Keywords
Children, adolescent, cancer, treatment, self esteem, self concept, body image.
Introduction
Cancer in childhood remains the second cause of death after accidents, despite the significant progress reported in the understanding of the pathogenesis and efficiency of treatment [1,2]. The goal of the treatment applied nowadays for childhood cancer is not only to increase the survival rate, but also to improve the quality of life of these children [3-6].
The severe bodily disease has unquestionable consequences on each phase of the child’s development by hindering or disturbing its normal evolution [7].
Cancer is frequently experienced by children as a violent internal and external attack. Daily routine is disrupted, complications occur, painful medical interventions are experienced, repeated admissions to hospital take place and there are frequent separations from their beloved ones, their social environment and school [8]. All the above contribute to the incidence of psychological reactions such as depression, anxiety, reduction of self?esteem and distortion of their body image [9-13].
Body image, especially self?concept, is a crucial determinant of behaviour [14]. The changes happening to the body during childhood, especially in puberty, and the personal attitude towards these changes have an immediate effect on the social adjustment of the child and adolescent [15,16,19]. The child with a severe bodily disease experiences a threat to body image, either from the illness itself or from the medical and nursing interventions [17]. Especially, chronic diseases, such as cancer, hinder the normal development of self?image in its emotional, intellectual and social dimension [18,20,21,23,24].
Despite the fact that each child reacts to the disease and the applied therapy in a unique way, studies have shown that certain factors such as age and gender affect children’s, and especially adolescents’ self?concept to a higher degree [22].
The stress that stems from body changes ?because of the disease? as well as from the emotional and social reactions of the family and other significant people, leads to a reduction in the child’s selfesteem, particularly in adolescents, and to retrogression to less mature behaviour and school performance as a means of defence against this condition.
The normal adjustment of the child and adolescent to the disease and to the consequences of the treatment depends on the way the disease is dealt with, by the people taking care of the child/adolescent.
Purposes of the study
1. To define the self?concept of children with cancer in comparison with healthy children and children with thalassaemia. In particular to study the self?concept in relation to factors such as: a) physical appearance, b) behaviour, c) anxiety, d) intellectual and academic level, e) happiness and satisfaction.
2. To define the extent to which certain demographic factors (gender, age, family situation) affect the self?concept of children with cancer.
Material and Method
Study Population
The study comprised of 165 ill children and adolescents, who were treated for various forms and stages of cancer at two of the largest paediatric hospitals in Athens – ‘Pan. and Agia Kyriakou’ and ‘Agia. Sophia’. Furthermore, two groups of children comprised the control patients: (a) 212 children with thalassaemia arriving at both hospitals for blood transfusion and (b) 417 healthy children of respective age of the children suffering from cancer. The healthy children, in their majority were from the 2nd senior and 5th junior high schools of Heraclion, Attica, and from the 53rd primary school of Athens, as well as from various other areas.
The criteria set for the election of the sample as well as for the control group were the following:
• The children and adolescents must be between the age of eight (8) and eighteen (18), of both sex and with some form of cancer.
• The children and adolescents must be informed about the study and the methodology to be used that is the interview before it takes place.
• There must be both parent/guardian and child’s consent.
• Children with a body handicap or that are mentally retarded must be excluded.
• Children and adolescents whose mother tongue is not Greek must be excluded.
• Children who are unable or unwilling to cooperate in order to fill in the questionnaire must be excluded from the sample.
• The interview time must not exceed that of twenty minutes.
• The children should answer all questions.
All children in the study population as well as the children with thalassaemia fulfilled the above study criteria and were included in the sample. Only two children of the healthy controls aged eleven and eighteen years old, answered the questions selectively and were excluded from the study.
Methodology
The collection of information was undertaken by only one researcher of the group interviewing both the children of the study and the children used as controls.
Each child of the sample and of the controls answered with a yes or no to the eighty questions of the Piers?Harris scale [25].
The Piers?Harris Children’s Self?concept scale sub?titled ‘How do I feel about myself’ is a brief means of self assessment which was created in order to help evaluate the meaning of ‘I’ in children and adolescents. The data on the scale are marked in a positive or negative wording so as to show the dimension of this self?evaluation. The scale comprises of eighty (80) questions. This scale can be given to individuals or to groups. A number of sentences which state how various people feel about themselves are given to the children and they are then asked to mark with a yes or no whether these sentences relate or not to how they feel about themselves.
The Piers ?Harris scale measures the attitudes of evaluation and the child’s behaviour. The main purpose of the scale is usually to give a global index of self?concept, but it can also be used as a means of promoting formulation of hypotheses and wider fields of clinical research.
More specifically, this scale checks whether the self?concept of the child is negative or positive. In addition, it provides the ability to measure the following factors: behaviour, intellectual and academic level, physical appearance, anxiety, popularity, happiness and satisfaction.
In the present study, the scale was given to 417 healthy children and further analysis of the factors took place. Hence, it was found, according to the answers of the children, that the scale utilised in Greek children provides the capability to measure only five factors, i.e. all except popularity, as the questions of the scale concerning the factor of popularity were included in the remaining five factors. The analysis took place with five factors instead of the six factors of the scale that Piers?Harris proposes.
To ensure confidentiality, the interviewing of sick children took place in a special office. Parents were excluded from the procedure. The duration of the interview was 20 to 30 minutes. The majority of older children answered within 20 minutes. During the interview, the researcher observed any possible changes to the external image of the body (e.g. alopecia) stemming from the sickness or therapeutic mode and took special notes regardless of whether the child understood this change or not.
The ethical principles ruling every social research were strictly maintained, thus all the children’s answers were treated as confidential, even from informing the parents. In addition, for the implementation of this study, permission was granted by the ethics committee of both pediatric hospitals, as well as by the Ministry of Education regarding the healthy controls.
Statistical Analysis of the Data
For the processing of the data, the following statistical methods were used:
A. Factor Analysis [26].
B. Discriminant Analysis [27].
C. Analysis of the variability, for the comparison of the mean values and the standard deviations of the two distributions [28].
D. The Student ‘t?test’ for the comparison of the mean values of the two distributions [28].
E. The linear multiple regression method [28].
Results
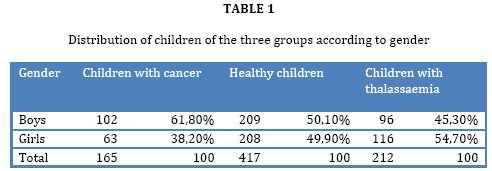
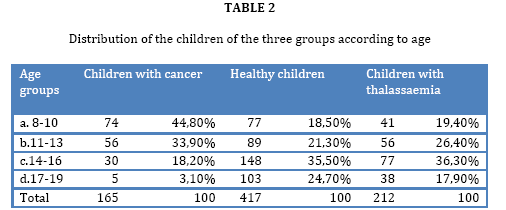
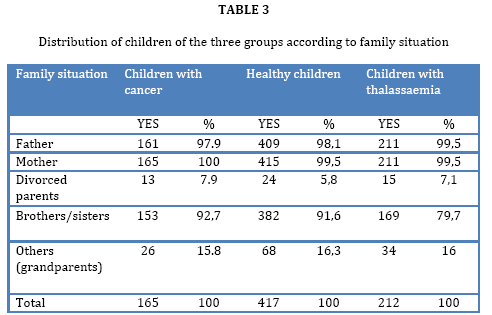
The general characteristics of the children of all three groups participating in the study are shown in tables 1, 2, 3.
From the clinical characteristics of the sick children, the following were found:
Regarding the type of cancer, leukemia was in the first place, with 83 children (50.3%) suffering from acute lymphoblastic leukemia. 46 children (27.9%) presented with lymphomas and in order of frequency followed 19 children (11.5%) with sarcomas, 10 children (6.1%) with neuroblastoma, 4 patients (2.4%) with brain tumors and 3 patients (1.8%) with nephroblastoma.
Concerning the stage of disease, 104 children (63%) were, during the collection of information, undergoing treatment. 21 children (12.7%) were in relapse and 40 children (24.2%) were in remission or recovery.
The distribution of the sick children according to the existence of obvious external change, by evaluation of the researcher, was that 95 children (57.6%) had undergone a change in their external body image and 75 children (42.4%) had not.
The factors studied were five: Physical appearance, Behaviour, Anxiety, Intellectual and Academic level as well as Happiness and Satisfaction. The results that arose after the statistical analysis with those of the method of multiple regressions by sex, family status and age group as independent variables showed the following:
I. Appearance
The analysis of data concerning appearance did not show anything of statistical significance for children with cancer in relation to their demographic characteristics. On the contrary, among the healthy controls it was found that children aged 8?13 years old believe that they have a better appearance (P<0.001), the same is believed by children of the same age with thalassaemia (P=0.038), whereas children of the same group aged 17?19 years old believe they have a bad appearance (P=0.003).
II. Behaviour
As far as behaviour is concerned, girls, children who have a father and children aged 14?16 years old, of the study population, believe that their behaviour is good in a significant proportion (p=0.013, p=0.013 and p=0.008) respectively. From the healthy controls, girls (P=0.006), and children aged 8?13 years old (P<0.001) think their behaviour is good, whereas children of divorced parents (P=0.039) think their behaviour is bad. From the controls with thalassaemia, girls think their behaviour is better (P=0.003).
III. Anxiety
It was found that girls of the study population experience more anxiety than boys (p=0.023), as well as children of divorced parents (p=0.020). On the contrary, in healthy children boys prevail over girls (P=0.006) whereas no statistically significant difference was found among children with thalassaemia.
IV. Intellectual and Academic level
In relation to the intellectual and academic level, children with cancer and especially boys believe that they have a good intellectual and academic level (p=0.005). However children aged 11?13 years old (p=0.042) and children aged 14?16 years old (p=0.006) believe they fall behind in this sector. From the healthy controls children aged 8?10 years old (P<0.001) and children aged 11?12 years old (P<0.001) believe that they are intellectually superior whereas children of divorced parents who belong to the group of thalassaemia believe they fall short in this level (P=0.037).
V. Happiness and Satisfaction
By applying the method of multiple regression and by using happiness and satisfaction as a dependent variable and demographic characteristics as an independent variable, no statistically significant correlation was found among children with cancer. Of the healthy children, those aged 8?13 years old (P=0.005) feel happier and more satisfied. Children with thalassaemia living with their grandparents or those of non?divorced parents express themselves positively regarding the factor of happiness and satisfaction P=0.044 and P=0.003. In contrast, children aged 17?19 years old feel less happiness (P=0.045).
Statistical results from the comparisons between groups
In order to determine the difference between the two mean values and standard deviations of the five factors, between the groups of children with cancer, of healthy children and of children with thalassaemia, the ‘analysis of variability’ and the ‘t?test’ were applied.
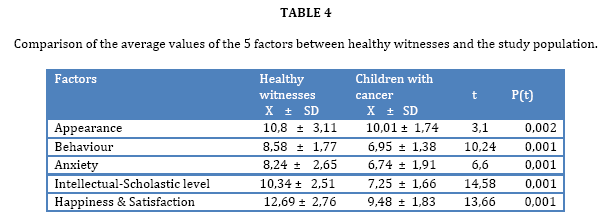
By comparing the mean values of the five factors mentioned above, between the healthy children and the children of the study (table 4), it was found that children with cancer evaluate themselves negatively in four of the factors in a statistically highly significant degree (p<0.001) with the exception of the factor of anxiety (p<0.001). In the present study the most anxiety is expressed by the controls, both healthy children and children with thalassaemia.
By comparing the mean values between healthy children and children with thalassaemia no statistically significant difference was found, except for the factor of intellectual and academic level, where children with thalassaemia believe they are superior in a statistically significant proportion (p=0.009) compared with healthy children.
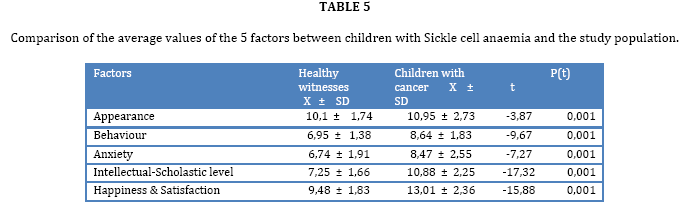
From the comparison of the mean values, between the children of the study and controls with thalassaemia, a difference of high statistical significance (p<0.001) was found in four factors, except for the factor of anxiety where the children of the study seem to have less anxiety. Children with thalassaemia express more intense anxiety (table 5).
From the comparison between healthy boys and boys with thalassaemia no statistically significant difference was found.
On the contrary, between the boys of the study and the boys with thalassaemia, it was observed that children with thalassaemia feel superior in the factors of behaviour, intellectual and academic level as well as in happiness and satisfaction (p<0.001), with the exception of appearance (P=0.018).
From the comparisons that took place between healthy girls and girls with cancer, healthy girls have larger values at a statistically highly significant proportion than girls with cancer in all factors (p<0.001), apart from the factor of anxiety (p=0.110).
In addition, from the comparison between healthy girls and girls with thalassaemia it was found that girls with thalassaemia feel greater anxiety (p=0.008), and also believe that they are of a higher intellectual and academic level (p=0.031).
In the comparison between girls with cancer and girls with thalassaemia a statistically significant difference was found in all factors (p<0.001), with the exception of girls with thalassaemia.
Discussion
In the present study the effect of cancer and its treatment on the child’s self?concept was evaluated, on the basis of five crucial factors which are: appearance, anxiety, intellectual and academic level and the feeling of happiness and satisfaction.
As the results of the general and clinical characteristics of the study population show, 50.3% of children suffered from acute lymphoblastic leukaemia which is the most frequent form of acute leukaemia in children, as reported in the international literature [29,30]. 61.8% were boys and 38.2% were girls.
The findings from the Piers?Harris scale, with the use of which it was investigated how children of all three groups (children with cancer, healthy children and children with thalassaemia) feel about themselves, it was found that each group does not present differences, other than the expected ones, when evaluated separately concerning the five factors. According to the answers given by the children of the study regarding the factor of appearance, no statistically significant difference was found between children. The children of the healthy group aged 8?12 years old believe their appearance is good. It is the age where children do not pay much attention to appearance and the secondary characteristics of their sex have not yet become so noticeable.
From the control children with thalassaemia, the children aged 17?19 years old believe they have a bad appearance. This is supported by clinical experience, which notice that if children of this age group with thalassaemia do not get good and correct treatment, a large proportion of them manifest changes in body image such as thin limbs, altered facial features and so on [31].
As for behaviour, by comparing the groups separately it was found that in all three groups girls believe their behaviour is better. In the group of healthy controls, children with divorced parents believe their behaviour is bad. This finding is in accordance with similar studies of children with divorced parents, where it was found that in the period of time after the divorce boys and girls experience significant emotional and behavioural disturbances. This type of behaviour is noticeable at home and school where negative social behaviour is observed. These children demonstrate aggressiveness, defiance and the need to ask for the help and attention of adults [32,33].
Girls of the study population experience more anxiety than boys. Although no difference in the intensity of anxiety between the two genders is reported in the international literature, the researchers Byrne and Hunsberger [34], Ryan [35], Shaw? Sorensen [36], Frydenberg and Lewis [37], report that boys express anxiety more through physical behaviour which may not so easily be perceived as an anxious behaviour, whereas girls use more emotional strategies. More intense anxiety and symptoms of depression were also observed in teenage girls with cancer in other studies [38,39].
Evaluation of the self-concept in the comparison of the three groups
From the comparison of the mean values of the five factors of the Piers?Harris scale between the children of the study and the children of both control groups, it appears that children with cancer have a negative image of themselves, whereas there is no difference between healthy children and children with thalassaemia. More specifically, no statistically significant difference was found between children of the control groups. The findings of this study agree with the study of Tsiantis40, who observed that children with thalassaemia do not differ from the healthy controls with regard to how they feel about themselves. A possible explanation of the above findings, as reported by the same researcher is that children with thalassaemia develop strong compensatory defence mechanisms; demonstrating an active denial of their problems in the face of uncertainty and anxiety due to their bad physical health and the continuous threat under which they live. Thus, it seems that, despite all the difficulties they experience, children with thalassaemia actively try to adjust to and deal with problems that arise from this chronic disease. In this study, children with thalassaemia, who demonstrate body image changes have a negative self?concept. On the contrary, children with thalassaemia, in contrast to healthy children, believe they are of a higher intellectual and academic level (p=0.009). An interpretation that one could give to this result is that these children know more facts about themselves, more issues concerning health and in addition, the attendance of these children at school is not stopped due to the good organisation of transfusion units. As mentioned above, children with cancer had a lower rate in all factors except anxiety, where it is observed that they experience less anxiety in comparison to witnesses. This finding is possibly a defence mechanism and in order to study its phenomenon in deeper analysis, more sensitive questions concerning anxiety measurement are required.
According to this study, children with cancer also present behavioural problems, a finding that agrees with those of Maguire’s study [41]. In another study by Enskär it was found that the disease and its treatment cause anxiety fear of the pain and the unknown, driving the child to social and physical isolation [42]. Such behavioural problems also occur at school. From related studies it has been found more explicitly that children with cancer demonstrate problems at school such as low sociability, anger, isolation, they are often tense and are frequently unable to concentrate [43-46].
In the present study, it was found that children with cancer experience less anxiety than the healthy controls and the controls with thalassaemia in both comparisons, whereas no statistically significant difference was found between the groups of healthy children and children with thalassaemia. The same result was found by the study of Srivastava [47]. However, the above finding does not agree with the finding of Tsiantis who used the Piers?Harris scale in children with thalassaemia and children with chronic disease, where it was found that there is no difference in how the children of these groups feel about themselves. Greater postoperative anxiety in children with cancer was found in the study of Lumley et al [48].
According to the results of the study, children with cancer believe they have a low intellectual and academic level, always in comparison with controls. It is obvious that the repeated visits and admissions of the child to hospital and the nature of the disease set obstacles to the child’s normal and regular attendance at school. Spinetta and Spinetta [49] found approximately the same. They compared 42 children undergoing treatment for leukaemia and other forms of cancer to 42 healthy children based on the teachers questionnaires. Children undergoing cancer treatment were more frequently absent from school, had learning difficulties, were unwilling to do things, and less active and 40% of these children had behavioural problems. The results of Eiser’s study were similar as well [50].
The children of this study also differ in a statistically significant degree from the controls in the fifth factor, i.e. happiness and satisfaction. One could say, without doubt, that this result is more or less expected from children with cancer as they face a plethora of problems.
Conclusions-Suggestions
The results of this study lead us to the following conclusions and suggestions:
Children with cancer have a negative view of their physical appearance, believe they have a negative behaviour at home and school in comparison with the control groups. They also believe that their performance at school is lower than that of other children and feel less happy and satisfied. Regarding the factor of anxiety, the study indicated that children with cancer experience less anxiety, a finding which suggests the need for more research.
The smooth adjustment of the child to the hospital environment, the sickness and its treatment, requires a scientific as well a personal humanistic approach so that the child maintains a positive selfconcept. In particular, the role of the nurse who cares for the child is important and must:
• operate as an essential link between the family and the therapeutic team.
• provide sufficient knowledge as far as the disease and its treatment are concerned, inspiring self?assurance and cooperation.
• provide consultation and supportive care to the child and his/her family.
A question to be asked and investigated in a future research study could be: whether nurses caring for such children can lessen or even reverse the results of this study.
3685
References
- Black, R., Bran, F., Ferlay, J., Parkin, D. Cancer incidence and mortality in the European Union. Cancer registry data and estimates of national incidence for 1990. Eur J Cancer, 1997; 33, 7: 1075‐1107
- Diler, L., Li FP. Epidemiology of Cancer in Childhood. In Hematology of Infancy and Childhood.Nathan D.G., Orkin, S.H.(eds) 5th ed. Philadelphia: W.B. Saunders, 1998; 1071‐1091
- Pinkerton, C. R., Sepion, Β. Childhood Cancer Management. A practical handbook. London, Chapman and Hall Medical. 1994
- Alcoser, P. N., Rodgers, CTreatment Strategies in Childhood Cancer. J. Pediatr Nurs, 2003; 18, 2: 103‐ 112.
- Zebrack, B. J., Chesler, M. A. Quality of Life in Childhood Cancer Survivors. Psychology 2003; 11; 2: 132‐41
- Hatira, P. The psychosocial rehabilitation and the quality of life of the child with cancer. Hellenic Oncology, 1993; 29, 1: 47‐52
- Papadatou, D. Caring for dying adolescents. Nursing Times, 1989; 85, 18: 28‐31
- Zeltzer, L. Cancer in adolescents and young adults: Psychosocial aspects. Cancer (Suppl), 1993 ; 7: 3463‐8
- Essen, L.V. et al. Self ‐ esteem, depression and anxiety among Swedish children and adolescents on and off cancer treatment. Acta Paediatric 2000; 89: 229‐36
- Beckham, J. C., Burker, E. J., Lytle, B.L.,Feldman, M. E., Costakis M.J. Self‐efficacy and adjustment in cancer patients: a preliminary. Behav Med. 1997 Fall; 23, 3: 138‐42
- Tram, JM., Cole, DA. Self‐perceived competence and the relation between life event depressive symptoms in adolescence : mediator or moderators. J Abnorm Psychol.2000; 109, 4: 753‐60
- Woodgate R., McClement S. Symptom distress in children with cancer: the need to adopts meaning‐ centered approach. J. Pediatr. Oncol. Nurs 1998; 15.1: 3‐12
- Hoffman KB, Cole DA,Martin JM, Tram J,Seroczynski AD. Are the discrepancies between self and others appraisals of competence Predictive or reflective of depressive symptoms in children and adolescents ; A longitudinal study, Part II. J Abnorm Psychol 2000 Nov; 109 (4): 651‐62.
- Hymovich,DP .The meaning of cancer to children. Seminars in Oncology Nursing II 1995; 51‐58.
- Hymovich,D and Roehnert,J. Psychosocial consequences of childhood cancer. Seminars in Oncology Nursing 1989; 5, 56‐62.
- Nichols M.L Social support and coping in young adolescents with cancer. Pediatric Nursing 1995; 21, 3: 235‐240.
- Woodgate R.L .Adolescents perspective of chronic illness. It is hard. J of Pediatric Oncol Nurs, 1998; 13, 210‐223.
- White, N.E., Richter J.M. & FryCoping, Social support and adaptation to chronic illness. West J Nurs Res.1992; 14 (2) 211‐224
- Ellerton, M.L., Stewrt, M.J., Ritchie et al. Social support in children with a chronic condition. 1996 ; Can J Nurs Res 28, 15‐36
- Cincotta, N. Psychosocial issues in the world of children with cancer. Cancer (Suppl) 1993; 71, 3251‐3259.
- Enskar, k.. Carlsson, M., Colstater, M., Hanrin, E. Symptom distress and life situation in adolescents with cancer. Cancer Nurs, 1997; 20, 23‐33
- Spirito, A., Stark, L.J. Gil, K.M. & Tye, V.L. Coping with every day and disease – related stressors by chronically ill children and adolescents. Journal of the American Academy of Adolescent Psychiatry,
- Eapen, V., Revesz, T., Mpofu, C., Daradkeh, T. Self‐perception profile in children with cancer: self vs parent. Psychol, 1999; 84, 2: 427‐432
- Pendley, JS, Dahlquist, LM. Dreyer, Z. Body image and psychosocial adjustment in adolescent cancer survivors. J. Pediatr. Psychol, 1997; 22, 1:29‐43
- Piers,E., Piers‐Harris Childrens’ Self‐concept Scale. Revised Manual 1984, Western Psychological Services, Los Angeles, California 1988.
- Anagnostopoulos, F., Papadatou, D. Factorial composition and internal coherence of the occupational fatigue recording questionnaire on a specimen of nurses. Psychological . Subjects1992; 5, 3: 183‐202.
- Dawson‐Saunders, B., Trapp R. G. Basic and clinical Biostatistics. Appleton & Lange, New York 1990; 120.
- Trihopoulos, D. Medical Statistics. Principles and Basic Methods of Biomedical Statistics. Parisianos, Athens 1975; 39‐58 & 95 – 126.
- Linet, M.S., Rise, L.A., Smith, M.A. et al. Cancer surveillance series recent trends in childhood cancer incidence and mortality in the United States. J. Natl Cancer Inst, 1999; 91: 1051‐1058
- Colby‐Graham, M.F., Chordas, Ch. The childhood Leukemias. J. of Pediatric Nursing, 2003; 18, 2: 87‐95
- Philippidis, F. Haemopoesis. Anaemia. Leukocyte Disorders. Abridged pediatrics, K. Papadatos, publisher Litsas, Athens 1987.p. 333‐382
- Timms, J. The silent majority‐ The position of children involved in the divorce and separation of their parents. Child Care in Practice, 2003; 9, 162‐175.
- Buchaman, C.M., Maccoby, E., Dornbusc, S.M. Caught between Parents: Adolescents’ experience in ivorced homes. Child Development, 1991; 62, 1008‐1029.
- Byrne, C., Hunsberger, M. Stress, crisis and coping. In Nursing Care of Children, Betz, C., unsberger, M., Wright, S. (eds) W.B. Saunders company. Montreal 1994; 629‐650.
- Ryan, N., Stress and coping strategies identified from school age children’s perspective. Res Nurs and Health 1989; 12, 2: 111‐122
- Shaw‐Sorensen, E., Children’s coping responses. J Pediatr Nurs 1990; 5, 4:259‐267
- Frydenberg, E., Lewis, R., Adolescent coping: The different ways in which boys and girls cope. J Adol 1991; 14, 119‐133.
- Brage, D., Grossman, C.C., Dunkel, J. Psychological correlates of adolescents’ depression. J Child and Adol Psych Nurs, 1995; 8, 23‐30
- Lamarine, R.S. Child and adolescent depression. J School Health, 1995, 65, 390‐393
- Tsiantis, I. Mental disturbances and intelligence of children with thalassaemia. Thesis for lectureship, Athens 1984. p. 48
- Maguire, G. P. The Psychological sequelae of childhood leukaemia. Cancer Res, 1983; 88, 47‐56.
- Enskär, K., Carlsson, M., Golsäter, M., Hamrin, E., Kreuger, A. Life situation and problems as reported by children with cancer and their parents. J Pediatr Oncol Nurs, 1997a; 14, 18‐26.
- Ģavuşoğlu, H. Depression in children with cancer. J. Pediatr Nurs, 2001; 16, 5: 380‐384.
- Valente, S. M., Saunders, S. M. Diagnosis and treatment of major depression among people with cancer. Cancer Nurs, 1997; 20:168‐177.
- Noll, R.B., Garstein, M.A., Vannatta, K., Correll, J., Bukowski, W.M., Davies, W.H. Social emotional and behavioral functioning of children with cancer. Pediatr, 1999; 103, 71‐78.
- Vance, Y.H., Eiser, C. The school exsperience of the child with cancer. Child: Care, Health and Development, 2002; 28, 1: 5‐19.
- Srivastava, P. S.. Approaches to the measurement of depressive symptomatology of children with cancer. attempting to circumvent the effects of defensiveness. J. Dev. Behav. Pediatr. 1999; 20, 3:150-156.
- Lumley, M., Melamed, B., Abeles, L., Predicting children’s presurgical anxiety and subsequent behaviour changes. J Paediatr Psych 1993; 18, 4: 481‐487
- Spinetta, P. D., Spinetta, J.J. Teachers’ appraisal: the child with cancer in school. A J Pediatr. Hemat. Oncol. 1980; 2:89‐94
- Eiser, C. Cognitive deficits in children treated for leukemia. Arch Dis Child, 1991; 66, 164‐168.

