Keywords
Anxiety; Cancer; Depression; Siege; Stressors
Introduction
For the last 7 years, there were an increasing number of the cancer patients among the Palestinian people that call actions and interventions by researchers and clinicians to stand as the basis and the nature of the cancer. Cancer mortality rates show the remarkable increase in Palestine during 2013 compared with 2007 and 2010, from (10.3%) in 2007 to (10.8%) in 2010 then increases to reach (13.3%) from the total deaths in Palestine in 2013(MOH, 2014). Breast cancer ranked first, with (401) reported cases, (18.3%) cases. Breast cancer is the highest among females and focus in the age group between 20-59, where colon cancer ranked second, with (236) reported cases and (10.8%) from all reported cancers (MOH, 2014). According to MoH reports, cancer considered the second-leading cause to death in Palestine. Cancer or terminally ill patients cannot receive any more treatment in Cairo or Israel for the closure of the borders [1]. Patients with cancer suffer from a wide range of stressors, including but not limited to stressing, anxiety, depression, physical health disturbance, and malnutrition and mood imbalance. Subsequently, the war and siege aggregate these stressors and increase the chance of death as a result of limited medications, equipment, and transfer procedures. Palestinian breast cancer patients and survivors reported considerably higher levels of cancer-related posttraumatic stress symptoms than Danish women with comparable disease severity [2]. Furthermore, the stressors of the cancer patients at Shifa hospital where state anxiety was at the highest rank 60.8%, followed by trait anxiety 54.6%; re-experiencing PTSD at the third rank 47.0%, PTSD 42.5%, hyper-arousal 40.5%, avoidance 40.1% [3]. There are many stressors that face women diagnosed with cancer, including the fear of possible death, stress of informing family members, and the stress associated with being informed that their lives is going to be drastically change. Disruption, social stigmatization, side effects of treatment, and other stressors more specific for the disease and treatments are also pertinent [4]. These stressors can occur within the context of a disrupted family and other ongoing sources of stress. Psychiatric problems have been frequently reported in cancer patients [5].
Cancer patients experience different types of stressors that generated from the cancer itself that presented to the patients suffering from cancer. Cancer is chronic, rather than acute stressors [6] and presents a series of different traumatic events over time, including diagnosis, disease progression, treatment, adverse physical effects (e.g. disfigurement) and recurrence [7,8]. Found that cancer-related symptoms are the strongest predictors of depression and the PTSD subdimension of hyper-arousal. These effects persist even when the effects of other stressors and non-cancer illness symptoms are statistically controlled. Patients with cancer face most of the stressors associated with diagnosis, illness and treatment. Cancer diagnosis and treatment brings changes in patient’s personal paths of life, in their daily activities, work, relationships, and family roles, and it is associated with a high level of patient psychological stress. This stress shows up as anxiety and/or depression [9]. These stressors may generate coping strategy, which may affect the mental health [10,11]. In a study to determine the levels of depression and anxiety, and coping strategies, and the effects of the levels of depression and anxiety on strategies for coping with stress in cancer patients. Anxiety was determined in 61.5% and depression in 81.3% of the patients. Other epidemiological and clinical studies over the past 30 years have provided strong evidence for links between chronic stress, depression, social isolation and cancer progression. Cancer and stress disease are both characterized by a huge complexity, heterogeneity and multifactorial pathogenesis. It is well accepted that cancer growth involves the microenvironment, a space where tumor cells receive nutrients from the host tissue, produce angiogenetic factors and form new vessels [12,13]. In a study aimed to identify clinical factors that are predictive of depression and quality of life (QOL) among 209 long-term survivors of head and neck squamous cell carcinoma and to develop predictive scores using these factors. The results showed significant pretreatment predictors of depression were identified on multivariate analysis as smoking at diagnosis. Furthermore, Ellis G [14] aimed to assess the prevalence of general anxiety and depression, as well as procedure-related worry and pain in patients undergoing local anaesthetic flexible cystoscopy and to determine whether these conditions occur more frequently in subsets of the population. The prevalence of significant anxiety was 15% and depression 3.5%.
Al-Jadili et al. [3] in a study aimed to examine the mental health status of the patients with cancer and the coping strategies that adopted by them in front of stressful situation. 42.5% of patients had PTSD. 47% had been re-experiencing of PTSD. 40.5% had been hyperarousal, and 40.1% had avoidance symptoms. The common emotional reactions in patients diagnosed to have cancer are shock, denial, disbelief, anxiety, anger, guilt, and depression. The major sources of continuing emotional distress are fear of incurability, pain, disfigurement, recurrence of disease, and a sense of helplessness over its treatment. Life stressors due to war and siege are linked to exacerbation of chronic medical conditions and mental-health problems in a variety of populations, including cancer patients. The study aims were 1) to explore the types and severity of stressors due to siege among cancer patients in Gaza Strip, 2) to explore the types and severity of war trauma among cancer patients, 3) to find prevalence of depression and anxiety among patients with cancer, 4) to explore the relationship between stressors due to siege, war trauma, depression and anxiety among cancer patients in and other sociodemographic variables.
Methods
Participants
The study sample consisted of 358 patients selected randomly from a total of 3683 cases (MOH, 2015). Of 358, 114 were males (32%) and 244 were females (68%).
Measures
Socio-demographic status
A brief socio-demographic questionnaire developed containing the magnificent data about the patients with cancer including sex, age, income, working status and other variables.
Medical history
While confirming the disease history of occurrence, type of drug taken (medical or chemotherapy) and the diagnosis.
Gaza siege stressful situations checklist [15]:
Stressful situations experiences were collected by using Gaza Siege Stressful Situation (GSSS) Checklist, this was developed before 2009 [15] and was modified recently [16], describing the most common stressful experienced during the last 10 years of closure and seize of Gaza Strip. This checklist consisted of 19 items with answers Yes (1) and no (0). The current scale was modified for Cancer patients. The scoring of the scale is considered by summing all the answers. In this study, the split half reliability of the scale was high (r=0.70). The internal consistency of the scale was calculated using Cronbach's Alpha was (α=0.78).
Beck depression inventory short form
The Beck Depression Inventory (BDI) is a 21-item; self-report rating inventory that measures characteristic attitudes and symptoms of depression [17]. The BDI has been developed in different forms, the 13-item short form and the more recent BDI-11 by Beck et al. [18]. Internal consistency for the BDI ranges from 0.73 to 0.92 with a mean of 0.86 [19]. Similar reliabilities have been found for the 13-item short form [20]. The BDI demonstrates high internal consistency, with alpha coefficients of 0.86 and 0.81 for psychiatric and nonpsychiatric populations respectively [19].
This inventory was validating in Palestine culture [21]. The severity of depression is classified on the basis of the total score; in a normal community sample, a BDI score <4 suggests no or minimal depression, 5 to 7 represents mild to moderate depression, 8 to 15 is moderate to severe and ≤ 16 indicates a severe level of depression. The internal consistency of the scale in study using Cronbach's Alpha was (α=0.86).
Hamilton anxiety scale (Hamilton)
The Hamilton Anxiety Scale (HAM-A) was one of the first rating scales developed to measure the severity of anxiety symptoms, and is still widely used today in both clinical and research settings. The scale consists of 14 items, each defined by a series of symptoms, and measures both psychic anxiety (mental agitation and psychological distress) and somatic anxiety (physical complaints related to anxiety). Although the HAM-A remains widely used as an outcome measure in clinical trials, it has been criticized for its sometimes poor ability to discriminate between anxiolytic and antidepressant effects, and somatic anxiety versus somatic side effects. The HAM-A does not provide any standardized probe questions. The items are rated on a five-point scale and summed to provide a score ranging from 0 to 56. A score of 17 or less represents mild anxiety, a score between 18 to 24 mild to moderate anxiety, and a score of 25 and above moderate to severe anxiety. The scale has been shown to differentiate older adults with generalized anxiety disorder from those with no anxiety disorders [18]. The scale was validated in previous studies in the Gaza Strip and showed validity and reliability in measuring depression [22]. The internal consistency of the scale in study using Cronbach's Alpha was (α=0.88).
Study procedure
The study was conducted in the in two cancer departments in Gaza Strip (European Gaza and Al Shifa Hospital). A letter of Approval for conducting this study was obtained from local Ethical Helsinki committee in Gaza. Another two letters from Ministry of Health and hospitals’ administration were obtained to collect data from the two departments. A consent form each patient was granted to participate in the study with an explanation the aims for the study and that the information will be kept with the researcher. The sample was a random sample in which we calculated the sample of the cancer patients who registered with the hospital directorate and attending the governmental hospitals and out-patients clinics (N=380) out of the total number of registered cancer patients in Ministry of Health in Gaza Strip (N=3683).
The data was carried out by the first author and by the help group of four nurses in the two departments who had been trained for four hours in data collection. The patients were interviewed at out-patients clinics and inside the oncology departments. The data collection was carried out from September 2015 to November 2015.
Statistical Analysis
Statistical Package for the Social Sciences (SPSS version 21.0; SPSS, IBM, Chicago, IL, USA) was used for descriptive statistics. Frequency tables that show sample characteristics and plot differences between various Gaza hospitals and out patient's clinics and clients characteristics variables will be done. Moreover, cross tabulation for main findings and advanced statistical tests such as Chi-square test to compare categorical variables, and T test or One-way ANOVA test to compare means of numeric variables will be done when required to analyze questionnaire data. Pearson's correlation test was used to find the relationship between stressors due to siege, anxiety, and depression. The level of significance was set at p<0.05.
Results
Sociodemographic characteristics of the study sample
The total number of sample selected for the current study were 380 cancer patients, 128 (33.7%) of the sample were males and 252 (66.3%) were females. The age ranged from 18-75 years, mean age patients was 52.7 years (SD=14.77 years). According to marital status, 10.5% were single, 85% were married, 2.9% were divorced and 1.6% was widowed. The results showed that; 48 of the cancer patients were not educated (12.5%), 48 were educated to elementary school (12.6%), 78 were to preparatory level (20.5%), 122 father of sample were to secondary education (32.1%), 33 were educated to diploma level (8.7%), 50 were educated to the university level (13.2%), and 1 was educated to the post graduate level (0.3%). The results showed that; 334 were unemployed (87.9%), 17 were simple worker (4.5%), 5 were skilled worker (1.3%), 20 were employee and working (30.8%), 3 were civil employee not at work and getting salary (0.8%), and 0.3% were merchants (Table 1).
Table 1. Distribution of the sample according to gender (N=380).
| Variable |
N |
% |
| Gender |
| Male |
128 |
33.7 |
| Female |
252 |
66.3 |
| Age |
| Less than 24 y |
23 |
6.1 |
| From 25 to 34 |
26 |
6.8 |
| From 35 to 44 |
54 |
14.2 |
| From 45-54 |
79 |
20.8 |
| 55 and above |
198 |
52.1 |
| Marital status |
| Single |
40 |
10.5 |
| Married |
323 |
85 |
| Divorce |
11 |
2.9 |
| Widowed |
6 |
1.6 |
| Place of residence |
| North Gaza |
75 |
19.7 |
| Gaza |
152 |
40 |
| Middle area |
71 |
18.7 |
| Khan Younis |
48 |
12.6 |
| Rafah |
34 |
8.9 |
| Family size |
| Four and less children |
150 |
39.5 |
| Five to seven siblings |
134 |
35.3 |
| Eight and more siblings |
96 |
25.3 |
| Family monthly income |
| Less than $400 |
321 |
84.5 |
| $401 - $600 |
38 |
10 |
| $601 - $750 |
11 |
2.9 |
| $751 and more |
10 |
2.6 |
| Patients’ education |
| Not educated |
48 |
12.6 |
| Elementary |
48 |
12.6 |
| Preparatory |
78 |
20.5 |
| Secondary |
122 |
32.1 |
| Diploma |
33 |
8.7 |
| University |
50 |
13.2 |
| Post graduate |
1 |
0.3 |
| Patients’ job |
| Unemployed |
334 |
87.9 |
| Simple worker |
17 |
4.5 |
| Skilled worker |
5 |
1.3 |
| Civil employee and working |
20 |
5.3 |
| Civil employee not at work and getting salary |
3 |
0.8 |
| Merchant |
1 |
0.3 |
Medical history
The commonly reported cancer types were: breast cancer (38.2%), lymphoma (13.7%), leukemia (11.3%), and colon cancer (8.4%) (Table 2).
Table 2. Type of cancers (N=380).
| Type of cancer |
No |
% |
| Breast Cancer |
145 |
38.2 |
| Lymphoma |
52 |
13.7 |
| Leukemia |
43 |
11.3 |
| Colon cancer |
32 |
8.4 |
| Cancer liver and spleen |
26 |
6.8 |
| Bladder cancer |
26 |
6.8 |
| Metastasis |
8 |
2.1 |
| Stomach cancer |
7 |
1.8 |
| Uterus cancer |
6 |
1.6 |
| Cancer brain |
6 |
1.6 |
| Spinal cord cancer |
6 |
1.6 |
| Intestinal cancer |
5 |
1.3 |
| Mouth and throat cancer |
5 |
1.3 |
| Colon cancer |
5 |
1.3 |
| Bone marrow cancer |
4 |
1.1 |
| Chest Cancer |
4 |
1.1 |
Type of stressors due to siege
The most common reported stressors due to siege were: 353 of participants (92.9%) said prices are sharply increased due to closure, 343 said they feel that they are in big prison (90.3%), 325 said their work affected so much due to cut-off of electricity and shortage of gas (85.5%). The patients with cancer reported from 2-16 stressors due to siege with mean 9.02 (SD=2.53) (Table 3).
Table 3. Types and frequency of stressors due to siege (N=380).
| |
Yes |
No |
| Stressor |
% |
No |
% |
No |
| 1. Prices are sharply increased due to closure |
353 |
92.9 |
27 |
7.1 |
| 2. I feel I am in a big prison |
343 |
90.3 |
37 |
9.7 |
| 3. My work affected so much due to cut-off of electricity and shortage of gas |
325 |
85.5 |
55 |
14.5 |
| 4. Social visits are less than before |
302 |
79.5 |
78 |
20.5 |
| 5. I cannot finish some construction and repair work in my house due to shortage of cement and building materials |
287 |
75.5 |
93 |
24.5 |
| 6. I sold some of my furniture and my wife's gold. |
264 |
69.5 |
116 |
30.5 |
| 7. I cannot get medicine |
228 |
60 |
152 |
40 |
| 8. I cannot go outside the Gaza Strip for treatment when there is no treatment in Gaza |
174 |
45.8 |
206 |
54.2 |
| 9. I went to Zakaorganizations and other organizations to get the food |
168 |
44.2 |
212 |
55.8 |
| 10. I was not able to get specific medicine for me or for one of the family member |
157 |
41.3 |
223 |
58.7 |
| 11. I had suffering of not able to receive proper medical care due to shortage of medicine |
154 |
40.5 |
226 |
59.5 |
| 12.I Cannot travel for treatment and work |
117 |
30.8 |
263 |
69.2 |
| 13. I stopped completely working due to siege |
104 |
27.4 |
276 |
72.6 |
| 14. One of the family member died due to prevention of traveling for treatment |
103 |
27.1 |
277 |
72.9 |
| 15. I stopped sending my children to schools and send them to work to help the family |
96 |
25.3 |
284 |
74.7 |
| 16.I thought of immigration |
93 |
24.5 |
287 |
75.5 |
| 17. My monthly income decreased and can’tsend my children for schools |
83 |
21.8 |
297 |
78.2 |
| 18. I went to human rightsorganizations and other organizations to get the help for travel outside Gaza for treatment |
58 |
15.3 |
322 |
84.7 |
| 19.I was prevented from visiting one of the family members in Israelis jails |
19 |
5 |
361 |
95 |
Differences in stressors due to siege and other socioeconomic variables
In order to find differences in types and severity of stressful situations due to siege and other sociodemographic variables such as, a t-independent test was conducted. Also, One Way ANOVA was done for groups more than two. The result showed significant differences between stressors due to siege according to sex toward males (Males vs. Females) (Mean=9.43 vs. 8.81) (t (378)=2.25, p<0.02). Post Hoc test using Tukey test showed that there were significant differences between the total means of stressors due to siege according to the number of children toward patients with number of children ranged from 5-7 (F (2/379)=3.745, p=0.02). The results showed that there were significant differences between the total means of stressors due to siege according to family income towards those who have family income less than $300(F (3/379)=7.96, p=0.001).
Depression in patients with cancer
As shown in Table 4, 7.7% of patients had no depression, 15% had mild depression, 53.4% had moderate depression, and 24.2% had severe depression (Table 4).
Table 4. Prevalence and level of depression.
| Depression |
N |
% |
| No depression |
28 |
7.4 |
| Mild to moderate |
57 |
15.0 |
| Moderate |
203 |
53.4 |
| Severe depression |
92 |
24.2 |
Differences in depression and other sociodemographic variables
There were significant differences in mean depression scores toward female patients (t (378)=10.08, p≤0.001). Post hoc test showed that there were significant differences in depression scores toward families with monthly income less than $300 (F(3/379)= 4.196, p=0.006) (Figure 1).
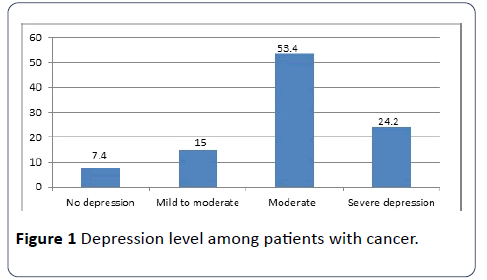
Figure 1: Depression level among patients with cancer.
Prevalence of anxiety symptoms
The study showed that the commonly reported anxiety symptoms among cancer patients were; being tense and restless (61.3%), had insomnia (56.3%), had cardiovascular symptoms (51.1%) and worried (50%).
Prevalence of anxiety among cancer patients
The results showed that 19.7% of patients had no anxiety, 21.3% had mild to moderate anxiety, and 58.9% had severe anxiety. There were statistically significant differences in level of anxiety toward female patients (t (378) =23.1, p<0.001).
Differences in anxiety and other socioeconomic variables
The result showed significant differences between anxieties according to sex toward female patients (Males vs. Females) (Mean 22.71 vs. 28.40) (t (378)=5.54, p< 0.001).
Also, the results showed that there were significant differences between the total means of anxiety according to family income towards those who have family income less than $ 300 (F (3/379)=5.06, p=0.002).
Relationship between stressors due to the siege, depression and anxiety
Pearson correlation test showed that there were statistically significant positive relationship between total stressors due to siege and depression symptoms (r (379)=0.27, p<0.001) and anxiety (r (379)=0.14, p <0.01). Where there were significant relationship between the depression and anxiety (r (379)=0.27, p<0.001).
Prediction of depression by stressors due to siege
In a multivariate regression model, each stressor due to siege was entered as an independent variables and total depression as dependent variable. I went to Zaka organizations and other organizations to get the food (β=0.19, t(380), p<0.001) was predicting depression, I feel I am in a big prison, my monthly income decreased and cannot send my children for schools (β=0.16, t(380), p<0.001), one of the family member died due to prevention of traveling for treatment (β=0.11, t(380), p<0.02), R2=0.10, F (1, 380)=11.02, p<0.001.
Prediction of anxiety by stressors due to siege
In a multivariate regression model, each stressor due to siege was entered as an independent variables and total anxiety as dependent variable. One of the family members died due to prevention of traveling for treatment was predicting anxiety (β=0.13, t(380), p<0.001).
I sold some of my furniture and my wife's gold (β=0.14, t(380), p<0.001), I had suffering of not able to receive proper medical care due to shortage of medicine (β=0.19, t(380), p<0.06). I went to human rights organizations and other organizations to get the help for travel outside Gaza for treatment (β=0.10, t(380), p<0.02), I stopped completely working due to inability to go to my land and restriction in sea area (β=0.12, t(380), p<0.001), my work affected so much due to cut-off of electricity and shortage of gas (β=0.16, t(380), p<0.01), I cannot travel for treatment and work (β=0.13, t(380), p<0.01), I went to Zaka organizations and other organizations to get the food (β=0.11, t(380), p<0.01), R2=0.15, F(1, 380)=8.37, p<0.001.
Discussion
The most common reported stressors due to siege were : 92.9% said prices are sharply increased due to closure, 90.3% said they feel that they are in big prison , 85.5% their work affected so much due to cut-off of electricity and shortage of gas. The researcher hypothesized that for dangerous effects of siege that destroyed everything in Gaza strip including but not limited to political, social, cultural and economic aspects. The expandable siege that blocked everything put Gaza under collective punishment against every Palestinian. While, Thabet et al. [16] found that the most common stressful situations due to blockade identified during the study are: General feeling of living in a big prison; The inability to finish construction and repair work in people’s homes due to a chronic shortage in cement and building materials; The sharp increase in prices in commodities in recent years; The inability to upkeep social and family relationships, including social and religious visits to the West Bank/East Jerusalem; The negative impacts on daily life and work due to repeated cut-off of electricity and shortage of gas and fuel. However, the results of the current study appeared to be consistent with the study of Thabet [15] that found the most common items of siege checklist; learning problems due to shortage of electricity and teachers unable to come schools 82.6%; I feel I’m in a big prison 79.3%; I was not able to go to school due to shortage of fuel and absence of transportation 75%; I can’t find some of the necessary things for study such as books and stationary 68.5%. Also, the study of Lubbad et al. [23] in study of university students in Gaza Strip showed that the most common siege items; we can’t finish some construction and repair work in my house due to shortage of cement and building material 97.4%; one of the family member died due to prevention of travelling for treatment 86.2%; we cannot find some of the necessary things for children 86.2%; I feel I am in a big prison 78.3%; shortage of fuel, papers, medicine, row material 77.3%; social visit less than before 75.3%.
Moreover, Qouta [24] found that the Israeli siege pushed around 84% of Palestinian families to change the patterns of their lives; 93% of them gave up their daily living requirements; 95% said they live in big prison; 47% of patients in Gaza are not able to get the medicine they needed; 38% not receiving medical services; reduction in social visits 79%; 95% of the citizens could not find the objects and goods that they were looking for; while the prices rose 99% as the income of citizens were reduced with 68%; 45% of whom were fired from their jobs; moreover, 77% of the workers were suspended of their jobs in the construction sector. The result found significant differences between stressors due to siege according to sex toward males of the cancer patients. The researcher attributed these results for dominant gender “males”, since they work, move, travel, buy, and share the society more than females. This reflected on their behavior and mental health more than female. The males have more participation in the community and the Palestinian families dependent on males. This let them experience the stressors of siege more than females. The results of the current study consistent with the results of study of Lubbad et al. [23] university students which found significant differences between stressors due to siege according to sex toward males of the study sample. Our results showed that there were significant differences between the total means of stressors due to siege according to family income towards those who have family income less than $300. We postulated that the families in Gaza Strip were unable to achieve the minimum requirement that needed for their life, but high income families were able to achieve their needs. The results of current study seem to be consistent with the results of Lubbad et al. [23] that found significant differences between the means of stressors of siege and family income toward low family income families.
The study showed that the most common depression symptoms were: discouraged about the future (52.9%) and feel sadness (46.6%), while the least common depression symptom was thoughts of killing self (13.7%). We attributed these results to direct consequences of siege effects that affected the mental health of the cancer patients. The siege has major negative consequences in all life aspects including psychological, social, physical, as well as economic and general life aspects. While, Chen [25] found that the most prevalent symptom in the total sample was insomnia (occurrence rate=67%). Insomnia, pain, anorexia, fatigue and wound or pressure sore occurred significantly more often in depressed patients, with no difference in occurrence rates of nausea/ vomiting and dyspnoea. Also, the results consistent with Qouta [24] found that the increase in the siege status leads to more psychological suffering like being existed, anxiety, depression, hostility and sensitivity. The results consistent with the results of Lubbad et al. [23] that found, the most reported depression symptoms were; tiredness or fatigue 64.5%; sadness 62.5%; guilty feeling 59.2%. Where the lowest depression symptoms were; past failure 8.7%; and self-dislike 11.5%. But, Gogne et al. [26] found a significant correlation was observed between response to neoadjuvant chemotherapy and depression levels in breast cancer patients. Karabulutlu et al. [11] in his study revealed that, depression determined in 81.3% of the cancer patients. A positive, statistically significant relationship was found between the avoidance strategy and depression levels of the cancer patients. Where, Thabet et al. [16] in their study found that most of the study sample reported symptoms of depression included general sad feelings and feeling weak in parts of the body.
The study results revealed 53.4% had moderate depression and 24.2% had severe depression. Such findings may be due to continue siege the imposed by the Israel government on Gaza strip for long time period and reflected on the mental health of the cancer patients. However, Ellis et al. [14] found that the prevalence of significant depression 3.5%. This was higher in younger, female and unmarried patients. Procedure-related worry and pain were generally low. Where, Smith et al. found on the Hospital Anxiety and Depression Scale (HADS)], 15 (22%) were depressed (HADS depression score]/11) among the cancer patients. The results were consistent with the results of Lubbad et al. [23] found that 59.7% have no depression; 37.2% have moderate depression; 3.1% have severe depression. However, Thabet et al. [16] and GCMHP (2007, 2008) reported that , the situation does gravely impact the mental health of the population and the psychological pain the people experience is being manifested in the high levels of domestic, tribal and community violence.
There were significant differences between means of depression and gender among cancer patients in favor of females. The researcher attribute these results to the majority of females who experience cancer and especially breast cancer, breast cancer manifested among females between 20- 59 years old. According to MOH breast cancer is the highest among females and focus in the age group between 20 -59 (MOH, 2014). Furthermore, in Gaza Strip, Health Information System Unit reported that, breast cancer ranked first, with 278 reported cases (19.7%), and considered the highest among females (HISU, 2015). These ratios for breast cancer, but there are other types of cancer that affect females. This give privilege to female cancer patients to experience wide range of siege stressors more than males that affected them because of limited medication, difficulty in transfer and more problems related and lead to depressive symptoms among females. In addition, the current study results were consistent with the study of Ellis et al. [14] found that the prevalence of was female and unmarried patients. Also, the results seem to be inconsistent with the results of Lubbad et al. [23] that indicated significant differences between the means of depression according to sex in favor of males. The results seem to be consistent with the results of Lubbad et al. [23] revealed significant differences between the means of depression and family income toward low income families. But, Gogne et al. [26] found that depression was found to be higher in literate (25, 54.3%) and employed (14, 53.8%) patients.
The study showed that the commonly reported anxiety symptoms among cancer patients were; being tense and restless (61.3%), had insomnia (56.3%), had cardiovascular symptoms (51.1%) and worried (50%). The researcher attributed these results for the siege that affect the life of the general population and cancer patients specifically. The effect of siege stack everyone young or adult, patients or healthy. The exposure to siege reflected on the daily living of the Gaza population. Where, Thabet et al. [16] found that Palestinian parents reported anxiety symptoms such as nervousness or trembling, feeling tense or locked up. Mothers showed similar signs of anxiety and somatization symptoms as fathers did, but at a lesser degree. The study results appear to be consistent with results of Hein found that 92% of the Palestinian children suffer from feeling of insecurity and feel of anxiety and tension due to continuous siege. The results different with results of Lubbad et al. [23] revealed the most common reported anxiety symptoms were; I would like to be happy like others 92.1%; I lost my sleep because of anxiety 86.7%; while the lowest items were; I feel no redness face at all 22.2%; I feel quietness all times 26.3%. However, Al-Jadili et al. [3] revealed that state anxiety was at the highest rank 60.8%, followed by trait anxiety 54.6% among the cancer patients. Where, Karabulutlu et al. [11] in his study revealed that anxiety was determined in 61.5% of the cancer patients. A positive, statistically significant relationship was found between the avoidance strategy and anxiety levels of the cancer patients. While, Smith et al. found that that Seventeen (25%) of patients were anxious [anxiety score]/11 on the Hospital Anxiety and Depression Scale (HADS)]. The results showed that 10.8% of males had no anxiety, 8.2% had mild to moderate, and 14.7% had moderate to severe anxiety. For females, 8.9% had no anxiety and 13.2% had mild to moderate anxiety, and 44.2% of females had moderate to severe anxiety. Our study showed that female patients had more anxiety. The effects of the siege contributed to psychological problems as well as anxiety. However, Lubbad et al. [23] in their study “the impact of the siege on the mental health of university students” reported that, 2% have no anxiety; 39.8% have mild anxiety; 42.3% have moderate anxiety; 15.8% have severe anxiety. Where, Ellis et al. [14] found the prevalence of significant anxiety was 15%. This was higher in younger, female and unmarried patients that appear to be consistent with our results. The results showed that there were significant statistical differences in level of anxiety toward females. We attributed that for emotional feeling of females, since they were more emotional than males and they were more sensitive for the disease itself and for mental health problems they encounter due to siege and life stressors. The results seem to be inconsistent with study of Lubbad et al. [23] that found no significant differences between the means of anxiety according to sex. The results showed that there were significant differences between the total means of anxiety according to family income towards those patients who have family income less than $400. Such low income families strive for achieving their needs in presence of high prizes and absent of goods due to siege. The high class may find their needs and requirements despite of expensive prizes, but the low income families are not able to do so. Such findings consistent with study of families in the Gaza Strip which showed that general psychological symptoms, somatization, depression, and anxiety were significantly higher in families with monthly incomes less than $300/month [16].
Clinical Implications
The results revealed that the majority of the study sample suffering from anxiety and depression due to siege. These results considered critical indicators that must be taken into consideration by the policy makers, researchers and clinicians to establish psychological support department specialized for cancer patients at the treating Centre and should be consult with specialized psychiatrist. To establish periodical appointment and follow up for the cancer patients seeking mental health service and provide frequent psychological support. To provide the cancer patients with a list of recognized community mental health centers and professional counselors for further therapy. Moreover, we had to establish psychotherapy groups for cancer patients inside the hospitals dealing with such target patients. To call the international organization to press and eliminate the siege immediately and improve the life situation in the Gaza Strip. For research, we need more precise and accurate studies that include large group and under the supervision of MOH with cooperation with the psychiatric hospitals with professional researchers. Additional, a need for research to evaluate the effective psychological program for treating anxiety and depression among Palestinian.
Study Limitations
The data collection based on self-report scales, therefore, where some potential reporting bias which may have occurred because of respondents interpretation of the questions or desire to report their emotions in a certain way or simply because of inaccuracies of responses. Furthermore, it found to be difficult to follow up the cancer patients during their transfer from hospital to another or to another clinic.
Conclusion
To live under siege and go ahead in your daily living considered impossible for everyone in Gaza Strip. The siege considered the most extreme case in which the Palestinian people in Gaza were totally isolated and separated from the world. The siege contributed to several problems including; psychological, economic, social, and physical problems. As a result, the individuals were living in critical and overwhelming situations and become nervous, anxious, depressed and fearful in addition to vague future due to continued siege. Furthermore, the continued siege resulted in destruction in the basic life material and complicated the entry of essential supplies and equipment to maintain life that made threat to health. The siege stressors are leading to various problems including; physical, social, psychological, economic problems. The stressors that generated by the siege and war affect the Palestinian people psychological health and generated mental health problems including but not limited to anxiety, depression, stress, fear and nervousness. The devastating and extreme exposure to these stressors will develop long term mental health problems.
19052
References
- Morgantini L (2006) The silence and indolence of the international community. Palestine and Israel articles and press releases.
- Zachariae R, AlHajjar BO, Connor M, Mehlsen MY (2011) Cancer-Related post-traumatic stress symptoms of palestinian breast cancer patients and survivors from the gaza strip: Associations with non-cancer traumatic events and centrality of event. Paper presented at the 13th World Congress of Psycho-Oncology.
- Al Jadili MJ, Thabet AA (2017) The relationship between post-traumatic stress disorder and coping strategies among patients with cancer in Gaza Strip.
- Singh U, Verma N (2007) Psychopathology among female breast cancer patients. JIAAP 33: 61-71.
- Derogatis LR, Fitzpatrick M (2004) The SCL-90-R, the Brief Symptom Inventory (BSI), and the BSI-18.
- Gurevich M, Devins GM, Rodin GM (2002) Stress response syndromes and cancer: Conceptual and assessment issues. Psychosomatics 43: 259-281.
- KangasM, Henry JL, Bryant RA (2002) Posttraumatic stress disorder following cancer: A conceptual and empirical review. Clinical PsycRev 22: 499-524.
- Deimling GT, Kahana B, Bowman KF, Schaefer ML (2002) Cancer survivorship and psychological distress in later life. Psychoâ€ÂÂÂÃÂOncology 11: 479-494.
- ZabaleguiA, Sanchez S, Sanchez PD, Juando C (2005) Nursing and cancer support groups. J AdvNurs 51:369-381.
- DeimlingGT, Wagner LJ, Bowman KF, Sterns S, Kercher K, et al. (2006) Coping among olderâ€ÂÂÂÃÂadult, longâ€ÂÂÂÃÂterm cancer survivors. Psychoâ€ÂÂÂÃÂOncology 15: 143-159.
- Karabulutlu EY, Bilici M, Çayır K, Tekin SB, Kantarcı R (2011) Coping, anxiety and depression in Turkish patients with cancer. European J General Medicine 7: 296-302.
- DenaroN, Tomasello L, Russi EG (2014) Cancer and stress: what’s matter from epidemiology: the psychologist and oncologist point of view. J Cancer Therp Res 3: 3-11.
- Moubayed SP, Sampalis JS, Ayad T, Guertin L, Bissada E, et al. (2015) Predicting depression and quality of life among long-term head and neck cancer survivors. Otolaryngol Head Neck Surg152: 91-97.
- Ellis G, Pridgeon S, Lamb B, Awsare N, Osaghae S, et al. (2015) Psychological distress in out-patients undergoing flexible cystoscopy for the investigation of bladder cancer. J ClinUrol 8: 196-201.
- ThabetAA, Tawahina A, Sarraj AEI, VostanisP (2008) Siege and quality of life of palestinians in the gaza strip. Arabpsynet E J20: 157-164.
- ThabetAA, Thabet S (2015) Stress, trauma, psychological problems, quality of life, and resilience of palestinian families in the gaza strip. JClinPsych 1: 11.
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J (1961) An inventory for measuring depression. Arch Gen Psychiatry 4: 561-571.
- Beck, AT,Steer RA,Ball R, William FR (1996) Comparison of beck depression inventories-ia and-ii in psychiatric outpatients. J Pers Assess 67: 588-597.
- Beck AT, Steer RA, Carbin MG (1988) Psychometric properties of the beck depression inventory: Twenty-five years of evaluation. ClinPsychol Rev 8: 77-100.
- Groth-MarnatG (1990) The handbook of psychological assessment (2 edn.). John Wiley & Sons, New York.
- ThabetAA, Tawahina AA, Sarraj E (2007) Domestic violence and mental health of palestinian women. Arabpsynet13: 137-143.
- Thabet AA, Tawahina AA, Victoria V, Vostanis P(2015) PTSD, depression, and anxiety among Palestinian women victims of domestic violence in the Gaza Strip. BJESBS.
- LubadI, Thabet AA (2009) The impact of siege on prevalence of depression and anxiety disorder among universities students. Arabpsynet EJ 24: 56-66.
- QoutaS, Kassab A (2008) Study on the relationship between the siege, the quality of life and psychological conditions in gaza. Paper presented at the “Siege and Mental Health Walls vs. Bridges International conference organized by GCMHP and WHO Gaza, Ramallah, Palestine.
- Chen ML, Chang HK (2004) Physical symptom profiles of depressed and nondepressed patients with cancer. J Palliat Med 18:712-718.
- Gogne A, Khandelwal R, Tandon M, Jain S, Kumar Y, et al. (2011) The correlation of anxiety and depression levels with response to neoadjuvant chemotherapy in patients with breast cancer. JRSM 2: 15.

