for the use of substance by street children in India. [19] Furthermore, Childline India Foundation states that the vital organs are mostly affected and inhalers got disruption of heart rhythm and cardiac arrest by substance abuse. Beside these, high rates of HIV and STDs transmission was among street children in north-east of India. Thus, the studies included on the review also suggest those effects on street children.
The policies, strategies and programmes for preventing substance abuse among street children in India are using WHO guidelines and initiatives. PSA of WHO was a benchmark for India in implementing programmes and the problems of high number of street kids were addressed through at Integrated Programme on Street Children in India. [26] However, there are some gaps of the Integrated Programme on Street Children that it could not cover all the street children of the country and limited to the major cities. [25] Beside the national programmes, other community oriented programmes for preventing children being on street were implemented in Dindigul, Palani, Mumbai, Delhi and many other parts of the country addressing the specific issues. [30,32,39] This shows that different organisation used different approaches providing basic needs, child rights and improving their career. On the other hand, preventing substance abuse and their effects among street children implemented as preventive approach including health based intervention as mentioned in conceptual framework.
A national plan for substance abuse was significant for treatment, rehabilitation, and awareness building for street children to prevent substance abuse. [19] However, counselling centres and awareness programmes were inadequate to change the behaviour of the people. Additionally, Government of India launched Integrated Child Protection Scheme (ICPS) for safe and secure environment for children and preventing substance abuse among them. [33] Modified Social Stress Model for preventing substance abuse among street children used WHO categories of response in India. Sambalpur, Banglore and Orissa State used this Model by controlling over the factors which increased the risk of substance abuse and promoting the factors which decreased the risk due to social attachments, coping strategies and resources. [22] Similarly, Frost [40] suggested that providing information and awareness using HBM could be appropriate for preventing substance abuse among street children. Thus, the multiple approaches were implemented in India for the prevention of substance abuse among street children in India. However, programmes related to different culture, tradition, geographical location, empowerment and employment are further essential to prevent root causes and consequences of substance abuse and street children in all part of the country.
Conclusions
There are relatively few studies conducted in relation to substance abuse among street children India although, they comprise a significant proportion of the total population. Most of the study focuses on the causes, effects and risk factors of substance abuse among street children in India and very few academic papers on prevention. However, the additional preventive programme and policies were discussed from government and organisational publications.
It was found that there were variation in findings of the study and the study were carried mostly in the urban areas of the country. The programmes need special focus on reducing poverty in the country and peer pressure for preventing substance abuse among street children. Furthermore, for the sustainability of the programme they need sustainable resources and their effective planning.
References
- UNICEF Rapid Assessment of street children in Lusaka. UNICEF, 2002; Available from: https://www.unicef.org/ evaldatabase/files/ZAM_01-009.pdf. (Accessed 21 Nov 2009).
- Visano L. The socialization of street children: The development and transformation of identities. Sociological Studies of Child Development, 1990; 3:139-161.
- Tuladhar S. Alcohol and Drug Use among Street Children in Nepal. Kathmandu: Child Workers in Nepal (CWIN); 2002.
- Gurumurthy, R. HIV/AIDS risk taking behaviour among street children in Mumbai, Mumbai: International Conference on AIDS; 2000.
- Joshi NC. Integrated Child Protection Scheme- taking care of overall care of overall development of children. The India Post; 2009; Available from: https://www.theindiapost.com/articles/ integrated-child-protection-scheme-–-taking-care-of-overall-development-of-children/. (Accessed 25 June 2010).
- Harold E. Concepts of Chemical Dependency, California: Brooks/Cole-Thomson Learning; 2002.
- Pagare D, Meena GS, Singh MM, Saha, R. Risk Factors of Substance Use Among Street Children from Delhi, New Delhi: Maulana Azad Medical College; 2003.
- Rao J. The History of Child Right in India. UNICEF, India; 2007; Available from: https://www.unicef.org/india/children_3220.htm. (Accessed 5 July 2010).
- UN-ODCCP. Rapid situation assessment of street children in Cairo and Alexandria. Cairo: UN-ODCCP; 2001.
- Harris-Roxas B, Simpson S, Harris E. Equity-Focused Health Impact Assessment A Literature Review. Australasian Collaboration for Health Equity Impact Assessment (ACHEIA); Sydney; 2004.
- Gilson L, Raphaely N. Health policy and planning, London: Oxford University Press; 2008.
- Kanth AK. Street Children and Homelessness. CYC-Online; 2004; Available from: https:// www.cyc-net.org/cyc-online/cycol-0904-Homelessness.html. (Accessed 24 May 2010).
- Tiwari PA, Gulati N, Sethi GR, Mehra M. Why do some boys run away from home- Indian Journal of Paediatrics; 2002; 69(8):732.
- Kacker L, Varadan S, Kumar P. Study on Child Abuse India 2007. Delhi: Ministry of Women and Child Development, Government of India; 2007.
- Uddin J, Koehlmoos TL, Ashraf A, Khan AI, Saha NC, Hossain M. Health Needs and Health Care Seeking Behaviour of Street Dwellers in Dhaka and Mumbai. Health Policy and Planning, 2009:24(5)1–10.
- Consortium for Street Children. Street children Statistics. Consortium for Street Children, 2009; Available from; https://www.streetchildren.org.uk/_uploads/resources/StreetChildren_Stats_FINAL.pdf . (Accessed 20 March 2010).
- Manihara NS. Street Children- SKCV; 2006; Available from: https://www.skcv.com/street%20children%20in%20india.htm. (Accessed 1 July 2010).
- D’Souza B, Castelino L, Madangopal DA. Demographic Profile of Street Children in Mumbai. Mumbai: Shelter Don Bosco Research Documentation Centre; 2002.
- Gaidhane AM, Zahiruddin QS, Waghmare L, Shanbhag S, Zodpey S, Joharapurkar SR. Substance Abuse Among Street Children in Mumbai. London: Routledge; 2008.
- Childline India Foundation (2010) Drug abuse among children. [Online] Available from: https://www.childlineindia.org.in/index.htm. [Accessed 21 May 2010].
- Benegal V, Bhushan K, Seshadri S, Karott M. Drug Abuse Among Street Children in Bangalore. Bangalore: National Institute of Mental Health and Neurosciences, Bangalore Forum for Street and Working Children; 1998.
- UNDCP The Social Impact of Drug Abuse. Available from: https://www.unodc.org/ pdf/technical_series_1995-03-01_1.pdf. (Accessed 24 May 2010).
- Sarangi L, Acharya HP, Panigrahi OP. Substance Abuse Among Adolescents in Urban Slums of Sambalpur. Indian Journal of Community Medicine 2008; 33(4): 265-267.
- Patro BB. (1997) India-AIDS: Street Children are Most Vulnerable. [Online] Available from: https://www.aegis.com/news/ips/1997/ip970902.html. (Accessed 29 May 2010).
- Consortium for Street Children Street children Statistics. Available from https://cfsc.trunky.net/_uploads/resources/StreetChildrenStats FINAL.pdf. (Accessed on 20 March 2010).
- Rao J. The History of Child Right in India. UNICEF, India; 2007; Available from: https://www.unicef.org/india/children_3220.htm. (Accessed 5 July 2010).
- I-India. Giving Street Children a Future. I-India; 2010; Available from: https://www.i-indiaonline.com/prog_ ISS.html. (Accessed 21 June 2010).
- Women Welfare Department India. An Integrated Programme for Street Children. Women Welfare Department India: Government of Utter Pardesh; 2007.
- Save the Children (2009) Making Children Rights a reality. Save the Children; 2009: Available from: https://www.savethechildren.org.uk/en/docs/POlicy_Brief_Making_ childrens_rights_reality.pdf. ( Accessed 25 June 2010).
- Ministry of Social Justice and Empowerment. An Integrated Programme for Street Children 2007. Available from: https://www.keralawomen.gov.in/applications/ T_1221551660281-354.pdf. (Accessed 22 June 2010).
- Sahayaraj. Empowerment and Livelihoods of Street and Working Children. Tamil Nadu: Arunodhaya Centre for Street and Working Children; 2005.
- Women Welfare Department India. An Integrated Programme for Street Children. Women Welfare Department India: Government of Utter Pardesh; 2007.
- Mukherjee N. Towards Evolving a Right-Based Participatory Monitoring Tool for Sustainable Human Development and Reduction of Vulnerability of Street Children in Urban South Asia. New Delhi: Development Tracks in Research; 2005.
- Ministry of Women and Child Development India. The Integrated Child Protection Scheme. Government of India: Ministry of Women and Child Development; 2007.
- WHO Substance Use, Health and Street Children, WHO, Geneva; 1993; Available from: https://pangaea.org/street_children/world/who2.htm. (Accessed 28 March 2010).
- Nigam J. Street children in India: a glimpse. Journal of Health management 2007 Jan- June: 7 (1): 63-71.
- Karmakar T, Bandyopadhyay T, Seal A. International Conference on AIDS, Assessment of sexual health status among the street children in the city of Calcutta. Calcutta: Vivekananda Education Society; 1998.
- Aptekar L. Street Children in the Developing World: A Review of their Condition, California: San Jose State University; 1994.
- Dreamz Home for Homeless Children. Mumbai: Social Development Centre and Smile Foundation; 2008.
- Frost R. Health Promotion Theories and Models for Programme Planning and Implementation. Arizona: University of Arizona; 2008.
3042
References
- UNICEF Rapid Assessment of street children in Lusaka. UNICEF, 2002; Available from: https://www.unicef.org/ evaldatabase/files/ZAM_01-009.pdf. (Accessed 21 Nov 2009).
- Visano L. The socialization of street children: The development and transformation of identities. Sociological Studies of Child Development, 1990; 3:139-161.
- Tuladhar S. Alcohol and Drug Use among Street Children in Nepal. Kathmandu: Child Workers in Nepal (CWIN); 2002.
- Gurumurthy, R. HIV/AIDS risk taking behaviour among street children in Mumbai, Mumbai: International Conference on AIDS; 2000.
- Joshi NC. Integrated Child Protection Scheme- taking care of overall care of overall development of children. The India Post; 2009; Available from: https://www.theindiapost.com/articles/ integrated-child-protection-scheme-–-taking-care-of-overall-development-of-children/. (Accessed 25 June 2010).
- Harold E. Concepts of Chemical Dependency, California: Brooks/Cole-Thomson Learning; 2002.
- Pagare D, Meena GS, Singh MM, Saha, R. Risk Factors of Substance Use Among Street Children from Delhi, New Delhi: Maulana Azad Medical College; 2003.
- Rao J. The History of Child Right in India. UNICEF, India; 2007; Available from: https://www.unicef.org/india/children_3220.htm. (Accessed 5 July 2010).
- UN-ODCCP. Rapid situation assessment of street children in Cairo and Alexandria. Cairo: UN-ODCCP; 2001.
- Harris-Roxas B, Simpson S, Harris E. Equity-Focused Health Impact Assessment A Literature Review. Australasian Collaboration for Health Equity Impact Assessment (ACHEIA); Sydney; 2004.
- Gilson L, Raphaely N. Health policy and planning, London: Oxford University Press; 2008.
- Kanth AK. Street Children and Homelessness. CYC-Online; 2004; Available from: https:// www.cyc-net.org/cyc-online/cycol-0904-Homelessness.html. (Accessed 24 May 2010).
- Tiwari PA, Gulati N, Sethi GR, Mehra M. Why do some boys run away from home- Indian Journal of Paediatrics; 2002; 69(8):732.
- Kacker L, Varadan S, Kumar P. Study on Child Abuse India 2007. Delhi: Ministry of Women and Child Development, Government of India; 2007.
- Uddin J, Koehlmoos TL, Ashraf A, Khan AI, Saha NC, Hossain M. Health Needs and Health Care Seeking Behaviour of Street Dwellers in Dhaka and Mumbai. Health Policy and Planning, 2009:24(5)1–10.
- Consortium for Street Children. Street children Statistics. Consortium for Street Children, 2009; Available from; https://www.streetchildren.org.uk/_uploads/resources/StreetChildren_Stats_FINAL.pdf . (Accessed 20 March 2010).
- Manihara NS. Street Children- SKCV; 2006; Available from: https://www.skcv.com/street%20children%20in%20india.htm. (Accessed 1 July 2010).
- D’Souza B, Castelino L, Madangopal DA. Demographic Profile of Street Children in Mumbai. Mumbai: Shelter Don Bosco Research Documentation Centre; 2002.
- Gaidhane AM, Zahiruddin QS, Waghmare L, Shanbhag S, Zodpey S, Joharapurkar SR. Substance Abuse Among Street Children in Mumbai. London: Routledge; 2008.
- Childline India Foundation (2010) Drug abuse among children. [Online] Available from: https://www.childlineindia.org.in/index.htm. [Accessed 21 May 2010].
- Benegal V, Bhushan K, Seshadri S, Karott M. Drug Abuse Among Street Children in Bangalore. Bangalore: National Institute of Mental Health and Neurosciences, Bangalore Forum for Street and Working Children; 1998.
- UNDCP The Social Impact of Drug Abuse. Available from: https://www.unodc.org/ pdf/technical_series_1995-03-01_1.pdf. (Accessed 24 May 2010).
- Sarangi L, Acharya HP, Panigrahi OP. Substance Abuse Among Adolescents in Urban Slums of Sambalpur. Indian Journal of Community Medicine 2008; 33(4): 265-267.
- Patro BB. (1997) India-AIDS: Street Children are Most Vulnerable. [Online] Available from: https://www.aegis.com/news/ips/1997/ip970902.html. (Accessed 29 May 2010).
- Consortium for Street Children Street children Statistics. Available from https://cfsc.trunky.net/_uploads/resources/StreetChildrenStats FINAL.pdf. (Accessed on 20 March 2010).
- Rao J. The History of Child Right in India. UNICEF, India; 2007; Available from: https://www.unicef.org/india/children_3220.htm. (Accessed 5 July 2010).
- I-India. Giving Street Children a Future. I-India; 2010; Available from: https://www.i-indiaonline.com/prog_ ISS.html. (Accessed 21 June 2010).
- Women Welfare Department India. An Integrated Programme for Street Children. Women Welfare Department India: Government of Utter Pardesh; 2007.
- Save the Children (2009) Making Children Rights a reality. Save the Children; 2009: Available from: https://www.savethechildren.org.uk/en/docs/POlicy_Brief_Making_ childrens_rights_reality.pdf. ( Accessed 25 June 2010).
- Ministry of Social Justice and Empowerment. An Integrated Programme for Street Children 2007. Available from: https://www.keralawomen.gov.in/applications/ T_1221551660281-354.pdf. (Accessed 22 June 2010).
- Sahayaraj. Empowerment and Livelihoods of Street and Working Children. Tamil Nadu: Arunodhaya Centre for Street and Working Children; 2005.
- Women Welfare Department India. An Integrated Programme for Street Children. Women Welfare Department India: Government of Utter Pardesh; 2007.
- Mukherjee N. Towards Evolving a Right-Based Participatory Monitoring Tool for Sustainable Human Development and Reduction of Vulnerability of Street Children in Urban South Asia. New Delhi: Development Tracks in Research; 2005.
- Ministry of Women and Child Development India. The Integrated Child Protection Scheme. Government of India: Ministry of Women and Child Development; 2007.
- WHO Substance Use, Health and Street Children, WHO, Geneva; 1993; Available from: https://pangaea.org/street_children/world/who2.htm. (Accessed 28 March 2010).
- Nigam J. Street children in India: a glimpse. Journal of Health management 2007 Jan- June: 7 (1): 63-71.
- Karmakar T, Bandyopadhyay T, Seal A. International Conference on AIDS, Assessment of sexual health status among the street children in the city of Calcutta. Calcutta: Vivekananda Education Society; 1998.
- Aptekar L. Street Children in the Developing World: A Review of their Condition, California: San Jose State University; 1994.
- Dreamz Home for Homeless Children. Mumbai: Social Development Centre and Smile Foundation; 2008.
- Frost R. Health Promotion Theories and Models for Programme Planning and Implementation. Arizona: University of Arizona; 2008.



