Background
Approximately 1.2 billion adolescents (aged 10−19 years old) make up 18 percent of the world’s population [1]. More than half of all adolescents live in Asia which is nearly one fifth of the world’s population [1]. Adolescents, a vulnerable populations have multiple sexual and reproductive health problems including gender inequality, sexual coercion, early marriage, polygamy, female genital mutilation, unplanned pregnancies, closely spaced pregnancies, abortion, sexually transmitted infections (STIs) including HIV/AIDS. Lack of access to appropriate health care and access to information and communication are the most important factors hindering their health care [2].
Information and communication technology (ICTs) in response to the health concerns was discoursed as far back as 1994 (two decades ago). In 2008, the International Telecommunication Union identified and published way for the use of ICT in public health with the extension of new technology and the exploration of existing standpoints for revolutionary applications. The arena of ICT is now transforming the field of public health [3,4]. Telemedicine, use of ICTs to provide health care where people did not have access to health services tries to address health challenges in several countries of Asia [5]. ICTs, aid in collective efforts to create a dependable and reliable health care and health information system, of good quality and it promotes continuous medical training, education, and research [6,7].
Adolescents are also becoming the leading subscribers of mobile phones and users of computers mainly for social networking and sexual health information that is easily accessible, trustworthy, credible, confidential and non-threatening. The profile of Internet usage is similar to that of mobile phone usage. Young people’s use of social media such as Facebook, Orkut in Brazil and India, RenRen in China and VK in the Russian Federation have grown exponentially over the past few years [8].
Aim
This review article was intended to assess and document the existing policy papers, official guidelines, research articles and survey reports on ICT use in adolescent sexual and reproductive health programs, altogether with exploring potential opportunities for improvement of adolescent health services through ICT in selected south Asian countries.
Methodology
A systematic search of published literature comprising research articles, program and policy reports were reviewed. Desk review of the published papers, reports and policies from the selected countries such as India (largest adolescent population in the world), Nepal (effective response to HIV and reproductive health issues), Afghanistan (conflict affected country), and Srilanka (ideal public health system). Male and female adolescents aged 10-19 years who were married or single were included in this study.
Literature search strategy was developed by the research team and critiqued by experts. The following search engines were used to retrieve policies and program on adolescent sexual and reproductive health from the official web portal of selected countries. Google and Google scholar search engines were used to locate particular website containing information on ASRH. Additional searches were conducted to retrieve studies published between 1990 and 2013 using PubMed, Google Scholar and Medline. Other review articles and articles written by prominent authors on ICT use in ASRH were also considered for citations.
An eligibility criterion was literature published in English, targeting male and female adolescents, aged 10-19 years irrespective of their marital status. The documents which mentioned information on ASRH, ICT use were included. In addition to this, those documents which have repetition of the similar information were excluded. Only studies in English were included in this systematic review. In the beginning, altogether 86 documents articles were gathered among them 42 were government and non-government policy papers and strategy documents and 23 were guidelines related to ASRH, 10 were journal articles and 11 were survey reports. Indepth study of the all articles were done and sorted out as per the inclusion criteria. 59 documents were excluded because they did not meet our inclusion criteria. Finally, 27 national documents, journal articles, survey reports and guidelines were selected which was published up-to 2013 (Figure 1). Major key words used were Information, Communication, Technology, Adolescent and Sexual Reproductive Health, Nepal, India, Srilanka, Afghanistan , Strategy, South Asia, Situation, and Mobile Use.
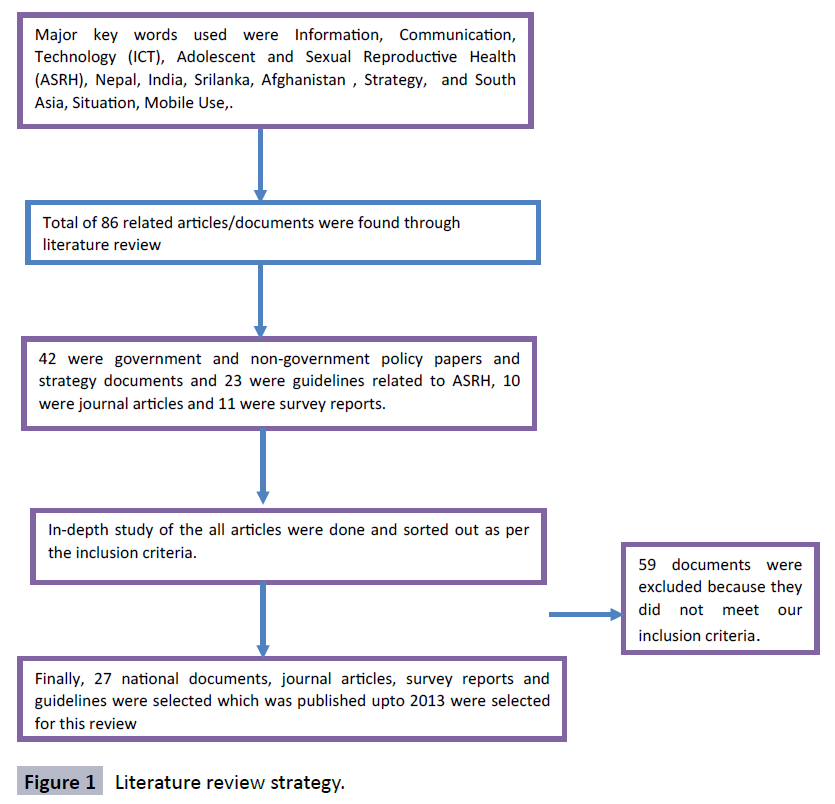
Figure 1: Literature review strategy.
All the available versions of policy, program and reports on ASRH from selected countries were assessed by research team and all the relevant information were extracted for review.
Results
Afghanistan has been politically unstable and at war for more than two decades. Documentation has often been difficult to obtain on health related matters. In case of India, it’s one fifth (22%) of the total population belongs to adolescent age group. However, data on adolescents from national surveys including NFHS III, shows that adolescent have limited awareness about sexual and reproductive health matters [9]. The current status of Nepal in terms of adolescent reproductive health is not very perfect due to dearth of crucial information. Sri Lanka has made considerable progress in addressing adolescent health as compared to India, Nepal and Afghanistan. Adolescents (10-19 years of age) constitute about 15% of the total population of Sri Lanka. A current estimate places nearly 3.9 million adolescents in this age group [10]. However, there is a gap in addressing sexual and reproductive health of this age group. Information on reproductive health services is still lagging in Sri Lanka (Table 1).
Table 1: Policies, Plan, and Strategies in Relation to ASRH.
| Countries |
Policies, plans and Strategies |
| Afghanistan |
•Safe Motherhood Initiative Policy, 1997
•National Child and Adolescent Health Strategy 2009 - 2013
•National Policy and Strategy for Nursing and Midwifery Services, 2010
•Strategic Plan for the Ministry of Public Health (MoPH) 2011-15
•National Reproductive Health Strategy, 2012-2016
•National Youth Policy – draft July, 2013
Major focus on :
•Reduction of early marriages of girls and adolescent pregnancies (figure not specified)
•Importance of personal hygiene and cleanliness
•Need for regular physical exercise
•Raise awareness on the danger of substance abuse |
| India |
•The National Youth Policy (2003) visualizes active participation of youth, including adolescents, at all levels of social enterprise. It recommends youth empowerment through education, nutrition, leadership development and equal opportunity.
•The National Health Policy (2002) has recognized the nutritional needs of adolescent girls as well as the necessity of implementing school health programs.
•The National Population Policy (2000) and the National Policy for the Empowerment of Women (2001) both recognize adolescents as an underserved and vulnerable population group with special sexual and reproductive health needs.
•The National AIDS Prevention and Control Policy (2000) recognize street children and sex workers as vulnerable groups and recommend the inclusion of HIV/AIDS issues in population education.
•The National Policy on Education (1986, modified in 1992) aims to equalize education opportunities in the 15–35 years age group, implement free and compulsory elementary education for all children up to 14 years and imparts functional literacy to adult illiterates. It recognizes the role of adolescents in population stabilization and parenthood.
•A strategic approach to reproductive, maternal, newborn, child and adolescent health (RMNCH+A) in India (2012-2017)
•Reduce anemia in adolescent girls and boys (15–19 years) at annual rate of 6% from the baseline of 56% and 30%, respectively [25].
•Decrease the proportion of total fertility contributed by adolescents (15–19 years) at annual rate of 3.8% per year from the baseline of 16% [25].
•The National Adolescent Reproductive and Sexual Health strategy (ARSH) under broader umbrella of Reproductive and Child Health-II (RCH-II), National Rural Health Mission (NRHM), incorporates a core package of services including preventive, promotive, curative and counseling services. It involves |
| Nepal |
•National Health Policy 1991 [26].
•Second Long Term Health Plan 1997-2017
•Safe Motherhood Policy 1998
•Directives on Safe Abortion 2002
•National Adolescent Health and Development Strategy 2002
•National Skilled Birth Attendant Policy 2006
•Nepal Health Sector Program II [27]. |
| Sri Lanka |
•National Health Policy, 1996 has identified adolescent health as one of the priority area to focus on.
•The population and reproductive health policy and action plan was formulated in 1998
•National youth policy in draft
•National Policy and Strategy on Health of the Young, 2010 addressed health of adolescent and young population.
•The National eHealth Policy of Sri Lanka is aimed at guiding the implementation of Information and Communication Technology solutions for all age groups including adolescents in the health care sector.
•National HIV/AIDS Policy (2011)
•National Maternal and Child Health Policy (2008)
•National Strategic Plan on Adolescent Health (2009)
•Adolescent Sexual & Reproductive Health & Rights Policy (2006)
•National Labor Migration Policy for Sri Lanka (2008) |
Access to ICT and Challenges of ASRH program
Afghanistan
Data specific to adolescents is difficult to obtain. Country wide in 2013, there are 2.4 million users of the internet in Afghanistan. Telecommunications covers 88% of the population (https:// mcit.gov.af/en). In 2010, UNICEF estimated that approximately 41.39/100 people in Afghanistan owned a mobile phone (https:// www.unicef.org/infobycountry/afghanistan_statistics.html).
Financial barriers
Out of pocket (OOP) expenditure on health as % of total health expenditure is almost 90% in Afghanistan [11]. To overcome this barrier the National Health Policy of 2012-2020 was generated which proposes universal package of health services with subsidy to the poor.
Supply-side barriers influencing availability of services
These include availability of personnel in recommended WHO ratio of 23physicians/10,000 population [12], legalized abortion services and availability of reproductive health commodities. Government of Afghanistan has trained 810 peer youth educators, set up 24 youth-friendly Adolescent Reproductive and Sexual Health centers and deployed 66 community midwives. This was a collaborative effort with USAID, JICA and Afghan Society of Obstetrics and Gynaecology (UNFPA, 2011)
Demand side barriers
Investment and action needed in increasing health system responsiveness to gender-based inequalities.
Proposed suggestions include
• Organizing services at times and locations that are convenient to women
• Ensuring visual and auditory privacy and confidentiality
• Integrating services – for example maternal health and family planning with HIV/AIDS
• According greater autonomy to women seeking health care [10].
India
India is the second-largest mobile phone user with over 900 million users in the world. It accounted for over 10% of the world’s online population in 2011. Government of India has recognized the potential of mobile cellular subscriptions to reach adolescents through IT enabled systems and mobile based information dissemination programs [13]. It also has the world's third-largest Internet user-base with over 137 million as of June 2012 [14]. A cross-sectional survey conducted in Kolkata has showed that substantial numbers of adolescent girls have seen the advertisements on hand washing and Government’s scheme on institutional delivery [15].
Reaching the huge population of adolescent group within diverse geographic locations with existing limited resources is the crucial and important challenge in front of government of India. However these challenges can be clubbed as below-
• Convergence and Intersectoral coordination- An active participation from key stakeholders beyond the health sector such as education, social welfare, different ministries and use of existing common platforms are crucial for implementing this preventive and progressive adolescent health strategy. Convergence among various programs within Ministry of Health and Family Welfare [13], including the existing adolescent health strategy, school health, adolescent education program (AEP) of NACO, mental health and anemia control initiatives, schemes of Ministry of Women and Child Development, Ministry of Youth and Sports Affairs, Ministry of Information and telecommunication as well as Ministry of Human Resource Development can prove helpful in providing comprehensive services to this age group.
• Geographic diversity- considering the diverse geographic background of India, it is always difficult to reach hard to reach areas such as hilly region, remote villages, northeastern states.
• Infrastructure- Strengthening health facilities to deliver adolescent friendly health services is always costly. Budgetary constraints for such new constructions or renovations restrict the expansion of program.
Nepal
Majority of adolescents had no personal mobile phone, with less than one third (32.0%) of all female respondents possessing a mobile phone, but more than half of all male respondents (57.3%) having one. Most respondents did not have a laptop/ computer, internet access or a motorbike. Overall, males were more likely to report having a laptop or PC (personal computer) in the house than females (11.0% versus 7.8%). Although overall internet access at home was low, men were twice as likely to have such access (male 8.6%; female 3.7%) [16].
Though the government has imparted for action to address the need of adolescent, however, challenges do exist. These challenges can be summarized into following headings:
• Future of the ASRH program envisioned: At least 1000 health facility needs to be strengthened to provide adolescent friendly service within 3 years. This demand for huge amount of resources.
• A variety of activities need to be provided to cater for the services, which might be constrained due to logistics and skills.
• Capacity Development: As a new area of service, the service providers need to know the essence of the “specialized” services. So, the capacity of the health workers needs to be enhanced within a short period of time.
• Acceptance by the community: Adolescent reproductive health is relatively new phenomenon and so, the community needs to understand and accept it. The existing socio cultural norms and practices might influence to the success of the program.
Srilanka
In 2006, there were 280,000 internet users, approximately 14% of total population of Sri Lanka [17]. Around 88% adolescent females had access to mass media in 2002-2011. There were 87 mobile users and 15 internet users per 100 populations in 2011 (UNICEF). There is a comprehensive e-government strategy to enable government to effectively utilize ICT opportunities, and allow citizens to benefit from the global information economy [18].
Sri Lanka has made considerable progress towards addressing the Millennium Development Goals, however, there are still gaps reflected in adolescent health and social indicators and in the delivery of services.
• Low adolescent sexual and reproductive health knowledge: Only 57% of adolescents knew that condoms can reduce the risk of transmission of sexually transmitted infections (STIs) while even less (18%) have this knowledge in the estate sector (plantation areas that are largely privatized) [19]. Three quarters of females and two thirds of males 10- 14 yrs report low levels of sexual knowledge [20].
• Rising teen pregnancy: While there has been a decline in the adolescent fertility rate from 35 per 1000 live births among women aged 15-19 in 1993 to 27 in 2000, in 2006/07 it has again increased to 28. The adolescent fertility rate for the estate sector in 2006/07 was 37/1000 [19].
• High rates of sexual abuse: Nearly 10% of early adolescents and 14% of mid and late adolescents school enrolment [21].
• Increasing demand for adolescent sexual and reproductive health (ASRH) information: Enrolments in schools are increasing in Sri Lanka as participation in the labour force for 15-19 year olds is declining [22]. This means that secondary teachers who have been identified as a key source of ASRH information [23] are facing an increasing demand for ASRH education.
• Failure of youth specific service centres trials such as the youth corner in hospitals: Adolescents in Sri Lanka have poor knowledge and utilisation of existing adolescent specific health services [24].
• Abortion: Illegal, unsafe, on the rise (150,000-175,000 performed annually)
• HIV/AIDS: On the rise, poor awareness among high risk groups (i.e. workers in free trade zones, in tourist industry, commercial sex workers, displaced persons)
Discussion
Adolescent health has been a priority for the entire public health fraternity for many years, and many of the governments have included it in their flagship national programs. A holistic approach assimilated through the Adolescent Reproductive and Sexual Health (ARSH) Strategy to meet unique needs of adolescents through delivering comprehensive package of health services, creating adolescent friendly environment at facilities and building mass awareness within communities with more attentive service providers.
Indeed, many other publications, reports, strategies and program documents of selected countries on adolescent health and ICT opportunities might have been missed through this exploratory review. Nevertheless, this systematic review suggest that in the south Asian context, in contrast to the general population, data on adolescent access to and use of ICT in practicing sexual and reproductive health services are minimal, and criteria and definitions that would aid data analysis and comparison across countries are lacking. Though almost all the selected countries have recognized the importance of adolescent health and have incorporated it in policies, program and strategic planning.
Numerous factors such as social exposure, economic dependency on parents, peer pressure, minimal access and limited knowledge about contraceptives, social norms for early marriages and childbearing, limited decision making power and less access to resources are interplaying role on adolescent’s sexual and reproductive health. However it has been widely evident that adolescents are large users of mobile phone, internet and related technologies to gain knowledge of many things. Thus, it became clear from the literature review that it would also be important to review the use of m & e-technologies. With the growing penetration of internet and smart phones and the rapid development of communication technologies, there has been increasing attention paid to the use of mobile phones for health (mHealth) and internet for e-health, including for a number of the functions that ASRH has been designed to fulfil, such as reminding [25-28] (e.g. about vaccination schedules), informing, providing health messages [29] contributing to behavior change and improving patient care [30].
ICT have a number of potential advantages over conventional system, for example they can be personalized and interactive, they are convenient and they blend with the lifestyles of many adolescents, even in LMICs, and reminders (for appointments, safe sexual practices, vaccines, follow up) can be sent in real time as needed, anticipating adolescents can make use of health services of their own choice at the right time. It may be reflective of a number of factors, including the relative lack of attention that has been paid either to the provision of ICT use for health services of adolescents or to the monitoring of milestones that have important implications for adolescent health and development, and transitions to adulthood.
There are clearly important opportunities for using mobile phone and internet based-technologies, and although the current focus and practice builds on paper/card, the future potential is likely to be something mobile, digital and alive, that can seamlessly connect adolescents with various providers, whether school- or health system-based.
Conclusion and Recommendations
Worldwide, access to ICT has improved for the general population. However, data on adolescent access to and use of ICTs are minimal, and criteria and definitions that would aid data analysis and comparison across countries are lacking. Overall, the available data suggest that Internet use is more likely with higher income and education, and more men than women use the technology in both industrialized and developing countries. Data also indicate a deep urban/rural divide, with urban dwellers more likely to log on. Internet use is also more common among people who are currently in school.
ICT platforms should be applied to scale-up policies and programs that promote the sexual and reproductive health of adolescents due to their low cost, increased access to remote populations, better efficiency and improved flexibility for programming. Effective models should be recognized through programme evaluation. The explosions of electronic technologies like the availability of internet either at home or school and the wide use of mobile phones are new opportunities to provide sexual health communication to adolescents. ICTs can enable access to information, foster the expression of ideas on a large scale and help adolescents connect with others; but it carries such risks as exposure to inappropriate content, unwelcome contact from others or the possibility of engaging in inappropriate conduct themselves.
Key recommendations to address ASRH service and information delivery issues are:
• Establish clear policy on adolescent sexual and reproductive health across the ministries of health, education and youth affairs and integrate with them
• Establish a responsible media policy in ASRH
• Develop an inter-sectoral approach to delivery of services across the health and education sectors
• Develop guidelines, regular reporting mechanisms and indicators for continuous quality improvement across both the health and education sectors.
6881
References
- UNFP (2011) World Population Prospects The 2010 Revision. Volume I: comprehensive tables. Department of Economic and Social Affairs, United Nations
- United Nations Population Fund (2008) Reproductive health and sexual and reproductive health framework. United Nations
- NFSD, ITU (2011) Summary of Geneva Dialogue. mhealth: Using mobile technology to advance public health in the developing world
- Déglise C, Suggs SL, Odermatt P (2012) Short message service (SMS) applications for disease prevention in developing countries. Journal of Medical Internet Research 14: e3
- Wootton R, Patil NG, Scott RE, Ho K (2009) Telehealth in the Developing World. Ottawa, Canada & United Kingdom (UK): International Development Research Centre
- von Ungern-Sternberg S, Lindquist MG (1995) Brief Communication. The Impact of Electronic Journals on Library Functions. Journal of Information Science 21: 396-401
- Gomez EA, Wu D, Passerini K (2010) Computer-supported team-based learning: The impact of motivation, enjoyment and team contributions on learning outcomes. Computers and Education 55: 378-390
- Livingstone S, Leslie (2012) EU Kids Online II: enhancing knowledge regarding European childrens use, risk and safety online. The London School of Economics and Political Science, London, UK
- Ram U, Mohanty SK, Singh A, Ram F, Santhya KG, et al. (2010) Youth in India: Situation and Needs 2006-2007, Andhra Pradesh. Mumbai. International Institute for Population Sciences, Mumbai
- UNFPA (2011) UNFPA Afghanistan: Recent Accomplishments in Reproductive Health
- Steinhardt LC, Waters H, Rao KD, Naeem AJ, Hansen P, et al. (2009) The effect of wealth status on care seeking and health expenditures in Afghanistan. Health Policy Plan 24: 1-17
- WHO (2006) The world health report 2006: Working together for Health. WHO, Geneva
- Press Information Bureau (2012) India is the Second-Largest Mobile Phone user in World. Ministry of Health and Family Welfare, Government of India
- Miniwatts Marketing Group (2012) Internet World Stats- Internet Usage in Asia 2012
- Ray S, Dasgupta A (2013) Information and communication technologies used by adolescents of today: an opportunity or curse? Int J Biol Med Res 4: 3169-3180
- Simkhada P, van Teijlingen E, Acharya DR, Schildbach E, Silwal PR, et al. (2012) Sexual and reproductive health of adolescents in rural Nepal: knowledge, attitudes and behavior. Nepal Population Journal 17: 3-10
- Central Intelligence Agency (2014) The World Factbook 2007, United States of America
- Perera Y (2013) User friendly state through e-Government. Proceedings of the Daily Mirror Online: Financial Times
- Department of Census and Statistics, Ministry of Healthcare and Nutrition (2009) Sri Lanka Demographic and Health Survey 2006-07. Colombo, Sri Lanka
- Silva WD, Karunathilake K, Perera R (2009) Patterns of sexual vulnerability among adolescents and youths in Sri Lanka. Asian Population Studies 5: 41-59
- Sunethra, P, Jampaklay, A (2011) International migration and children left behind: Impacts on children’s school enrolment in Sri Lanka. Sri Lanka Journal of Population Studies 12-13.
- Yakandawala YLH (2007) Knowledge Attitudes and Practices of Girl Guides in Selected Districts on Sexual and Reproductive Health Including Sexually Transmitted Diseases and HIV/AIDS. Family Planning Association of Sri Lanka Colombo.
- Agampodi SB, Agampodi TC, Piyaseeli UKD (2008) Adolescents’ perception of reproductive health care services in Sri Lanka. BMC Health Serv Res 8: 98
- International Institute for Population Sciences, Macro International (2007) National Family Health Survey (NFHS-3), 2005-06: India: Volume I. Mumbai: IIPS
- Ministry of Health, Population- Government of Nepal (1991) National Health Policy 1991
- Ministry of Health, Population- Government of Nepal (2010) Nepal Health Sector Programme Plan II (NHSP-2) 2010-2015
- Kharbanda EO, Stockwell MS, Fox HW, Rickert VI (2009) Text4Health: a qualitative evaluation of parental readiness for text message immunization reminders, Am J Public Health 99: 2176-2178
- Gurman TA, Rubin SE and Roess AA (2012) Effectiveness of mHealth Behaviour Change Communication Interventions in Developing Countries: a Systematic Review of the Literature, J Health Commun 17: 82-104
- L’Engle K, Vadhat H (2009) Mobile Phone Interventions for Reproductive Health (M4RH): Testing the Feasibility of Text Messaging to Improve Family Planning, Progress in Family Planning, FHI.

