Keywords
Renal stone, risks factors, bilhariziasis, gout. renal calculi.
Introduction
Renal calculi mean kidney stone and having a stone in any location of urinary tract is referred to as urolithisis. It is consider one of the oldest diseases which occur in the urinary tract and it rarely happens in children, it takes various in shapes and sizes and may be very small or as large as the orange size, it is the most painful urologic disorder [1,2]. An estimated 1.3 million Americans seek medical help for kidney stone each year .At the same time, studies suggest kidney stone affects over (5%) of Americans and that the prevalence has increased over the past three decades [1-3].
It may be recurrent and can be easily diagnosed through X-ray.
Formation of renal calculi may occur in kidneys, the ureters or the bladder leading to the damage of the kidneys and block the flow of urine, impair kidneys function in getting rid of body waste products and finally cause renal failure.
Many literatures and studies mentioned that there is no exact cause of urinary calculi but there are a number of genetic body reaction to certain metabolic and chemical conditions and life style risks that contribute to renal calculi formation [1,4-6].
Understanding such factors can help those at risk for developing urinary calculi in preventing this condition.
Risk factors are factors that do not seem to be direct causes of the disease, but they may be associated in some way. Having a risk factor for urinary calculi makes the chance of getting a condition higher but does not always lead to urinary calculi.
However, the reason why it occurs in some people and not in others facing the same factors is unknown [7-9].
Nurses have an important role in teaching people about how to avoid the risk factors of urinary calculi and how to prevent them, therefore, the researcher intended to find out the most common risk factors which may cause urinary calculi and to find out if there is a significant relation between those factors and other variables.
Aims of the study
The aims of this study were to identify the most common risk factors which may cause renal stone and explore if there is a significant relation between those factors and renal stone formation.
Material and method
One hundred patients out of (135) patients were diagnosed with renal stone after several investigations, such as urine analysis Ultrasonography and X-ray for kidneys ureters and bladder (K.U.B).
Patients were chosen from the Medical city and Al-Karama hospitals in Baghdad and in order to know these risk factors were unique for formation of urinary calculi (100) normal subjects were chosen as a control group after getting their agreement to participate in this study. A comparative group 100 normal subjects were selected to match patients with renal stone regarding their age, sex, marital status educational level and place of residence. The patients were selected according to the following criteria:
1.Diagnosed with renal stone.
2.Didn’t have any acute disease and had no history of or chronic diseases such as, diabetes mellitus or heart disease.
3.Their ages 18 years or older.
The study was carried out during the period between May 2008 –September 2009. After reviewing the literatures related to this disease, a questionnaire format was designed includes the following:
1.General information comprised sociodemogrphic data including, age, sex, marital, status, educational level, and area of residency.
2.8 items related to factors concerning the medical history of patients and control group.
3.11 items related to risk factors concerning the diet and drugs in patients group and control group.
The questioner was revised by 10 expertises in this field for validity and the result showed (96%) agreement. On the basis of their feedback 3 items were changed and 2 items were added.
An Interview technique was used as a method for gathering data, the researcher and her assistants completed the questionnaires and all patients with renal stone from the two hospitals agreed to participate in this study after getting the permission from the two hospitals.
In addition, patient's files were checked for urine analysis to find out if the patients had increases in uric a cid and calcium, their x-ray (K.U.B) were checked too.
Data analysis was done through frequency, percentage, t test and chi square.
Results
To find out the differences between the sample patients and the control group (normal subjects) a comparison between the two groups was done.
Table (1) represented the socio-demographic characteristics of the sample patients and the control group. (38%) of the samples age was between 36 and 45 years old and most of the samples were married.
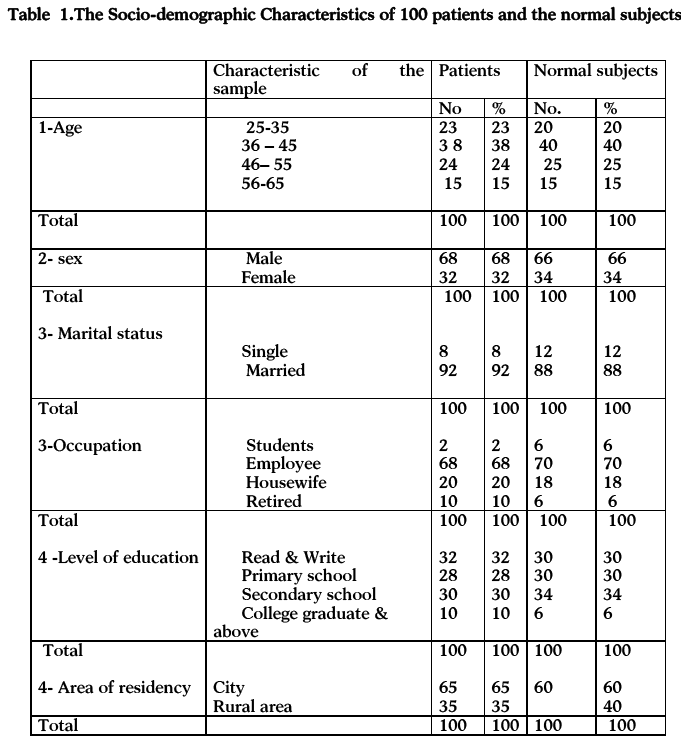
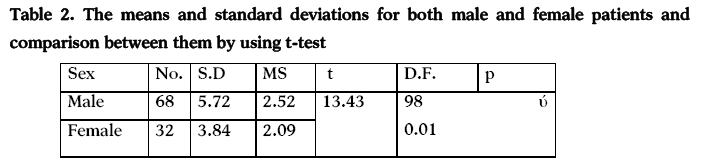
Male patients constituted (68%) of the sample and female (32%), moreover, table 2 illustrated that there was a statistical difference between the mean and the standard deviations for male and female patient p<0.01.
The highest percentage of the patients and the control group were employee and high secondary school graduation was achieved in (30%) of the patients enrolled.
Regarding the area of residency, (75%) of the sample lived in the city, while (27%) of them came from rural areas.
Table (3) declared the risk factors of stone formation related to health history in patients group and control group.There were significant differences (p‹0.01) between the two groups regarding all the risk factors except for the parathyroid disorders, however , about half of the patients were complaining from urinary tract infections.
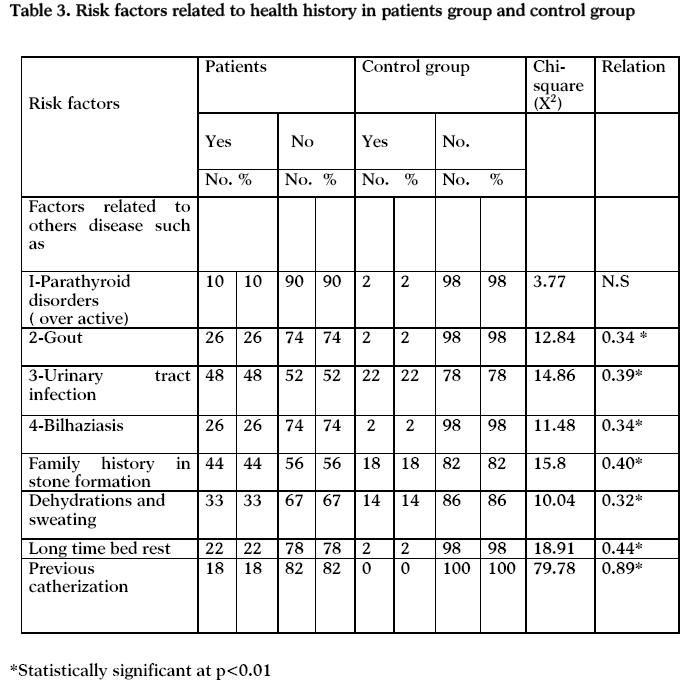
(48 %) and (44%) of them had family history of stone formation, in addition (26%) of patients had previously bilharziasis, while only (2%) of control group had the same disorders. Moreover,(26%) of those patients had gout, and( 22%)were complaining from other diseases leading them to confined in bed for along time as showed in table 3.
There were no significant differences between the two groups related to the risks factors which were displayed in table (4) except for the risk factors of taking green vegetables and taking antacids (p<0.01).
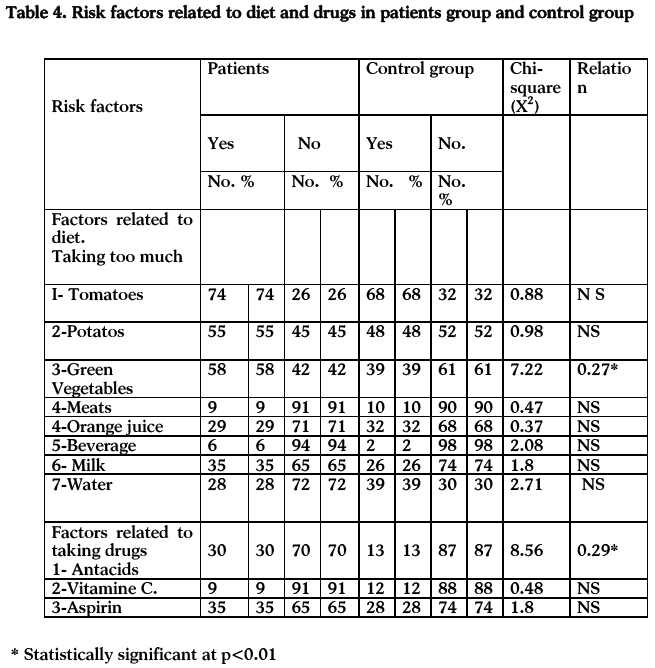
The highest percentages of patients (58%) were taking a large a mount of green vegetables in their diet, while (39%) of control group also did. However the percentage of patients who ate meat is very low (9%), and (10%) for the control group.
The current study revealed that more than half of patients enrolled in this study ate a large amount of potatoes (55%) and (75%) were taking tomatoes, while patients taking antacids were (%30) and (%13) of control group also did. Moreover, 35% of the patients receiving Aspirin tablets.
Discussion
The current study results indicated that male expose to renal stone formation than female, this finding is similar to other studies, [1,3,4] they found that most of the patients with renal stones were males. This could be due to anatomical differences in urinary tract between males and females; in male the urethra is longer than in female which may cause accumulation and stagnation of urine in the bladder for longer times.
Regarding the area of residency, the majority of sample lived in the city, while (27%) of them came from rural areas. This could be because the hospitals were in the centre of the city while the patients who lived in the rural areas may visit the health centres near them.
The present study indicated that about half of patients were complaining from urinary tract infections, this is in consistent with other studies [1,3,8,9] which mentioned that a person prone to urinary tact infection may be at risk of developing urinary calculi.
Bacteria in the urine may alter the pH level (acid –base balance) and this can trigger the formation of urinary calculi. In addition urinary tract infection disturbs the flow of fluid in the body.
The current study showed that (44%) of the patients whose relative have been afflicted with urinary calculi in comparison with control group is (18%). This finding is in agreement with other studies, which mentioned that hereditary genetic disorder could increase the risk of developing renal stone [4,5,10]. This could result in the body’s inability to properly absorb substance ,such as calcium. Consequently a build –up of calcium can lead to the formation of urinary calculi. In addition, this factor is probably one of the few factors which is not preventable [4,5,11].
Kavanagh [12] in his study about renal stone found that most of renal stones were composed of calcium oxalate (CaOx), which had commonly been attributed to the presence of high urinary oxalate output. Bilharziasis may cause bladder calcification and formation of urinary calculi. WHO report and other studies [13-16] found that people with this disease are more liable to urinary calculi than other people because female ova deposits 300 to 400 eggs a day. Those move across tissues by action of their prolytic enzymes and enter the bladder, causing severs inflammation, tissue reaction, fibroses and calcification.
The current study supports the literatures finding that there were significant differences between the patients group and the control group P < 0.01, (26%) of the patients had previously bilharziasis, while only (2%) of the control group had the same disease.
The present study indicated that (33%) of patients had dehydration due to decrease fluid intake and sweating, while (14%) of control group had the same condition, this is supported by other findings [9,10,17] which stated that low fluid intake will decrease urine output, it will concentrate urine and allow solutes to precipitate and during summer the body lose a lot of fluid through perspiration and urine output decrease. This will increase the possibility of developing urinary calculi. Moreover, rise in the urine concentration, typically occurring in the hot climate, speeds up the process of crystal growth and increases the chance for urinary calculi formation. Gout is a medical condition that can affect the normal balance and increase in uric acid secretion and may be a risk of urinary calculi [4-6]. In the current study (26%) of patients had Gout, while only (2%) of the control group had the same disease.
Okada et al., [18] mentioned in their study that Long-term bed-rest induced renal stone formation. In addition, other various studies found that complete bed rest for long time and reduction of physical activity may be a risk factor for urinary calculi formation, [1,16,17] the present study is in agreement with those previous studies,(22%) of the sample patients were complaining from other diseases leading them to confine in bed for a long time, while (2%) of control group had the same condition.
Dalton19 Khanna et al., [20] ,Ja Heon et al., [21] reported that many patients developed urinary calculi after the insertion of a Foley catheter. The presence of a foreign body within the urinary tract can develop urinary calculi even in the absence of infection, they concluded that renal stone is more common in patients with urethral catheterization than for those voiding spontaneously, in the present study (18%) of the sample patients were previously catheterized ,this finding is consistent with the results of the previous studies More than half of the sample patients were taking a large a mount of green vegetables in their diet and very low (9%) ate meat , although a diet high in animal protein affects certain minerals in the urine, that may promote the formation of renal stone [1,2,9].
Many studies found those who ate the most animal protein had a 33 percent higher risk of developing urinary calculi [1,2,22]. However, most of the people in Iraq prefer to eat vegetables and beans because they are cheaper than meat.
Vegetables contain a large a mount of oxalate which may cause renal stone. This result is supported by other literatures which mentioned that oxalate should be restricted in people who are at risk of urinary calculi formation [1,3,6].
The current study revealed that (30%) of the patients were taking antacids, while (13%) of control group also did. This is in agreement with other studies who mentioned that there is evidence that certain types of medication may increase the risk of developing urinary calculi [1,2,5,16]. Moreover, (35) percent of the patients were receiving Aspirin tablets this is in consistent with other literatures [1-3,16] who mentioned that this drug may increase the likelihood of stone formation.
Conclusions
A field study was carried out on (100) patients diagnosed with urinary calculi and admitted to Medical City and Al-Karama hospitals in Baghdad in order to find out the risk factors of this disease and to find out if there were statistical significant differences between the variables. In order to find out whether these risk factors were unique for those patients, (100) normal subjects were chosen as a control group.
A questionnaire format was designed and included (19) items and data were gathered through patient's interview.
Frequency, percentage and chi-square and t test were used as statistical measures to analyze the data.
Results showed that (9) out of (20) items were significant (p<0.01) , there were significant relations between renal calculi and risk factors, such as( Gout, dehydration, Bilharziasis, genetics factors, bed rest, urinary catheter, taking antacids tablets and vegetables).
The application of t –test indicated that there was a significant relationship between risk factors of renal stone and sex of the patients. According to the result of this study, the researcher recommends the following:
1.Teach people to avoid those risk factors which may help in developing urinary calculi.
2.Change Lifestyle through encouraging people to drink quite a lot of fluid because fluids hinder the formation of calculi by diluting the urine especially in hot climate (Such as Iraq) which causes increased a mount of perspiration and loss of fluid.
3.Avoid taking too much vegetables and drugs that cause urinary calculi e.g. antacids and aspirin because dietary adjustments help in preventing the development and the recurrence of the calculi.
4.Advise people who are prone to stone formation to cut back foods with high calcium and animal protein.
5.Encourage people with bilharziasis to treat the disease and take the drugs regularly as prescribed to avoid bladder calcification and others complications.
Acknowledgment
The author wish to acknowledge Dr.Nibras Abdul Hadi for helping in the revision of the manuscript in English Language.
3124
References
- Bihl G, Meyers A. Recurrent renal stone disease--advances in Pathogenesis and clinical management. Lancet. 2001; 358 (9282): 651-6.
- http//www.Harvard health publication.com.2010.. Kidney stones –Risk factors.
- http//www. About-Com .Heath Topics A-Z .Kidney Stones 2010 Adam.about.com/reports/000081-7.htm.
- DevuystO.Pirson Y. Genetics of hypercalciuric stone forming diseases. Kidney International.2007; 72 (9): 1065-72.
- Prié D, Friedlander G. Genetic Causes of Renal Lithiasis.International Bone & Mineral Society (IBMS). 2009; 357-67.
- Abdel Goad EH, Bereczky ZB. Metabolic risk factors in patients with renal stones in KwaZulu Natal: an inter-racial study (Asian and Whites). BJU Int. 2004;93(1):120-3.
- Aron HC, Chris P. OA Reversible renal impairment caused bythyroid disease.Scandinavian Journal of Urology and Nephrology. 2010;44:3:190-93.
- Costa Bauza A, Isern BP. Factors affecting the regrowth of renal stones in vitro: A contribution to the understanding of renal stone development .Scandinavian Journal of Urology and Nephrology .2005;39:( 3):194.
- Chris. Kidney stone causes and Risk Factors. Home /Current Health Articles. www health centre .com 2010.
- Smeltzer SC, Bare BG, Hinkle JL. and Cheever K.H . Management of patients with urinary disorders. Textbook of Medical-Surgical Nursing12th ed. Lippincott Williams and Wilkins. 2010 ;1375-80.
- kavanaghJ.Super saturation and Renal precipitation. Urologic research. 2006; 34(2):81-5.
- The Carter Centre Schistosomiasis Control Program.http:/www, Carter Centre. Org/health/Schistosomiasis/index.html.retrived.2008; 07-17.
- Lukacs DFA. El-seaghy and Pajor L. Multiple Urolithiasis in BilharziasisPatient.InternationalUorology and Nephrology. 1989; 21 (3).269-73
- Elderdery A, Altoum M, Ahmed B, Abelgalil, H.B. Schistosomiasis in Sudan and Beyond.Uorologic Cancer. 2008; 3(4)18-20.
- Bilhariziasis in Iraq by Al-Yarmok –University Students mht-Iraqi Youth-Bilharziasis=\;mhtml;file;//F. 2010 accessed 8/4/2010.
- Amiel J. Choong S. Renal Stone Disease: The Urological Perspective. Nephron ClinPract . 2004; 98: 54-58.
- Okada A, Ohshima H, YasunoriItoh, Yasui K, Tozawa, K, Kohri K. Risk of renal stone formation induced by long-term bed rest could be decreased by premeditation with bisphosphonate and increased by resistive exercise. International Journal of Urology. 2008; 15: 630-35.
- Dalton DL, Hughes J Glenn J.E. Foreign bodies and Urinary stones. Uorology. 19990; l6: 1.
- Agarwal MM, Singh SK, Mavuduru R, Mandal AK. Preventive fluid and dietary therapy for urolithiasis: An appraisal of strength, controversies andlacunae of current literature. Indian Journal of Urology 2011;27:310-9.
- Khanna R, Gupta SK, Madhusoodanan P, Sandhu AS, Sinha T, Kumar A, et al.An Iatrogenic secondary urolithiasis: A case reportIndian J Urol .2004 cited 2010 ;20:187-8.Available from: https://www. In dianjurol.com/text.
- Hyeon JK, Tae YL, Jeong KP, Won HS, Hong B. Risk factors for urinary stone formation in men with spinal cord injury: a 17-year follow-up study. BJU International. 2006; 97 (4) 790-93.

