Keywords
Depression in elderly, primary care, Zung Self-Rating Depression Scale
Introduction
The proportion of the elderly in the population and the life expectancy after birth are increasing. This is the trend which has been seen in both developed and developing countries [1]. Depression is characterized by persistent feelings of extreme sadness and low mood associated with loss of interest in activities and inability to experience pleasure. There are often associated biological features of significant changes in appetite and weight, disturbed sleep, fatigue and poor concentration. Reported prevalence rates in the elderly population ranged from 0.8% for major depression to 26% for affective disorders and neurosis [2,3].
The community-based mental health studies in India have revealed that the point prevalence of depression in geriatric Indian population varies between 13% and 25% [4,5]. Diseases like cancer, cardiovascular diseases, diabetes, infections and poor oral health, most notably tooth loss are more prevalent in this age group. Chronic disease and most oral diseases share common risk factors. Globally, poor oral health amongst older people has been particularly evident in high levels of tooth loss, dental caries experience, and the prevalence rates of periodontal disease, xerostomia and oral cancer [6].
Elderly have a disproportionately high incidence of depression. Depression is more common in hospitals and nursing homes [7]. Depression can reduce a satisfaction of late life and also, can significantly reduce life expectancy. The elderly have the highest suicide rate and a range of physical disorders which make depression more severe [8]. It can be a psychological reaction to the illness, or directly caused by the physical illness [9]. Stressful life events retain a substantial causal relationship with the onset of depressive episodes [10]. No clear evidence is available on the differential role of life events in males and females, but the quality of experience associated with life events may contribute to gender differences in depression [11]. In the elderly, a number of life changes can increase the risk for depression, or make existing depression worse. Some of these changes are: adapting to a move from home to an apartment or retirement facility, chronic pain, feelings of isolation or loneliness as children move away and their spouse and close friends die, loss of independence (problems getting around, caring for themselves, or driving), multiple illnesses, struggles with memory loss and problems thinking clearly. Similarly, the ageing process of some serotonin systems might be more apparent in females than males, as measured by diurnal variations in imipramine binding and serotonin uptake in platelets. The likelihood of a relationship between food intake, weight gain and depressed mood in females, with brain serotonin being involved in these disturbances of mood and appetite, is intriguing [12]. Physical illnesses that increase the risk for depression include: thyroid disorders, Parkinson's disease, heart disease, cancer, and stroke. Symptoms of depression may occur as part of dementia (Alzheimer's disease). Symptoms of depression are also a side effect of many drugs commonly prescribed for the elderly [13].
Objectives
The purpose of the present study was the subjective assessment of the depressive symptoms of the elderly as reflected in the last week. Also, the individual targets were to investigate the prevalence of depressive symptoms and their correlation with the daily life events.
Methods
Study Design
The survey was conducted in a 4-month period (March - June 2011) in 4 nursing homes in Heraklion of Crete. All registered members were 208 elderly. Included criteria were a) age over 65 years b) the information is provided only by the participant and c) to be a registered member in the last year. Eight people were excluded because of collaboration and consultation problems. The study was conducted with the quantify-descriptive method. A questionnaire was used to collect demographic information and past medical history, including smoking habit, CVD (congestive heart failure, coronary artery disease, and arythmias), mental diseases (already diagnosed depression, dementia, psychotic disorder, and anxiety disorder) and other chronic diseases (COPD, Hypertension, and Diabetes mellitus). Collection that concerns depressive symptoms was performed using the Zung Depression Rating Scale (ZDRS).
The study questionnaire
The Zung Depression Rating Scale consists of 20 items that cover affective, psychological and somatic symptoms. The patient specifies the frequency with which the symptom is experienced (Likert scale): a little = 1, some = 2, a good part of the time = 3, or most of the time = 4. Scores on the test range from 20 through 80. The scores fall into four ranges : 20-49 Normal Range, 50-59 Mildly Depressed, 60-69 Moderately Depressed, 70 and above Severely Depressed [14].
The ZDRS is a self-reporting instrument and was originally developed in order to assess depression symptoms in 20 situations: I feel down-hearted and blue, morning is when I feel the best, I have crying spells or feel like it, I have trouble sleeping at night, I eat as much as I used to, I still enjoy sex, I notice that I am losing weight, I have trouble with constipation, my heart beats faster than usual, I get tired for no reason, my mind is as clear as it used to be, I find it easy to do the things I used to, I am restless and can't keep still, I feel hopeful about the future, I am more irritable than usual, I find it easy to make decisions, I feel that I am useful and needed, my life is pretty full, I feel that others would be better off if I were dead, I still enjoy the things I used to do. Moreover, individual questions (demographic data - age, sex ect) will be reported in order to serve the goals of the present study.
Statistical Analysis
With the x2 test analysis were analyzed the distributions of the descriptive characteristics of the patients (age, gender, education level) that were associated with depression and the distributions of the symptoms of the depression with features health habits (smoking, sleep, etc.), or other chronic diseases (diabetes, hypertension, snoring, etc.). Also, with the r-Pearson partial correlation coefficient were analyzed the depression scores in a correction (controlling) as to the gender of the elderly. Finally, the Cronbach's α (alpha) was used as a measure of the internal consistency or reliability of the psychometric test score for the sample of examinees. In the present study the question that concern the “enjoy of sex” was excluded by statistical analysis due to missing data. The data analysis was performed using the statistical programme IBM SPSS 19.0.
Results
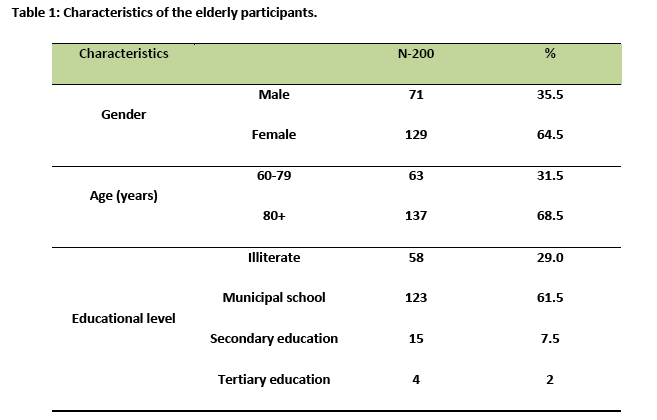
A total of 200 elderly were enrolled in the study from four nursing homes in Heraklion of Crete. The coefficient of Cronbach's alpha was a = 0.81 and reached the acceptable range for internal consistency. Table 1 shows the characteristics of the respondents. Most of them were female (64.5%), aged above 80 years (68.5%), with low level of education (90.5%), (data not shown)
The mean score of depression for the elderly where the value was 49 which is a normal result. The overall prevalence of depression reached 58.5%, the mild depression was 52.0%, the moderate depression was 6.5% and none was found with severe depression. The total prevalence of symptoms of mild and moderate depression was 46.5% in male and in 65.1% in females.
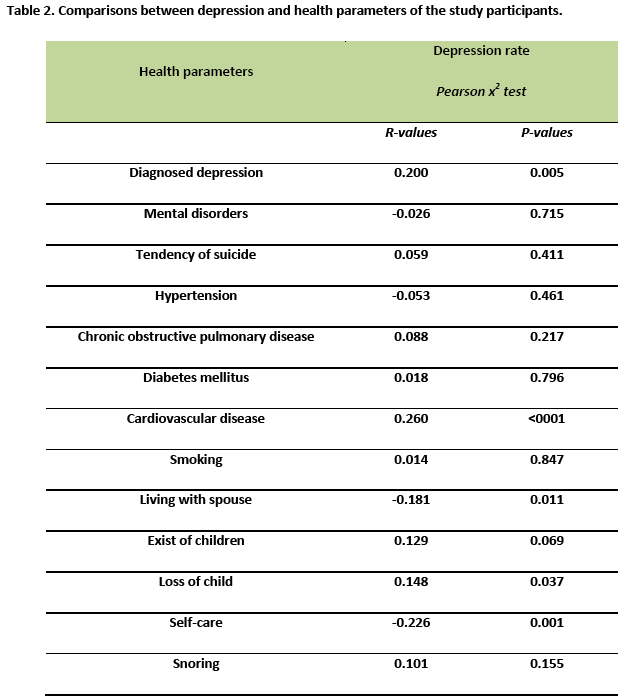
Table 2 shows the association between depression and health parameters. These parameters had statistically significant correlation with depression: diagnosed depression (P-value = 0,005), cardiovascular disease (P-value <0,001), living with spouse (P-value = 0,011), loss of child (P-value = 0,037), self-care (P-value = 0,001). In mild depression the appearance of cardiovascular disease was 32.7% and the moderate depression had a significant increase of the percentage that was 46.2% . There was a decreasing trend of cases where the elderly are not affected by if live on their own or with their spouses. There was statistically significant difference between normal (14.5%) and mild depression (6.7%). In the moderate depression the percentage was 0%. The highest percentage of elderly with self-care had normal depression 63.9% while there was significantly reduced of the percentage of elderly with mild depression (43.3%) and fewer declines in the elderly with moderate depression (38.5%). The elderly that had slept 13 hours had mild depression 15.4%, whereas in moderate depression the result was 0% if the elderly had slept less than 13 hours. From the present study we found how significant the loss of a child to assess the degree of depression was. There was not much difference between normal (7.2%) and mild depression (8.7%). It is noteworthy that there was an almost fourfold difference in moderate depression (30.8%). Also, it seems that snoring was an important indicator in the rating of depression.Τhere was ascending trend to normal (31.3%), to mild (42.3%) and moderate depression (61.5%). The present survey shows the percentage of elderly that had already diagnosed with depression. There was steadily increasing trend among patient with normal depression (36.1%), mild depression (48.1%) and moderate depression (61.5%).
Discussion
The mean depression score of elderly people was 49 in ZDRS scale. This means that the average depressed mood is below 50 where 50 or more is a sign of depressive disorder. Diagnosing major depression in the elderly is positively correlated with the total rating.
The main finding of our study was the high rate of moderate depression which was significantly associated with CVD. There was an upward trend for the appearance of CVD. The most cases of elderly people with CVD were associated with depression symptoms. Several studies [15-17] in the literature are in congruent with the above finding that many people suffer from these two disorders and that is coexistence of these. Moreover, depression in elderly is further complicated by the high levels of co-morbidity with medical conditions, including cancer, cardiovascular disease, and neurological disorders [18,19].
Life changes can increase the risk for depression, or make existing depression worse. Some of these changes are: adapting to a move from home to an apartment or retirement facility, chronic pain, feelings of isolation or loneliness as children move away and their spouse and close friends die [20]. Our results suggest that the loss of loved ones especially a child and the existence of spouse are in an agreement with the above writers. Also, in a survey [21] was found that the loneliness in the lives of elderly can be a major risk factor for the occurrence of serious mental health concerns such as depression. In addition, quality of experience associated with life events may contribute to gender differences in depression [22].
In the present study was found that female participated to a greater proportion aged above 80 years with low level of education. It is evident that the symptoms of mild depression appeared in elderly people aged over 80 years. The total prevalence of mild and moderate depression 47.7% was in the age group 60-79 while in the aged group over 80 years was 63.5%. It is also worth noting that there was not an incident with major depression (aged above 70 years) according to the Zung Depression Rating Scale. The most recent studies indicate that generalized depressive disorder is the most common disorder among adults over 60 years [23]. Of all the elderly that are addressed in primary care the 25% presents an depressive disorder, while in the aged group over 65 years the incidence of generalized depressive disorder is estimated at 14% [24,25]. Moreover, there was a high prevalence of mild and moderate depression among individuals with lower level of education (illiterate 62%, primary school 61%). In a research in University of Illinois [26] found that the higher the level of education is, the less is the depression. Ιt was noticed a big difference in the incidence of mild depression in female than in male. The total prevalence of symptoms of mild and moderate depression was 46.5% in male and in 65.1% in females. Two studies showed that female is consistently a significant risk factor for depression in the elderly [27,28].
No significant association was found between mental disorders, tendency of suicide, hypertension, diabetes mellitus, smoking, snoring and COPD. These results are probably appeared due to a small sample, but many studies suggest the association of above finding of medical history with the depression [29,30].
A potential limitation of our study may be the fact that the assessment factors because the self-reference answers have subjective value and the elderly are an age group with specific physical and mental characteristics. Another potential limitation was that diagnosis of depression was not given by specialist neurologist in all participants. Finally, the low educational level is an important difficulty in collaboration and consultation in aging generally.
Conclusions
Old age is one of the most vulnerable age groups and requires more attention and care from the other age groups. This study confirms that depression is related with cardiovascular diseases. Our data suggest that the life situations of elderly are directly related to life situations such as self-care, loss of child, loneliness and chronic diseases which affect the daily mood. All these situations are associated with the daily mood increasing the normal depressive mood to high levels in elderly.
2807
References
- Kinsella K, Phillips D. Global aging: The challenge of success. Population Bulletin 2005; 60(1):1-40.
- Blazer D, Hughes DC, George LK. The epidemiology of depressionin an elderly communi- ty population. Gerontologist 1987; 27(3):281–287.
- Kay D, Beamish P, Roth M. Old age mental disorders in Newcastle-upon-Tyne. Br J Psychiatry 1964; 110:668-82.
- Nandi D. The Incidence of mental disorders in one year in a rural community in West Bengal. Indian Journal of Psychiatry 1997; 39.2: 122.
- Ramachandran V, Menon-Sarada M, Arunagiri S. Socio-cultural factors in late onset depression. Indian J Psychiatry 1982; 24(3): 268 –73.
- Petersen P, Yamamoto T. Improving the oral health of older people: The approach of the WHO Global Oral Health Programme, Community Dentistry Oral Epidemiology 2005; 33:81–92.
- Mulsant H, Ganguli M. Epidemiology and Diagnosis of depression in late life. J Clin Psychiatry 1999; 60(2): 9-15.
- Salvatore T. Elder Suicide. A preventable tragedy. Caring 2000; 19(3) :34-7.
- Unutzer J. Clinical practice: late-life depression. N Engl J Med 2007; 357(22):2269-2276.
- Kendler K, Karkowski L, Prescott C. Causal relationship between stressful life events and the onset of major depression. American Journal of Psychiatry 1999; 156(6):837-841.
- Bebbington P. The origins of sex differences in depressive disorder: bridging the gap. International Review of Psychiatry 1996; 8(4):295-332.
- Wurtman J. Depression and weight gain: the serotonin connection. Journal of Affective Disorders 1993; 29(2): 183 -192.
- Unutzer J. Clinical practice: late-life depression. N Engl J Med 2007; 357(22):2269-2276.
- Zung W. "A self-rating depression scale". Archives of General Psychiatry 1965; 13(6): 508.
- Mirowsky J, Ross C. Age and Depression. Journal of Health and Social Behavior 1992; 33:187-205.
- Licinio J, Yildiz B, Wong M. Depression and cardiovascular disease: co-occurrence or shared genetic substrates. Molecular Psychiatry 2002; 7(10):1031-2.
- Charney D, Reynolds C, Lewis L, Lebowitz D, Sunderland T, Alexopoulos G, Young R. Depression and Bipolar Support Alliance consensus statement on the unmet needs in diagnosis and treatment of mood disorders in late life. Archives of General Psychiatry 2003; 60.7: 664.
- Krishnan K, Delong M, Kraemer H. Comorbidity of depression with other medical diseases in the elderly. Biol Psychiatry 2002; 52:559–588.
- Wurtman J. Depression and weight gain: the serotonin connection. Journal of Affective Disorders 1993, 29(2): 183 -192.
- Beal C. Loneliness in older women: a review of the literature. Issues Ment Health Nurse 2006; 27(7) :795-813.
- Bebbington P. The origins of sex differences in depressive disorder: bridging the gap. International Review of Psychiatry 1996; 8:295 -332.
- Mohlman J, Price R. Recognizing and treating late –life generalized anxiety disorder: distinguishing features and psychosocial treatment Expert Rev Neurother 2006; 6:1439-45.
- Flint J. (Generalized anxiety disorder in elderly patients: Epidemiology, diagnosis, and treatment options. Drugs Aging 2005; 22(2):101-14.
- Τolin F, Robison J, Gaztambibe S, Blank K. Anxiety disorders in older Puerto Rican primary care patients. Am J Geriatr Psychiatry 2005; 13(2):150-6.
- Fountoulakis K. Reliability, validity and psychometric properties of the Greek translation of the zung depression rating scale. BMC Psychiatry 2001; 1(1):3.
- Cole M, Dendukuri N. Risk factors for depression among elderly community subjects: a systematic review and meta-analysis. Am J Psychiatry 2003; 160(6):1147–1156.
- Djernes J. Prevalence and predictors of depression in populations of elderly: a review. Acta Psychiatr Scand 2006; 113(5):372–387.
- Meana J, Barturen F, Garcia – Sevilla J. a2-Adrenoceptors in the brain of suicide victims: increased receptor density associated with major depression. Biological Psychiatry 1992; 31 (5): 471-490.
- Mikkelsen L, Middelboe T, Charlotta P, Stage K. Anxiety and depression in patients with chronic obstructive pulmonary disease (COPD). Nordic Journal of Psychiatric 2004; 58(10):65-70.

